Ultrasound Guided Therapeutic Nerve Blocks
It has long been observed that a simple suprascapular nerve block has a benefit for a variety of shoulder pain conditions. Similarly, a greater occipital nerve block can provide relief to cervicogenic headache and median branch nerve block relieves facet joint pain. It a simple extension of this idea that nerve blocks can be used at other sites to gain pain relief for a variety of chronic painful soft tissue conditions. When patients present with such painful soft tissue problems, commencing a procedure with a nerve block, will make the injection procedure less painful and will have a longer-term additional benefit in pain relief.
Introduction
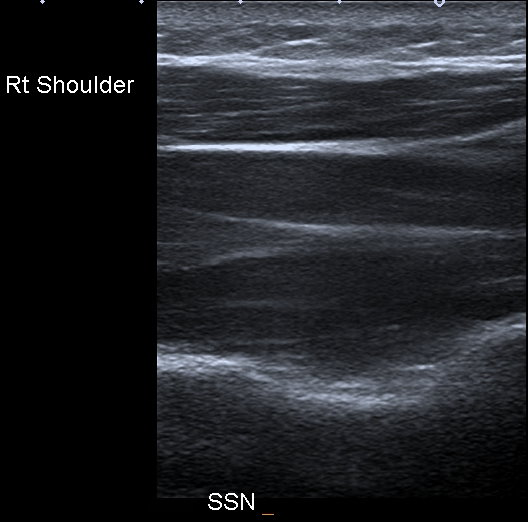
In 1989, Emery et al showed that a suprascapular nerve block has a benefit in relieving shoulder pain in patients with rheumatoid arthritis [1]. This has been confirmed in several studies since and including a variety of shoulder pain conditions such as arthritis, frozen shoulder rotator cuff tendinopathy and perishoulder pain in general [2]. The procedure is much more effective and safer when it is done under ultrasound guidance [3, 4]. With ultrasound, the suprascapular nerve can be identified as a posterior branch of the brachial plexus, but it most easily found deep to the supraspinatus muscle belly in the superior scapular notch.
The typical inverted dome of the notch is easily imaged and allows accurate targeting of the nerve, as shown in Figure 1. There is an accompanying artery which makes it easy to find with color Doppler. While injecting this region, patients often experience neural type pain radiating around the shoulder.
Similarly, a nerve block of the greater occipital nerve is of benefit in patients with cervicogenic headaches. With ultrasound, the nerve is most easily located between the trapezius muscle and oblique inferior capitus muscle.
In both cases, the injection has no effect on the primary pathology but lessens the pain that the patient suffers, usually for many months. Understanding how this works can benefit from a brief overview of the pathophysiology of peripheral nerves in chronic pain.
Pathophysiology of Pain
The initiating event is soft tissue/bone injury. In athletes this can be:
- acute injury
- repeated stress
- chronic recurrent injury With this tissue injury there is a release of inflammatory and pain mediators. This cascade of mediators results in greater and more frequent transmission of action potentials to the pain neurons than in ‘normal’ pain responses. This is known as peripheral sensitisation. Next, at the synapse level, these sensitised pain fibres have a decrease in the threshold for activation so becoming hyperexcitable and transmit more frequent action potentials. This is known as hyperexitation. The effect of this is that the patient perceives pain in response to stimuli that are not normally painful, such as a light stroking of the skin, vibration or bumping. This is known as allodynia. In addition, the individual perceives abnormally high levels of pain in response to light painful stimuli. Patients may also perceive spontaneous pain. All the above result in pain transmission along the nerves being more frequent (sometimes continuous) and of a greater magnitude. This is known as wind-up. As a result of the above mechanisms the receptive field will also expand so the patient feels the pain over a larger region [5].
If there is damage to peripheral nerves, there can be a component of neuropathic pain. Accumulation of sodium channels generates action potentials in the damaged pain fibres proximal to the injury site. This is known as ectopic activity and results in hyperexitability and spontaneous pain. If there is complete severance of a nerve fibre, adjacent normal nerves will transmit pain signals. This is known as cross talk, and it leads to the receptive field expanding.
The resulting effect for the patient of all the above mechanisms is that:
- The perceived pain becomes worse
- Light painful stimuli are perceived as worse pain
- Non painful stimuli are perceived as pain
- There can be spontaneous pain
- The region of perceived pain expands The exact mechanism by which a therapeutic nerve blocks alleviates these features is not known. In my experience adding a therapeutic nerve block to a chronically painful soft tissue condition results in better overall long- term relief of pain.
Clinically Useful Nerve Blocks
I have already discussed the suprascapular nerve block for shoulder pain. I find it is particularly helpful for frozen shoulder where it makes hydrodilatation much less painful than it otherwise would be.
Plantar fascia
One of the particularly painful injections we do in clinical practice is for plantar fasciitis. Under ultrasound it is less painful to inject from the medial side of the foot and to run the needle parallel to the sole of the foot. This also makes it easier to inject deep to the fascia. For a painful plantar fascia, I do a posterior tibial nerve block. I place the foot externally rotated which is the position I use for the actual injection. I then search for the posterior tibial nerve just above the malleolus. It is slightly variable in its relation to the accompanying veins. Ideally, I target the nerve where it is clear of the overlying veins, and I infiltrate steroid and local anaesthetic around it. If you target too low, you can miss the calcaneal branch which it is important to include in the nerve block. Usually there is incomplete anaesthesia of the skin but good anaesthesia of the deep tissues.
Medial epicondyle
This is supplied by the ulnar nerve. The ulnar nerve is best located several centimeters above the elbow at the inside portion of the upper arm. The ulnar nerve lies just under the skin, medial to the triceps muscle belly. If you are having trouble locating it you can find it in the olecranon groove and follow it back up the arm. It is important to target the nerve several centimeters superior to the elbow to include the branches of the nerve which supply the medial epicondyle
Lateral Epicondyle
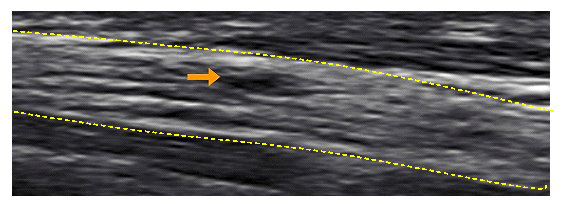
This region is supplied by the radial nerve. It is easily located several centimeters above the elbow where it lies adjacent to the lateral humerus as shown in Figure 2. This is the easiest location to find it and inject it as it does not move away from the needle as it is pinned against the bone. It then moves medially and superficially as it progresses down past the elbow where it braches into posterior interosseos nerve (PIN) and superficial radial nerve. People who are used to locating it at this site to assess the PIN can find it here and then follow it back up the arm.

Greater Trochanter Pain syndrome
The nerve supply to this area is complex. The bursa is supplied by the inferior gluteal nerve and the gluteus medius and minimus tendons are supplied by the superior gluteal nerve. I find the most effective block is to block the superior gluteal nerve, which supports the idea this is primarily an enthesopathy and not a bursitis. The superior gluteal nerve has an accompanying artery which helps with its location. It emerges from the pelvis in the sciatic notch and then lies between the gluteus minimus and medius muscle bellies in the region of the muscular tendinous junction. It is seen with ultrasound in the concave space between the two muscles. It is important to scan as posterior as possible. In some obese patients this region is very deep and it is important to use a needle long enough to reach this region. Follow up from our referring doctors has been that we are achieving much better analgesia in these patients since we have added the nerve block.
Deep buttock pain
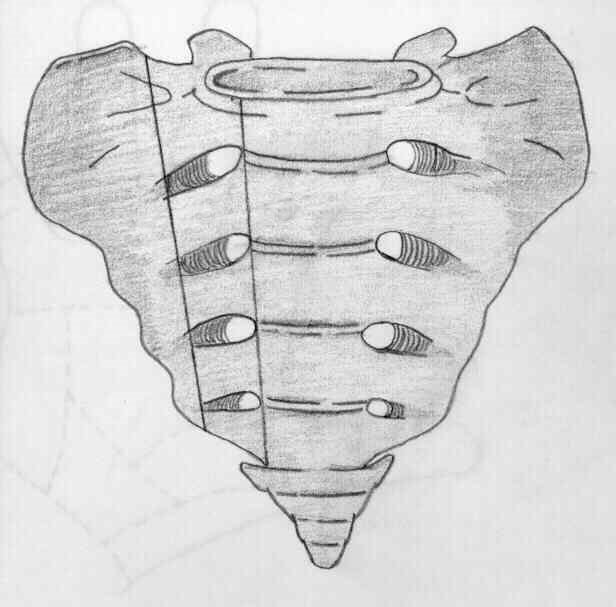
We commonly see patients with mixed hamstring pathology and pathology to the deep rotators of the hip (i.e. the piriformis, superior/inferior gemellus, obturator internus and quadriceps femoris) these small muscles are very hard to treat and can be quite disrupted. We have not found a good way to provide relief of pain until we started doing a therapeutic nerve block. I block the L5, S1, S2 and S3 nerve roots on that side. Under ultrasound the sacral foramina are seen as small holes in the sacrum. They lie in a peri-sagital line just lateral to midline and slightly oblique as shown in Figure 3. The sizes are variable and sometimes very small. I approach the foramen from directly above to be able to insert the needle into the foramen, which is important to be able to block the deep nerve roots which are the target. If the block is done properly there will be complete anaesthesia of the patient’s buttock pain after it is done.
Other regions I have treated with nerve block include
Chronic testicular pain – I inject in the cremasteric bundle. There is a very generous nerve supply to the testes and it is important to inject within and around the cremasteric bundle.
Pelvic pain. I inject the pudendal nerve deep to the sacro- tuberous ligament. The nerve lies just medial to the artery which is easily located with color doppler.
Athletic pubalgia. I inject the genitofemoral, ilioinguinal and iliohypogastric nerve around the medial inguinal ligament. Knee pain. I inject the geniculate nerve in the medial thigh.
Compression Neuropathy
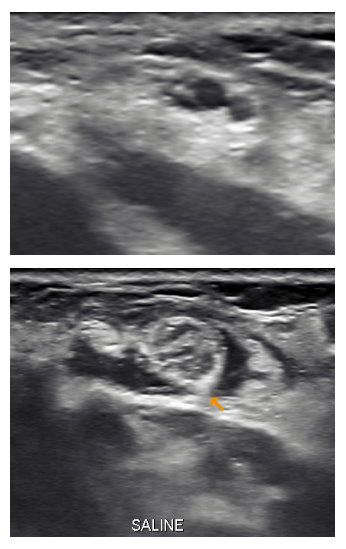
Some patients we see have a compression neuropathy. As well as injecting steroid around the nerve I will try and fix the problem by using the volume of the injection to stretch the tissues off the nerve. Common sites we see in the upper limb are the brachial plexus, the PIN in the supinator canal, the ulnar nerve at the ebow or wrist and the carpal tunnel. Sites we see in the lower limb include: the sciatic nerve, the obturator nerve, the lateral peroneal nerve and the posterior tibial nerve at the tarsal tunnel. In the trunk sites include the lateral femoral cutaneous nerve and the ilioinguinal nerve. In all cases I will attempt to stretch the tissues off the nerve, or if there is a thick fibrous epineureum, then stretch this off the nerve. Post injection the nerve often enlarges in cross section area showing a ‘released spring’ effect, confirming it was under compression. This can be seen in Figure 4. If the nerve is under long segmental compression from scar tissue or fibrosis, I will increase the volume injected by adding 5 – 20ml of saline. This is shown in figure 5. The volume I use depends on the site and the amount of fibrosis I need to treat. I use ice cold saline as it has a local anaesthetic effect, and the cold induced vascular spasm helps prevent bleeding from the soft tissues being hydrodissected.
Nerve Injury
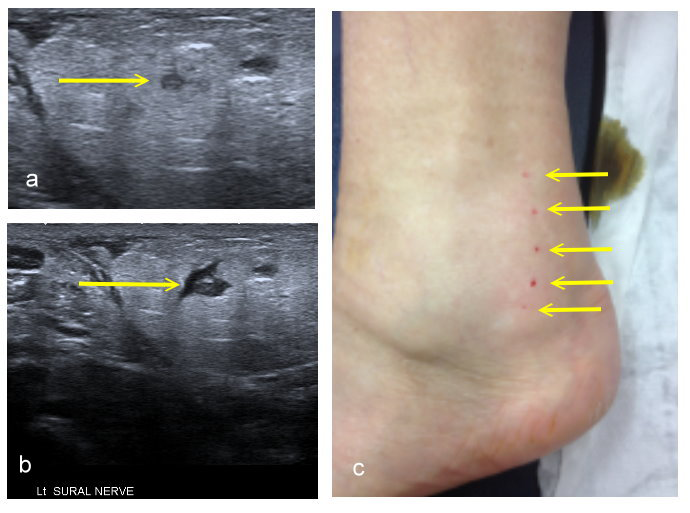
I deliberately try never to inject into a nerve because of the risk of injury to nerve fascicles. As opposed to a relatively simple injury caused by a sharp needle cut, intraneural injection has the potential to create structural damage to the fascicles that is more extensive and less likely to heal. An example of this is shown in Figure 6. The consequence of sensory and motor loss after injection of various agents into peripheral nerves has been well documented. Nerve with large fascicles are more likely to sustain fascicle injury than nerve with multiple fascicles where it is more difficult to inject into the fascicle. Injecting into a fascicle causes mechanical destruction of the fascicular architecture and sets into motion a cascade of pathophysiologic changes. These include inflammation, cellular infiltration, axonal degeneration, and others, all leading to nerve scaring. The extent of actual neurologic damage after an intrafascicular injection can range from minimal structural damage to severe axonal and myelin degeneration. This leads to increased excitability and the development either of acute or chronic neural pain.
The degree of neural damage is categorized by the terms neurapraxia, axonotmesis, and neurotmesis. The mildest form, neurapraxia, denotes a mild degree of neural insult with failure of impulse conduction across the affected segment. Usually when the offending cause has been removed, recovery occurs over a variable amount of time that may be as long as several weeks. Complete recovery can usually be anticipated. Axonotmesis, an intermediate injury, occurs when there is axonal disruption with preservation of the endoneurium. Recovery is dependent on the rate of axonal regeneration (1-3 mm/day). If recovery occurs, it is most likely to be prolonged and incomplete. The prognosis is better for young, healthy patients with distal lesions. The most severe form of neural injury is neurotmesis; a complete transection or crushing of the nerve with disruption of the endoneurium. Surgical repair is usually indicated, but even then, recovery is usually incomplete. Prognosis for full recovery is poor.
Using ultrasound guidance rather than just blind injection from cutaneous landmarks maximizes the chance of a safer injection without traumatizing the nerve or adjacent vascular structures.
Conclusion
When patients present with chronic painful soft tissue problems, commencing a procedure with a nerve block, will make the injection procedure less painful and may have a longer-term additional benefit in pain relief. Using ultrasound guidance for the nerve block ensures a more accurate injection, minimising the chance of a ‘missed’ nerve block and minimising the chances of traumatising the nerve.
References
-
Emery P, Bowman S, Wedderburn L, Grahame R. (1989) Suprascapular nerve block for chronic shoulder pain in rheumatoid arthritis. BMJ 299(6707): 1079–1080.
-
Chan CW, Peng PW. (2011) Suprascapular nerve block: a narrative review. Reg Anesth Pain Med 36(4): 358–373.
-
Harmon D, Hearty C. (2007) Ultrasound-guided suprascapular nerve block technique. Pain Physician 10(6): 743–746.
-
Abdelshafi ME, Yosry M, Elmulla AF, Al-Shahawy EA, Adou Aly M, Eliewa EA. (2011) Relief of chronic shoulder pain: a comparative study of three approaches. Middle East J Anesthesiol 21: 83–92.
-
American Medical Association (2013) AMA module 1 Pathophysiology of Pain and Pain Management. American Medical Association, USA.
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage
- Effect of Contrast Agents on Pregnant Women