Glycemic Variability in Diabetic Patients Adding Canagliflozin 300Mg to their Underlying Treatment
Background: The kidney is vital for the regulation of glucose. Sodium-glucose co-transporter-2 (SGLT2) receptors are located in the initial portion of the proximal tubule and are responsible for 80–90% of total glucose reabsorption. SGLT2 inhibitors are a new class of drugs tested to treat type 2 diabetes mellitus (DM) patients; their objective is to control glucose in an insulin-independent manner, viaglycosuria. Objective: This study aimed to determine the effects of oral canagliflozin on plasma glucose levels, in patients with T2D that is inadequately controlled by standard therapy. The drug was administered at a dose of 300 mg every 24 hours, and plasma glucose levels were being measured using the iPRO2 system.. Materials and methods: This is a pilot, prospective, and longitudinal study. Patients with uncontrolled diabetes determined by blood glucose and glycosylated hemoglobin levels> 7% were recruited, with no modification of treatment dosage (oral hypoglycemic agents or insulin treatment) in the previous 3 months. Blood pressure and somatometric measurements were obtained and recorded.300mg of canagliflozin was then added to their antidiabetic regimen. Patients were monitored using the iPRO2 system, and metabolic control was determined3 months after initiation of treatment. Results: A total of 26 patients were included in the study. Results shown normal distribution, analyzed by ANOVA, with and statistical significance at: HbA1c (p < 0.001), BMI (p < 0.001), and blood pressure (p < 0.05). Conclusion: Glycemic control is improved in diabetic patients when treated with Canagliflozin 300 mginsulinindependent correction of glycemic levels, demonstrated by iPRO2 monitoring.
Introduction
In the early 1970s, Vick, Diedrich, and Bawman demonstrated that the reabsorption of blood glucose occurs in the proximal tubule through the activity of sodium-glucose co-transporters (SGLT) 1 and 2 [1, 2]. Florizin was the first SGLT inhibitor identified; it is obtained from the bark of apple trees and induces glycosuria, and therefore helps to normalize blood glucose levels. However, it does not distinguish between SGLT 1 and 2, and also affects the gastrointestinal tract. Therefore, the synthesis of an SGLT2-specific inhibitor was required, with an improved absorption rate, increased bioavailability and fewer adverse effects [2, 3]. SGLT 1 and 2 are responsible for glucose reabsorption through the kidney, therefore inhibition of these co-transporters should induce glucose excretion in the urine [4, 5]. Both co-transporters are located in the proximal tubule: SGLT2 is located in the first portion of the proximal tubule and is responsible for the reabsorption of 80-90% of filtered glucose in the kidney. SGLT1 is located in the distal portion of the proximal tubule and is responsible for the reabsorption of the remaining 10-20% of the filtered glucose [3]. SGLT1 is also expressed in the intestines, heart and lung, while SGLT2 is expressed almost exclusively in the kidney.1 SGLT2 inhibitors are a new class of drugs approved for the treatment of type 2 diabetes (T2D), which aim to control glucose in an insulin-independent manner. This is done by inducing glycosuria, which is caused by the decrease in the transport maximum (Tm) and the reduction of the blood glucose threshold concentration [3, 4, 5]. The rate of glucose excreted by the urine increases in a linear fashion when it surpasses the Tm or renal elimination threshold (180mg/dl) [3, 4]. The therapeutic effects of SGLT2 inhibitors include the inhibition of glucose reabsorption, thus reducing glycosylated hemoglobin (HbA1c) levels; weight loss, as 80-120 g glucose is excreted daily in urine, corresponding to a caloric loss of 320-480 kcal/day; and a decrease in systolic blood pressure, as urinary glucose excretion leads to osmotic dieresis [1, 3, 4, 5]. Other indirect effects of SGLT2 inhibition are the reduction of glucotoxicity, increased pancreatic beta cell function, and a tendency towards hepatic glucose sensitivity, as well as peripheral sensitivity to insulin [6, 7], probably as an indirect effect of glycemic control and reduction in glucotoxicity. The efficacy of SGLT2 inhibitors has been demonstrated by the consistent reduction in HbA1c levels, both when used as monotherapy and in combination with other antidiabetic agents [1]. Approved SGLT2 inhibitors have been shown to reduce both fasting and postprandial glucose levels, blood pressure (particularly systolic pressure), and body mass index by inducing weight loss [8]. They therefore provide beneficial effects in populations with a high obesity index and high rates of morbidity and mortality, that are often at risk of conditions such as cardiovascular disease [2, 3, 5, 9]. In addition, it is noteworthy that the tendency of other antidiabetic agents (such as insulin, sulfonylureas, and thiazolidinediones) to promote weight gain can be mitigated, by adding SGLT2 inhibitors to the treatment regime of patients that require additional therapy to achieve their therapeutic goals [1, 10].
Objectives
This study aims to assess the effects of once-daily canagliflozin 300 mg therapy on plasma glucose variability assessed as standard deviation in patients with inadequately controlled type2 DM in a real clinical setting. Data will be measured using glucose continuous ambulatory monitoring system iPRO2, changes in HbA1c, body weight and blood pressure will be assessed over 3 months.
Materials and Methods
This is a pilot, longitudinal, prospective clinical study of real-world clinical evidence in an outpatient medical center. The protocol was applied to those patients who regularly attend clinical consultation and who require an adjustment to their treatment due to inadequate glycemic control. That is, those with HbA1c levels higher than the control goals of 7%, despite receiving treatment for the previous 3 months without dosage or therapy changes, including metformin monotherapy, a dipeptidyl peptidase IV (DPP-IV) inhibitor, or a combination of both, or basal or multi-dose insulin or sulfonylurea. It is justifiable to modify therapy for these patients, and those who can receive 300 mg canagliflozin according to approved indicators, will be candidates for glucose monitoring with the iPRO2 system. This system will continuously monitor glucose levels in ambulatory patients over a period of 5 days. The Medtronic iPRO2 is a continuous glucose monitoring system that improves the glycemic control of patients with diabetes. This system allows continuous and accurate measurement of fluctuating glucose levels, which normally could not be detected with the HbA1c test. This system also detectshypo- and hyperglycemia and therefore can prevent complications of poor glycemic control [11]. The iPRO2 contains a glucose sensor that automatically performs interstitial glucose measurements and records them continuously in a database. It is easy to use by the patient and allows regular daily activities since the device is placed in the abdomen; it is small, lightweight, waterproof, and the patient is blind to the measurements, so it does not interact directly with it or with the information obtained. After 5 days of using the IPRO2, patients attended a medical consultation to analyze the glycemic control data: the information was obtained using iPRO CareLinkTM software downloaded from the manufacturer's website, and showed the summary of blood glucose levels during the period of use [11]. The database was compared to the patients’ data online, and was reported using follow-up charts and continuous evaluation, as well as reports of hypo- and hyperglycemic events, and substantial changes caused by physical activity, stress, and food intake. The report given by the software was also useful for patient education and motivation, as it allowed patients to review in a comprehensive manner the integrated blood glucose levels and fluctuations in different situations. Patients who participated in the study voluntarily accepted the placement of the iPRO2 device and were asked to maintain a continuous review of capillary glucose levels on four occasions per day: stating whether this was three meals per day, with a fast in the morning. They were also asked to write down a list of the daily food they consumed, they were to be notifying by telephone in the case of hypoglycemia or any other complication. On the third day of iPRO2 placement, patients were instructed to take canagliflozin 300 mg tablet 20 min before the first meal of the day, and to continue with this treatment unless instructed to discontinue by the attending physician.
Selection Criteria
Inclusion criteria: Men and women with type 2 DM and prior unmodified treatment in the previous 3 months; whose previous treatment is one of: metformin, DPP-IV inhibitor, or both in combination; insulin; sulfonylurea; diet; or glucagon-like peptide type 1 receptor analog (GLP-1); with HbA1c levels > 7%; who regularly attend a physician; who show an adequate attachment to their previous pharmacological treatment; and who are aged between 18 and 75 years. Exclusion criteria: Patients who do not accept the indicated treatment; pregnant or lactating women; those with a glomerular filtration rate <45ml/min calculated by MDRD; those with a medical history of Child-Pugh C hepatic disease, intestinal malabsorption syndromes, or inflammatory bowel disease; those who have suffered a cardiovascular event in the last 3 months (acute myocardial infarction, acute coronary syndrome, unstable angina, angioplasty or bypass);those who previously suffered a cerebrovascular event, transient ischemic attack, or pulmonary thromboembolism; or those who are participating in another clinical trial, or have participated in the last 30 days before attending the doctor’s office. The iPRO2 system was withdrawn on the fifth day and patients continued with the indicated treatment, attending clinical visits according to their personal care standards. This study evaluated HbA1c levels, body weight, and blood pressure parameters, which were measured 3 months after the initiation of canagliflozin treatment.
Statistical Analysis
SPSS software version 20.0 (SPSS, Inc., Armonk, NY) was used for statistical analysis. A descriptive statistical analysis was performed for quantitative variables, reporting measures of central and dispersion tendency. Frequencies and percentages were obtained for qualitative variables. Quantitative comparative variables were reviewed for distribution, using the Shapiro-Wilk test to determine normality, ANOVA for repeated samples in the case of measured variables with the iPRO2, or the Friedman’s test in order to compare baseline values with endpoint values after 3months of canagliflozin treatment. We used Student’s t-test for related samples or the Wilcoxon signed-rank test. A p value of <0.05 was considered statistically significant.
Results
A total of 26 patients participated (14 women and 12 men), aged between 18 and 78 years (average 54.2 years); with diabetes duration ranging from 4 months to 36 years (average 11.43 years). Previous treatments were as follows: 13 patients treated with insulin, two with metformin, one with GLP-1ra, one with DPP4i, four with metformin and DPP4i in combination, two with sulfonylurea, and one with diet. HbA1c levels ranged between 7.4-14% (average 9.26%); BMI from 21.15- 57.04 kg/m2 (average 30.36 kg/m2); serum creatinine levels from 0.4-0.6 mg/dl (average 0.9mg/dl); glomerular filtration rate (GFR) between 50-297 ml/min (average 110.9 ml/min); systolic blood pressure between 110-160 mmHg (average 135 mmHg), and diastolic blood pressure between 70-95 mmHg (average 84.68 mmHg).
The iPRO2 system was placed for 6 days; during the last three days, 300 mg of canagliflozin was added to patients’ usual treatment before the first meal of the day, and daily charts were registered for 5 days through iPRO2 software. Patients attended the doctor’s office three months later. Two patients did not complete the study: one had a urinary tract infection and discontinued treatment, and one used the treatment within 3 days of the protocol, voluntarily discontinued treatment, and died of myocardial infarction due to diagnosed arrhythmia 2 months after protocolinitiation. HbA1c levels after treatment with canagliflozin ranged from 5.2 to 9.5% (average 7.2%); BMI between 19.81-53.5 kg/m2 (29.31 kg/m2 average); serum creatinine between 0.4-1.3 mg/dl (0.83 mg/dl average); GFRbetween 42-318 ml/min (117.6 ml/min average); systolic blood pressure between 100-160 mmHg (118 mmHg average), and diastolic blood pressure between 70-90 mmHg (79.2 mmHg average). The results of the effects of once-daily canagliflozin 300on glucose variability measured as SD in patients with inadequately controlled type 2 DM, showed non- statistically significant difference in day 5 of the protocol (p=0.09) between Day 0 and subsequent days.
For mean glucose values at each patient, there was a difference of -27.56 (p= 0.11) (Figure 1), and thehypoglycemia events reported (p=0.11 and p=0.45, respectively, see Table 1).
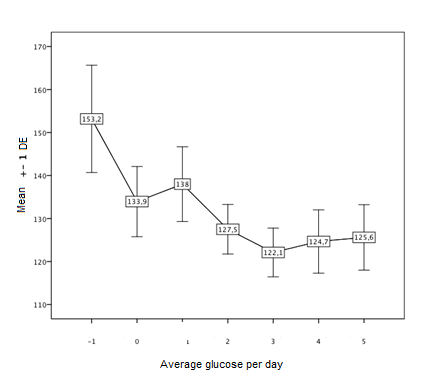
| Day-1(n=22)Mean(ED) | Day 0(n=22)Mean(ED) | Day 1(n=22)Mean(ED) | Day 2(n=21)Mean(ED) | Day 3(n=22)Mean(ED) | Day 4(n=21)Mean(ED) | Day 5(n=18)Mean(ED) | P | |
| Standard Deviation (SD) | 25,11(15.02) | 32,11(22.39) | 30,11(20.82) | 24,72(12.67) | 25,33(14.35) | 27,44(20.25) | 24,56(22.6) | 0.09 |
| Glucose | 153,17(52.9) | 133,94(34.6) | 138(36.8) | 127,5(24.4) | 122,1(24) | 124,67(31.2) | 125,61(32.2) | 0.11 |
| Excursions | 1,22(1.1) | 2,56(1.6) | 1,94(1) | 2,50(1.3) | 2,00(1.3) | 1,67(1.3) | 1,33(1) | 0.08 |
| Hypoglycemia | ,06(.23) | ,56(.70) | ,11(.32) | ,33(.84) | ,33(.59) | ,22(.42) | ,17(.38) | 0.45 |
| T rango | 52,29(41.17) | 63,24(31.11) | 65,18(32.83) | 69(26.52) | 73,35(24.89) | 72,88(28.76) | 70,82(29.13) | 0.63 |
Table 1: Daily glucose measurements with iPRO2.
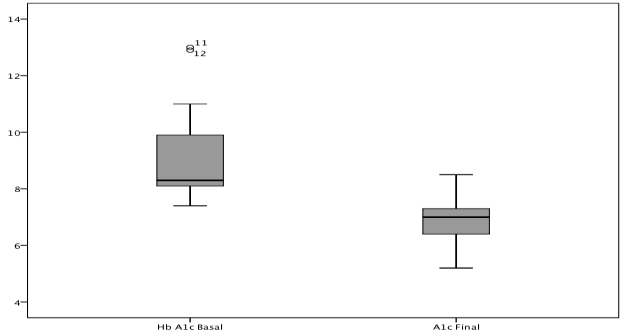
Table 1: Daily glucose measurements with iPRO2. Changes in HbA1c levels after 3 months of canagliflozin treatment were studied (Figure 2), a -1.2% reduction of HbA1c (p <0.001) was observed, with a median decrease of 8.3% (range 8.1-10.3%) at baseline, and a final value of 7.1% (range 6.6-7.5%, see Table 2). Decreased BMI and blood pressure were also observed: these decreases were statistically significant (p <0.05).
| Study Population | Basal | Final | *p |
| Study Population | n=25, median(q1-q3) | n=25, median(q1-q3) | |
| HbA1c | 8.3(8.1-10.3) | 7.1(6.6-7.5) | <0.001 |
| BMI | 28.2(25.9-33.3) | 27.7(24.8-31.7) | <0.001 |
| Systolic blood pressure | 140(120-147.5) | 130(120-140) | 0.03 |
| Diastolic blood pressure | 85(80-90) | 80(70_85) | 0.02 |
| Basal creatinine | 0.9(0.8-1) | 0.8(0.7-1) | 0.28 |
| GFR | 100(69.5-117) | 102(74-147) | 0.13 |
Table 2: Comparative evaluation after 3 months of treatment with canagliflozin.
HbA1c: Glycosylated hemoglobin, BMI: Body Mass Index, GFR: Glomerular filtration rate obtained by MDRD, n: Number of patients, Q1 - Q3: Quartile 1 and quartile 3, * Wilcoxon rank test. Table 2: Comparative evaluation after 3 months of treatment with canagliflozin. Although our studied population was small, the change in HbA1c over time was very significant incanagliflozin-treated patients: a difference of -2.3% was observed in 13 patients using insulin; and of -2.2% in the 5 patients using DPP-IV inhibitors.
Discussion
In our study, the results for body weight changes and serum glucose levels are promising and consistent with the worldwide literature [12]. The addition of a 300-mg daily dose of SGLT2 inhibitor (canagliflozin), either in dual oral therapy or added as dual therapy to insulin [7], improves multiple systems in patients with uncontrolled diabetes. This includes direct action at renal level system in the proximal tubule, as well as effects on indirect receptors of the glucose transporter in other organs such as the gut [2, 3, 6, 13]. In the presence of SGLT2 inhibitors, the renal homeostatic mechanism allows a reduction in HbA1c, as well as an absence of sporadic glycemic peaks during the treatment. This latter effect decreases glycated formations and systemic cellular deposits in the long term, with a subsequent reduction in blood glucose and HbA1c levels [14, 15]. In our study, serum glucose levels tended to decrease, the figures obtained for blood glucose would have an impact, as reported globally in clinical trials. The model for adjust HbA1c can be applied, because it is significance glucose after apllyment [16]. This would therefore be beneficial to patients with diabetes with poor therapeutic control, by decreasing their risk of cardiovascular disease, which is the main cause of morbidity and mortality in these patients [10]. Hayward et al. showed that strict control of serum glucose levels, for 12 years in patients with type 2 DM, led to a decrease in HbA1c values of up to 1.5% in the first 5 years of the intervention (mean figures of 6.9% versus 8.4%).As above, the reduction of HbA1c values led to a 17% decrease in the risk of presenting a cardiovascular event, compared to patients with standard glycemic control. These factors were especially beneficial in patients over 55 years of age [17]. With the addition of 300mg canagliflozin, additional benefits were reported, such as weight loss [8] and decreased blood pressure: this was secondary to the insulin-independent mechanism [18]. If glucose exceeds the threshold of ~90 mg/dl glycosuria is present which leads to a diuretic effect which also contributes to lowering blood pressure. We also observed body weight changes in our population, as reported in the literature [8]. There is an association between diabetes and being overweight: once patients with diabetes lose weight, it is easier to control their blood glucose levels [19]. In fact, diabetes education and medication are suggested as part of diabetes management to achieve therapeutic goals. Lowering BMI improves metabolic prognosis and required drug dosage [20]. Patients receiving canagliflozin therapy tend to lose up to 4.2% of their initial weight after 26 weeks of treatmen, [5] which corresponds to the findings of our study. This has the additional benefit of decreasing the glucose/insulin ratio, by gutvia mechanism [3, 17]. Research surrounding the intestinal mechanism continues, since body weight loss is not only due to the dosage of canagliflozin, as it affects not only SGLT2 receptors but also the SGLT1 in intestine. Studies such as that by Polidori show a reduction in renal postprandial glucose in healthy patients, regulated by renal SGLT2 and intestinal SGLT1 [3]. Despite the current lack of therapeutic indication, ongoing clinical trials such as CANVAS (Canagliflozin Cardiovascular Assessment Study), whose results will be reported in the next few years, will provide scientific evidence for this therapeutics.
The latest guidelines of the American Diabetes Association (ADA) [14], report that SGLT2 inhibitors have shown vital importance in decreasing cardiovascular risk in patients with diabetes, by controlling glucose peaks as demonstrated by iPRO2 monitoring. This impact, along with the reduction of HbA1c, causes patients with diabetes to moderate their own plasma glucose levels, thus avoiding hyperglycemia and secondly chronic cell damage [21].
Conclusions
Currently, there is a continuous increase in patients diagnosed with diabetes worldwide. A large proportion of patients with diabetes do not achieve glycemic goals with lifestyle modifications and pharmacologic treatment. Current treatment guidelines for patients with T2D recommend the use of SGLT2 inhibitors as an alternative when metformin is not tolerated or appropriate, or as an adjunct when metformin fails to confer adequate glycemic control. SGLT2 inhibitors hold additional promise as antidiabetic agents, since they have the advantage of acting in a component of the pathophysiology of T2Dthat leads to increased renal glucose reabsorption. SGLT2 inhibitors provide increased insulin- independent glycemic control, as monotherapy or in dual therapy with other antidiabetic agents. Hyperglycemia is implicit in type 2 DM and is the main risk factor for microvascular and macrovascular complications. Other abnormalities that manifest in type 2 DM include obesity, hypertension, and dyslipidemia: these factors complicate the management of patients with diabetes and cause predispositionto the development of further complications. UKPDS have showed that for every 1% decrease in HbA1c, there is a 37% reduction in the risk of microvascular complications. However, half of the patients with diabetes worldwide fail to achieve therapeutic goals. Glucotoxicity has been associated with important cardiovascular complications, inflammatory effects, and renal damage. Therefore, it is important to mention that blood glucose control goes beyond maintaining normal fasting glycemic figures, which unfortunately remains as the clinical criterion of control even today, since many hospitals do not have access to Hb1Ac tests. The iPRO2 system detects changes in blood glucose 288 times a day, and an average of 1,600 glucose measurements is obtained within a period of 6 days. This system allows to measure glucose excursions, including its behavior over a period of 6 days and at different times, postprandial changes, and the effects of standard meals. It also allows the identification of hypoglycemic episodes, and identifies whether adding canagliflozin to normal treatment improves glycemic behavior. We can conclude that, despite not obtaining statistically significant change in glucose excursions in the studied patients, canagliflozin induced statistically significant reductions in HbA1c, blood pressure and body weight. This drug may therefore be a useful tool for patients with uncontrolled diabetes, and may reduce the potential for micro- and macrovascular complications.
Acknowledgment
We thanks to Janssen Mexico the support for this work.
References
-
Abdul-Ghani MA, Norton L, DeFronzo RA (2015) Renal Sodium-glucose Cotransporter Inhibition in the Management of Type 2 Diabetes Mellitus. Am J Physiol Renal Physiol 309(11): F889-F900.
-
Mudaliar S, Polidori D, Zambrowicz B, Henry RR (2015) Sodium-glucose Co transporter Inhibitors: Effects on Renal and Intestinal Glucose Transport: From Bench to Bedside. Diabetes Care 38(12): 2344-2353.
-
Blonde L, Stenlöf K, Fung A, Xie J, Canovatchel W, et al. (2016) Effect of Canagliflozin on Body Weight and Body Composition in Patients with Type 2 Diabetes over 104 Weeks. Postgrad Med 128(4): 371-380.
-
Devineni D, Polidori D (2015) Clinical Pharmacokinetic, Pharmacodynamic, and Drug- drug Interaction Profile of Canaglifozin, a Sodium- glucose Co-transporter 2 Inhibitor. Clin Pharmacokinet 54(10): 1027-1041.
-
Lavalle-González FJ, Eliaschewitz FG, Cerdas S, Chacon Mdel P, Tong C (2016) Efficacy and Safety of Canagliflozin in Patients with Type 2 Diabetes Mellitus from Latin America. Curr Med Res Opin 32(3): 427-439.
-
Polidori D, Sha S, Mudaliar S, Ciaraldi TP, Ghosh A (2013) Canagliflozin Lowers Postprandial Glucose and Insulin by Delaying Intestinal Glucose Absorption in Addition to Increasing Urinary Glucose Excretion: Results of a Randomized Placebo-controlled Study. Diabetes Care 36(8): 2154-2161.
-
Inagaki N, Harashima S, Maruyama N, Kawaguchi Y, Goda M, et al. (2016) Efficacy and Safety of Canagliflozin in Combination with Insulin: a Double-blind, Randomized, Placebo-controlled Study in Japanese Patients with Type 2 Diabetes Mellitus. Cardiovasc Diabetol 15: 89.
-
King P, Peacock I, Donnelly R (1999) The UK Prospective Diabetes Study (UKPDS): Clinical and Therapeutic Implications for Type 2 Diabetes. B J Clin Pharmacol 48(5): 643-648.
-
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, et al. (2015) Empaglifozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 373: 2117–2128.
-
Vivian E (2015) Sodium-glucose Co-transporter 2 Inhibitors in the Treatment of Type 2 Diabetes Mellitus. Diabetes Educ 41(S1): 5S-18S.
-
(2016) Medtronic Launches Next-Generation Continuous Glucose Monitoring System for Advanced Diabetes Management in 49 Countries around the World.
-
Fioretto P, Giaccari A, Sesti G (2015) Efficacy and Safety of Dapaglifozin, a Sodium Glucose Contransporter2 (SGLT2) Inhibitor, in Diabetes Mellitus. Cardiovasc Diabetol 14: 142.
-
Stein P, Berg JK, Morrow L, Polidori D, Artis E, et al. (2014) Canagliflozin, a Sodium Glucose Co- transporter 2 Inhibitor, Reduces Post-meal Glucose Excursion in Patients with Type 2 Diabetes by a Non Renal-mechanism: Results of a Randomized Trial. Metabolism 63(10): 1296-1303.
-
Okosun IS, Turbow S, McJenkin K, Monique Davis- Smith Y, Seale JP (2016) Diagnostic Performance of Glycated Hemoglobin for Diabetic Retinopathy in Non-diabetic Overweight/obese African-Americans. Diabetes Res Clin Pract 120: 124-131.
-
Johnson JF, Parsa R, Bailey R (2016) Real World Clinical Outcomes and Patient Characteristics for Canagliflozin treated Patients in a Specialty Diabetes Clinic. Curr Med Res Opin 33(1): 77-84
-
Gerich JE (2010) Role of the Kidney in Normal Glucose Homeostasis and in the Hyperglycemia of Diabetes Mellitus: Therapeutic Implications. Diabet Med 27(2): 136-142.
-
Bays HE, Weinstein R, Law G, Canovatchel W (2014) Canagliflozin: Effect in Overweight and Obese Subjects without Diabetes Mellitus. Obesity 22(4): 1042-1049.
-
Bridges JF, Brignac D, Thomas S, Kent C, Ogbuli M, et al. (2012) Optimizing HgA1C and Glucose Monitorizing Frequency in Patients with Type 2 Diabetes. Med Sci Monit 18(12): CR693-CR697.
-
Hayward RA, Reaven PD, Wiitala WL, Bahn GD, Reda DJ (2015) Follow-up of Glycemic Control and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 372(23): 2197-2206.
-
Guo XH, Yuan L, Lou QQ, Shen L, Sun ZL, et al. (2012) A Nationwide Survey of Diabetes Education, Self-management and Glycemic Control in Patients with Type 2 Diabetes in China. Chin Med J 125(23): 4175-4180.
-
Whalen K, Miller S, Onge ES (2015) The Role of Sodium-glucose Co-transporter 2 Inhibitors in the Treatment of Type 2 Diabetes. Clin Ther 37(6): 1150-1166.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance