Family History of Diabetes Alters the Acute Response to Resistance and Combined Training
Type 2 diabetes (T2DM) has an autosomal genetic transmission pattern and can be hereditary. In this type, glucose transporter genes and insulin secretion may contribute to the genetic of the disease. The objective of the study was verify the effects of a single session of resistance and combined training on hemodynamic and metabolic parameters of individuals children diabetics (CDI). Sixteen subjects were selected. The variables of heart rate, blood pressure and capillary glucose (CG) were evaluated. Exercise sessions were divided into two groups - the Resistance Training (RT) group and the Combined Training (CT) group. Both trainings were composed of three phases: warming up, main phase and cooling down. The RT in its main phase was composed of eight resistance exercises and the CT was composed of 20 minutes of aerobic training and the RT protocol. Wilcoxon test and Kruskal-Wallis test was used, adopting p ≤ 0.05. In intragroup analysis, CDI showed significant reduction in systolic blood pressure (SBP) (125.0±10.0 mmHg vs 110.5±15.9 mmHg p=0.01), diastolic blood pressure (81.5±6.4 mmHg vs 71.2±10.4 mmHg, p=0.007), and (CG) (102.8±16.1 mg/dl vs 92.5±10.9 mg/dL p=0.02) in RT. In the intergroup analysis, CDI showed better results in SBP variables (114.75±11.5 mmHg vs 103.75±9.92 mmHg, p=0.01) and CG (93.8±8.02 mg/dL vs 87.0± 4.97 mg/dL p=0.03) in CT. CDI showed positive results after both trainings. However, they may be at risk of further developing T2DM according to pre-exercise CG.
Introduction
Type 2 diabetes (DM2) has an autosomal dominant genetic transmission pattern, which can be hereditary [1]. In the case of this type of diabetes, genes related to glucose transport, β cell function, and insulin secretion can contribute to the genetic basis of the disease [2].
The increased risk of developing DM2 is related to a positive family history, strongly linked to a sedentary lifestyle and environmental factors [1, 3], individuals with a positive history of DM2 can be identified with an increased risk of developing it, based on available phenotypic markers, fasting glucose levels, blood pressure and / or abnormal lipid levels, overweight and the family history itself [4].
For these individuals predisposed to DM2, lifestyle modification can help to reduce this risk 3, it is recommended to participate in structured programs that emphasize changes in lifestyle, which include moderate weight loss and physical exercise (150 min / week), with reduced calorie food re-education in addition to decreased fat intake [5].
Currently, studies have linked abnormal hemodynamic changes at rest, during or after physical exercise with a higher risk of developing cardiovascular disease and DM2, in addition to these changes being a predictor for higher risk of mortality [3, 6].
Early detection of metabolic and / or cardiovascular changes at rest and in response to physical exercise is important for the prevention of DM2 in individuals with a positive family history for this disease. Children of diabetics should adopt a healthy lifestyle in order to prevent and / or delay the disorders to which they are genetically predisposed [7].
Prospective studies and clinical trials highlight the importance of physical exercise and / or the combination of physical exercise and dietary lifestyle changes resulting in the prevention of DM2 [8, 9].
Prospective studies and clinical trials highlight the importance of physical exercise and / or the combination of physical exercise and dietary lifestyle changes resulting in the prevention of DM2 [10, 11, 12].
In view of these data, and the hypothesis of the effectiveness of the intervention of these protocols in diabetics, and of the consistency of the prevention of DM2 through physical exercise, the objective of the present study was to verify the effects of a resistance and combined training session on the parameters hemodynamic (heart rate and blood pressure) and metabolic (capillary glycemia) of individuals born to diabetics.
Methods
Samples
Individuals with a positive history of DM are children of diabetics participating in Sweet Life - Supervised Physical Exercise Program for Diabetics. The subjects without a family history of DM were selected through the dissemination of posters in the Graduation Course of the Higher School of Physical Education at the University of Pernambuco.
Sixteen subjects of both genders were voluntarily selected for the present study, who were allocated to two intervention groups, the Children of Diabetics (CD) group, n = 08, and the Children of Non-Diabetics (CND) group, n = 08.
All participants were informed about the procedures that would be performed during the study, and after explanation, they signed the Informed Consent Term, which was registered and duly authorized by the Ethics and Research Committee of the University of Pernambuco, obtaining the opinion nº 386,094 / 2013.
To participate in the research, the subjects of both groups should meet the inclusion criteria, such as: chronological age between 18 and 30 years, be sedentary, blood pressure less than 140/90 mmHg, capillary blood glucose less than 125 mg / dL, not being a smoker, not having drunk three days before collection, having a BMI of 18.5 kg / m² to 25 kg / m² The subjects who presented complications of orthopedic and myoarticular order, recent surgeries, diagnoses of pathologies of cardiological, metabolic, neurological and rheumatological order did not participate in the study. Instrumentation and Data Collection Hemodynamic variables of Blood Pressure (BP) and Heart Rate (HR) and the metabolic variable of Capillary Glycemia (CG) were evaluated. The measurements of each variable were performed before and after each training session, with the BP and HR variables being measured by the same evaluator using double channel RAPPAPORT® premium stethoscopes and aneroid sphygmomanometers also. BP was measured with the subject resting for five minutes, in a calm environment, in a sitting position with his legs uncrossed, making sure that they did not ingest alcoholic and caffeinated beverages, nor practiced physical exercise in the last 24 hours before collection, following exactly all the recommendations of the VI Brazilian Guidelines on Hypertension [13].
Heart rate was measured using a POLAR® cardiac monitor model FT1. The HR value was obtained with the cardiac monitor on the right wrist, together with the heart rate belt properly positioned above the xiphoid appendix. At the time of HR measurement, the subject was at rest and the lowest value indicated on the cardiac monitor was adopted between the 60th and 70th seconds of the appointment. To ensure the state of rest, the same recommendations as the VI Brazilian Guidelines on Hypertension were adopted [13].
Capillary glycemia was measured 60 minutes after the completion of a routine meal, which coincided before the intervention of the physical exercise sessions. Glucometers BAYER® model Breeze 2 were used, the measurement was performed on the ring finger and / or minimum, discarding the first drop of blood, following the procedures described and validated by Hortensus [14].
The Body Mass Index was obtained from the height measurement in a wooden stadiometer, where the subject was in an orthostatic position, to check the height, and he took a deep inspiration. Body mass was determined using a FILIZOLA® scale, with a maximum load of 150 kg and a minimum interval of 100 grams [15]. The age data, diagnosis of diabetes of the parents, and the report of physical inactivity, were obtained through an anamnesis answered shortly after acceptance and signature of the Informed Consent Form.
Protocol of Training Sessions
The physical exercise sessions were divided into two training groups, the Resistance Training (RT) group and the Combined Training (CT) group. The sessions were held individually and lasted 65 minutes.
The collection was carried out at the premises of the School of Physical Education/University of Pernambuco between the hours of 09:00 to 11:00 and / or from 14:00 to 16:00, in the Biodynamics Laboratories and in the Laboratory Human Performance, with an average temperature of 22 ºC and a relative humidity of 65%. Each session was supervised by physical education teachers and academics, all properly trained for specific follow-up.
Each subject participated in a session of the RT and a session of the CT, adapted from Lima. et al, [12]. The sessions were held on non-consecutive days, with the first session of the RT and successively the second of the CT.
Resistance Training was performed as follows:
- 1st Stage - Warm-up: Pectoralis, Grande Dorsal, Deltoides, Triceps Brachii, Biceps Brachii, Quadriceps Femoris, Hamstrings, and Gastrocnemius exercises, lasting 15 seconds for each movement. Totaling 15 minutes for this step.
- 2nd Stage - Main Part: Eight TR exercises were performed at the Biodynamics Laboratory (Flying - Pectorals, Seated Row - Dorsal, Alternating Frontal Lift with Dumbbells - Deltoid, Triceps Forehead - Triceps Brachii, Alternating Curl Dumbbell - Biceps Brachial, Chair Quadriceps Femoral Extender, Flexora Chair - Hamstrings, Bilateral Calf - Gastrocnemius). Free weights (dumbbells and rings) and New Fit Equipment® machines were used to perform the exercises. The present study used, for determining the intensity of the RT, the system of “series until failure” [16], which consists of performing repetitions until exhaustion, that is, performing a series until no repetition (concentric phase of the movement) is completed with the “correct” exercise technique [17]. The multiple series system was used, with three series of 8-16 repetitions, with a maximum execution speed of 1 second for the concentric and eccentric phase, with intervals between the series and exercises of 45 seconds. Totaling 40 minutes for this step.
- 3rd Stage - Cooling: Stretching exercises for the Pectoral, Great Dorsal, Deltoid, Brachial Triceps, Brachial Biceps, Quadriceps Femoris, Hamstrings, and Gastrocnemius, lasting 15 seconds for each movement, along with body awareness and relaxation work. Totaling 10 minutes for this step.
The Combined Training was carried out as follows: The Heating and Cooling steps were the same as those performed in the RT. The Main Part, lasted 20 minutes of Aerobic Training (AT), on a treadmill of the Imbrasport® brand of super atl model, held at Biodynamics Laboratories and in the Laboratory Human Performance.
The training intensity was manually controlled by the same evaluator according to the established protocol, and the response presented by the Heart Rate (HR) during the effort. The training intensity was obtained from the Reserve Heart Rate (RHR) formula for use in sedentary individuals [18].
The progression of the intensity of the AT occurred with three minutes of warm-up to an HR below 40% obtained by calculating the RHR, ten minutes at an intensity of 50% to 60%, ten minutes at an intensity of 60% to 70%, and three minutes of cooling to an HR below 40%. After the AT, the subject went to the Biodynamics Laboratory where six RT exercises were performed (Seated Row - Great Dorsal, Forehead Triceps - Triceps Brachii, Alternating Dumbbell Curl - BicepsBraquial, Extending Chair - Quadriceps Femoris, Flexor Chair - Hamstring , Bilateral Panturrilha - Gastrocnêmio), following all guidelines covered in the TR protocol, totaling 40 minutes for this stage.
The post-session collections of the RT and CT occurred with the subjects at rest for five minutes after the cooling stages of each session. For the BP and CG measures, the same procedures as for pre-training collection were adopted. For HR measurement, only the time taken to mark the result obtained is reduced (the lowest value indicated on the cardiac monitor was adopted between the 10th and 15th seconds of the mark).
Statistical Analysis
For statistical analysis, the SPSS for Windows 16.0 software was used. The Wilcoxon test was used for the intragroup evaluation and the Kruskal-Wallis test for intergroups, considering values of significance level of p≤0,05.
Results
The Children of Diabetics (CD) presented, in most of the variables at rest (BP, HR and CG) higher values when compared with the Children of Non-Diabetics (CND) (Table 1).
| CD | CND | p | |
|---|---|---|---|
| n | 8 | 8 | |
| Age (years) | 21,71 ± 2,3 | 21,62 ± 3,1 | |
| BMI (Kg/m2) | 25,13 ± 5,2 | 22,71 ± 2,4 | |
| History of Diabetes (♂♀) | 5♂3♀ | X | |
| Physical Downtime (months) | 36,87 ± 30,2 | 6,37 ± 3,0 | p= 0,001 |
| Systolic Blood Pressure (mmHg) | 122,0 ± 10,4 | 104,8± 8,6 | p= 0,001 |
| Diastolic Blood Pressure (mmHg) | 79,2 ± 7,2 | 64,5 ± 7,8 | |
| Heart Rate (bpm) | 82 ± 9 | 77 ± 9 | |
| Capillary Glycemia (mg/dL) | 101,4 ± 11,5 | 94,2 ± 8,8 |
Table 1: Baseline characteristics of the Children of Diabetics Group (CD) and the Children of Non-Diabetics Group (CND). * The re
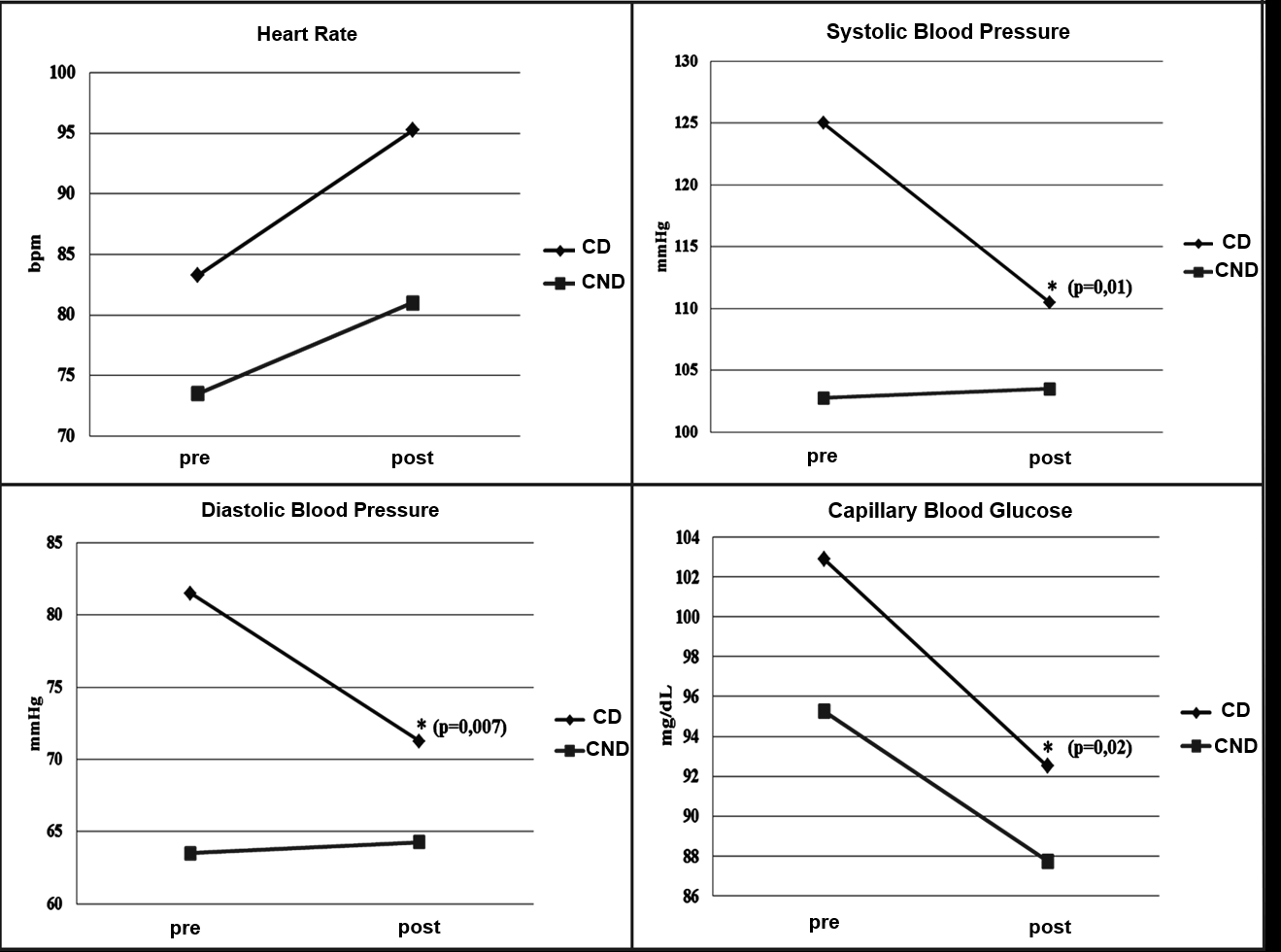
Table 1: Baseline characteristics of the Children of Diabetics Group (CD) and the Children of Non-Diabetics Group (CND). * The results are presented in means and standard deviations; ♂ – Diabetic Father, ♀ – Diabetic Mother, X – No History of Diabetes, RT – Resistance Training, CT – Combined Training, p – Significance Level After the intervention, in the intragroup analysis, the CD group in the RT, obtained a significant reduction in the values of Systolic Arterial Pressure (SBP) (125.0 ± 10.0 mmHg vs 110.5 ± 15.9 mmHg p = 0.01 ), Diastolic Blood Pressure (DBP) (81.5 ± 6.4 mmHg vs 71.2 ± 10.4 mmHg p = 0.007), and Capillary Glycemia (CG) (102.8 ± 16.1 mg / dLvs 92.5 ± 10, 9 mg / dL p = 0.02) (Figure 1). The CT did not reduce the variables in the intragroup analysis of the two groups (CD and CND).
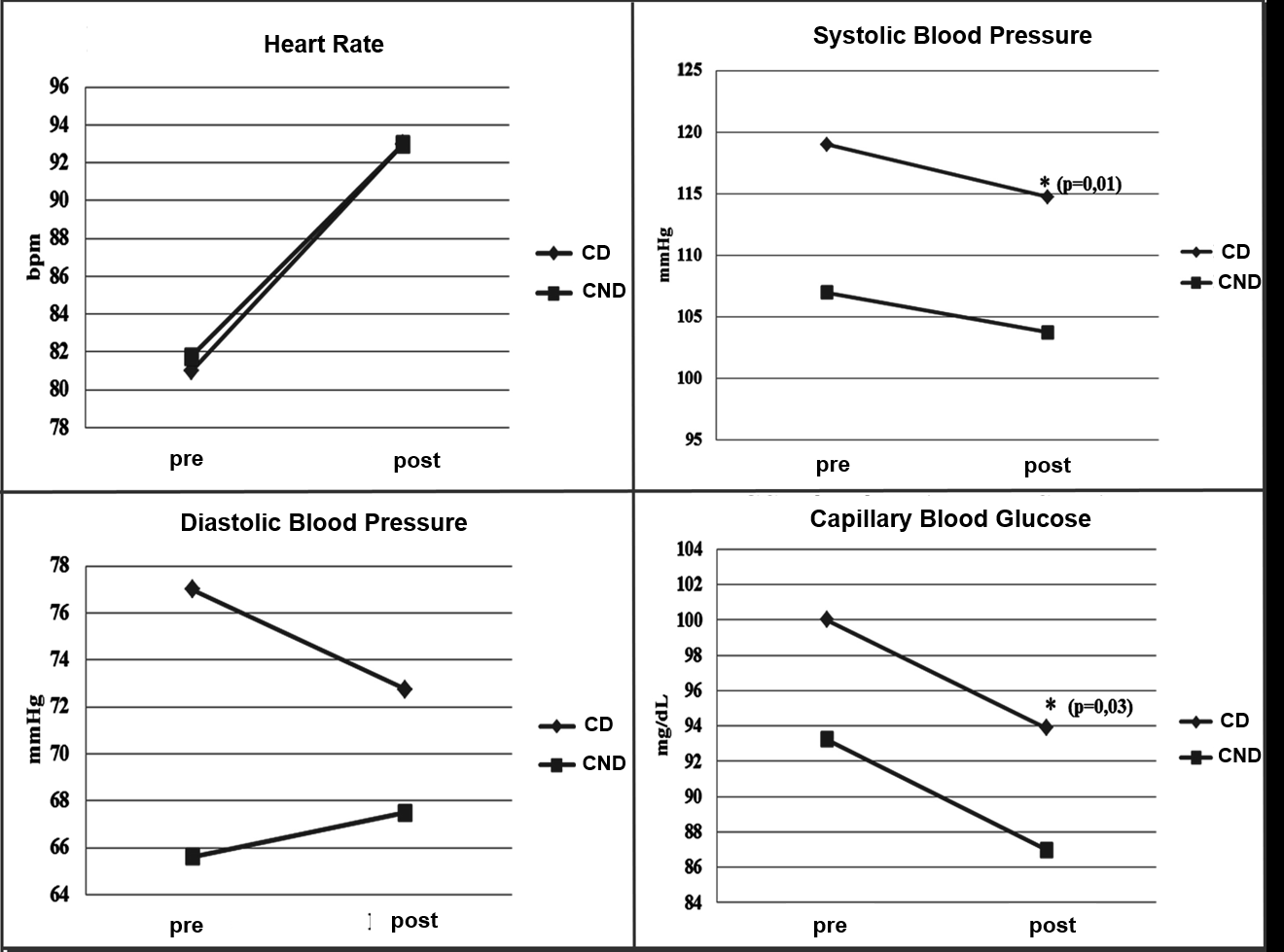
In the intergroup analysis, there was no significant difference in the acute effects for the groups (CD vs CND) in RT. In the TC, the Children of Diabetics presented better results when compared with the NDF in the variables SBP (114.75 ± 11.5 mmHg vs 103.75 ± 9.92 mmHg p = 0.01) and CG (93.8 ± 8, 02 mg / dL vs 87.0 ± 4.97 mg / dL p = 0.03) (figure 2).
Discussion
The research was guided with the objective of verifying the effects of a resistance and combined training session on the hemodynamic (HR and BP) and metabolic (CG) parameters of children of diabetic parents Cross-sectional studies support that β cell malfunction is related to glucose intolerance in subjects with a first-degree family history of diabetes [19], where they are at greater risk of developing glucose intolerance and DM due to the presentation of reduced glucose uptake [20, 21].
The results of the present study demonstrated that CD showed significant reductions in SBP (p = 0.01), DBP (p = 0.007) in CG (p = 0.02) with the intervention of RT, and SBP (p = 0.01) and in the CG (p = 0.03) with the intervention of CT.
These findings can be explained based on the study by Boulé [22] where he states that adding physical exercise can improve glucose tolerance and based on Kraemer and Hakkinen [23] where from a phenomenon called the adaptation window; which consists of a potential for changes achieved when starting a training, that is, when the subject is less trained, the greater the potential for changes (objectives achieved) with the training and the greater the window of adaptation, on the contrary it should be smaller when the individual is more trained [24]. This hypothesis that the higher the subject’s training level, the smaller his adaptation window, can justify the results presented in the CND group. Where they were more active compared to the CD group (CD 36.87 ± 30.27 months vs CND 6.37 ± 3.07 months).
The results of both groups (although more effective in the CD group due to the influence of the adaptation window) may be related to the molecular mechanisms of glucose entry into the skeletal muscle, promoted by the activation of IRS1
and IRS2 (receptor substrate insulin 1 and 2) and the PI3k / AKT pathway, resulting in a greater translocation of GLUT4 to the cell membrane leading to an increase in glucose entry by facilitated diffusion [25, 26, 27].
The pre-training CG values were within normal levels for both groups according to the SBD and adequate according to the inclusion criteria of the present study, but it was noted that the CD present a higher value of the CG when compared to NDC (102.8 ± 15.1 mg / dL vs 95.2 ± 9.7 mg / dL in the RT session) and (100.0 ± 5.7 mg / dL vs 93.2 ± 7 , 7 mg / dL in the CT session) [28].
The hypothesis to justify this result may be related to the positive family history of DM, in addition to the altered BMI in the classification of overweight in the CD group (25.13 ± 5.2 Kg / m² vs 22.71 ± 2.4 Kg / m²), and the longest physical downtime3.
The present study, which is unique in several aspects, can expand the knowledge of the effects of physical exercise and family history on the development of DM2, where the protocols of RT and CT were used in an acute way, which were effective in trying to avoid the DM2 risk in CD, with a reduction in systolic blood pressure, diastolic blood pressure and capillary blood glucose after RT and CT
Conclusion
It is concluded that the children of diabetics, from this sample, presented positive results after the intervention of Resistance and Combined Training, but may present future risk for the development of Diabetes Mellitus according to Capillary Glucose before physical exercise, indicating that this group should include physical exercise in your daily routine.
References
-
Zecchin HG, Carvalheira JBC, Abdalla MJ (2002) Genetic basis of insulin resistance, metabolic syndrome and type 2 diabetes mellitus. 2 Rev SOCESP 3: 508-520.
-
Grant RW, Moore AF, Florez JC (2009) Genetic Architecture of Type 2 Diabetes: Recent Progress and Clinical Implications. Diabetes Care 32(6): 1007-1014.
-
Sargeant LA, Wareham NJ, Khaw KT (2000) Family history of diabetes identifies a group at increased risk for the metabolic consequences of obesity and physical inactivity in EPIC-Norfolk: a population-based study. The European Prospective Investigation into Cancer. Int J Obes Relat Metab Disord 24(10): 1333-1339.
-
Wilson PW, Meigs JB, Sullivan L, Fox CS, Nathan DM, et al. (2007) Prediction of Incident Diabetes Mellitus in Middle Aged Adults: The Framingham Off spring Study. Arch Intern Med 167(10): 1068-1074.
-
American Diabetes Association (2014) Standards of Medical Care in Diabetes-2014. Diabetes Care 37: S14-S80.
-
Jouven X, Empana JP, Schwartz PJ, Desnos M, Courbon D, et al. (2005) Heart-rate Profile During Exercise as a Predictor of Sudden Death. N Engl J Med 352(19): 1951- 1958.
-
Sartori M, Hereen MV, Valente J, Tubaldini M, Irigoyen MC, et al. (2011) Positive family history of diabetes alters chronotropic response to acute exercise. Rev Bras Med Esporte 17(6): 389-392.
-
Manson JE, Nathan DM, Krolewski AS, Stampfer MJ, Willett WC, et al. (1992) A Prospective Study of Exercise and Incidence of Diabetes Among US Male Physicians. JAMA 268(1): 63-67.
-
Tuomilehto J, Lindstrom J, Eriksson JG, et al. (2001) Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle Among Subjects With Impaired Glucose Tolerance. N Engl J Med 344(18): 1343-1350.
-
Sigal RJ, Kenny GP, Boule NG, George A Wells, Denis Prud’homme, et al. (2007) Effects of Aerobic Training, Resistance Training, or Both on Glycemic Control in Type 2 Diabetes: A Randomized Trial. Annals of Internal Medicine 147(6): 357- 369.
-
Castaneda C, Layne JE, Orians LM, Patricia L Gordon, Joseph Walsmith, et al. (2002) A Randomized Controlled Trial of Resistance Exercise Training to Improve Glycemic Control in Older Adults With Type 2 Diabetes. Diabetes Care 25(12): 2335 - 2341.
-
Lima GN, Queiroz SL, Cruz PWS, Santos HLBA, Cavalcanti CBS, et al. (2012) Effects of Aerobic, Resistance and Combination Training on the Body Composition of Type 2 Diabetics. ConScientiae Saúde 11(4): 543-549.
-
Sociedade Brasileira de Cardiologia, Sociedade Brasileira de Hipertensão, Sociedade Brasileira de Nefrologia (2010) VI Diretrizes Brasileiras De Hipertensão. Rev Bras Hipertens 17: 1-64.
-
Hortensius J, Slingerland RJ, Kleefstra N, Logtenberg SJJ, Groenier KH, et al. (2011) Self-Monitoring of Blood Glucose: The Use of The First or The Second Drop of Blood. Diabetes Care 34(3): 556-560.
-
Sabia RV, Santos JE, Ribeiro RPP (2004) Efeito da Atividade Física Associada à Orientação Alimentar em Adolescentes Obesos: Comparação entre o Exercício Aeróbio e Anaeróbio. Rev Bras Med Esporte. 10(5): 349- 355.
-
Gomes MB, Gianella D, Faria M (2006) Prevalence of Type 2 Diabetic patients within the targets of care guidelines in daily clinical practice: a multicenter study in Brazil. Rev Diabetic Study 3(2): 73-78.
-
Snowling, NJ, Hopkins WG (2006) Effects of different modes of exercise training on glucose control and risk factors for complications in type 3 diabetic patients: a meta-analysis. Diabetes Care 29(11): 215-227.
-
Marins JCB, Luiz A, Monteiro A, Jesus G (1998) Validation of Heart Rate Measurement Time after Submaximal Effort at 50 and 80%. Rev Bras Med Esporte 4(4): 114- 119.
-
Pimenta W, Korytkowski M, Mitrakou A, et al. (1995) Pancreatic Cell Dysfunction as The Primary Genetic Lesion in NIDDM: Evidence From Studies in Normal Glucose Tolerant Individuals With a First Degree NIDDM Relative. JAMA 273(23): 1855-1861.
-
Cnop M, Vidal J, Hull RL (2007) Progressive Loss of Cell Function Leads to Worsening Glucose Tolerance in First Degree Relatives of Subjects With Type 2 Diabetes. Diabetes Care 30(3): 677-682.
-
Best JD, Kahn SE, Ader M, Watanabe RM, Ni TC, et al. (1996) Role of glucose effectiveness in the determination of glucose tolerance. Diabetes Care 19(9): 1018-1030.
-
Boulé NG, Weisnagel SJ, Lakka TA (2005) Effects of Exercise Training on Glucose Homeostasis: The HERITAGE Family Study. Diabetes Care 28(1): 108-114.
-
Kraemer WJ, Hakkinen K (2002) Strength Training for Sport, 1st (Edn.), Blackwell Publishing, Oxford.
-
Azevedo DC, Carvalho SC, Leal EWPS, Damacesno SP, Ferreira ML (2008) Influência da Limitação da Amplitude de Movimento Sobre a Melhora da Flexibilidade do Ombro Após um Treino de Seis Semanas. Rev Bras Med Esporte 14(2): 119-121.
-
Pauli JR, Cintra DE, Souza CT, Ropelle ER (2009) New mechanisms by which physical exercise improves insulin resistance in the skeletal muscle. Arq Bras Endocrinol Metab 53(4): 399-408.
-
Hayashi T, Wojtaszewski JF, Goodyear LJ (1997) Exercise Regulation of Glucose Transport in Skeletal Muscle. Am J Physiol 273(6): 1039-1051.
-
Ropelle ER, Pauli JR, Prada PO, Cláudio T S, Paty K Picardi, et al. (2007) Reversal of Diet Induced Insulin Resistance With single Bout of Exercise in the Rat the Role of PTP1B and IRS-1 Serine Phosphorylation. J Physiol 577(3): 997- 1007.
-
Sociedade Brasileira de Diabetes (2014) Diretrizes da Sociedade Brasileira de Diabetes, 2nd (Edn.), Grupo Gen.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance