Role of New Insulin Analogs in the Management of Diabetes. A Clinical Review
This paper has reviewed different insulin analogs currently available in the market and pharma industry, their safety, efficacy and their roles in the diabetes management, comparing with human regular and NPH insulin. Traditional insulins (human regular and NPH insulins) do not have constant or smoother pharmacokinetic and pharmacodynamic profiles and are usually associated with erratic blood glucose profiles with hypoglycemia or hyperglycemia when compared with analog insulins. Similarly they do not match physiologic insulin profiles with basal bolus format. According to the medical literature, current insulin analogs are more efficacious and also it has been documented in research trials that recent insulin analogs are better and safer as compared to human regular and NPH insulin in terms of hypoglycemia and HbA1c reductions. Hence this paper has reviewed these insulins analogs (longer acting basal and rapid acting insulin analogs) for their safety and efficacy in terms of hypoglycemia and HbA1c control, for the management of both type-1 and type-2 diabetics in hospitals and clinics.
Introduction
Diabetes Disease, Traditional and Analog Insulins
Diabetes Mellitus is a clinical syndrome characterized by hyperglycemia due to insulin deficiency and insulin resistance [1, 2, 3, 4]. Good metabolic control is essential to prevent complication of diabetes [5]. Type-1 diabetics require only insulin to control glucose metabolism mostly basal bolus regimen. However, type-2 diabetics, due to insulin resistance, also require oral agents (such as metformin) to control blood glucose [6, 7]. Clinical experience has shown that most of these type-2 diabetic patients will require also insulin over the time in combination with oral agents if good glycemic control is not achieved. They may require only basal insulin initially, then mixtures of insulins, two times daily, and finally some will be managed by basal bolus regimens as well [8].
Regarding analog insulins, they are very similar to human insulin, however, their one or two amino acids are changed by biotechnology and genetic engineering methods. In recent years, several insulin analogs injections have been developed. However, in clinical practice most of the physicians still use human regular insulin and NPH insulin or combination of them (Humulin 30/70). Our aim in this review is to highlight the role of current available insulin analogs (rapid acting and longer acting insulin analogs) in the management of diabetes, their efficacy and safety in terms of hypoglycemia and HbA1c reductions. Current topic has not been reviewed in the past in such a manner and this review will significantly contribute to the scientific literature and to the diabetes physicians so that they can clinically judge which insulin is more efficacious and safe in their clinical practice while managing diabetes in hospitals and clinics.
Methods and Literature Review
This is a scientific review article, comparing different insulins currently available in the pharmaceutical industry. Time duration of literature search was four months, from January 2022 until April 2022. For literature review of various insulins, different studies and research trials were searched on the internet from PubMed from the year 1920 until 2022. The search criteria for articles were the terminologies, including “insulins”, “hypoglycemia” “HbA1c”, “insulin analogs”. Only free full text papers in English language were selected. Out of 257 results, 74 studies were short listed and selected focusing on newer insulin analogs and their comparison with other insulins. After detailed study from the research papers text, main conclusions were drawn comparing human insulins (regular and NPH) with that of current long acting and rapid acting insulin analogs (RAIs). Also different variables such as Insulin types, HbA1c, Hypoglycemia, Plasma glucose were also studied in this review with their scientific applications and these variables were also discussed among different insulins, for their safety, efficacy and flexibility of use in the selected literature.
Clinical Management of Hyperglycemia by Insulins
Diabetes mellitus is a hyperglycemia syndrome with different etiologic presentations, a condition which must be diagnosed specifically before targeted treatment (insulin/ oral agents) is initiated and prescribed to the patient. According to the literature review, we have found that recent insulin analogs are safer and efficacious than human insulins in terms of hypoglycemia and HbA1c reductions and for better diabetes control. Initially for the commercial use, insulin was extracted from porcine and bovine pancreata, with a purity of 80 - 90%, with some major contaminants and allergens. Hence, such insulin was associated with immune- mediated reactions, especially lipoatrophy, antibody mediated insulin resistance with swelling and pain at the site of injection, ultimately affecting the kinetics of insulin absorption and action [9]. In the medical research and literature history, industrial synthesis of human insulin was done by three techniques. The earliest one involved isolation of insulin directly from human cadaveric pancreata and thereafter purifying it i.e., methods for separating insulin from non- insulin protein [10]. But due to unavailability of human tissue, this technique did not provide sufficient quantities for commercial insulin preparation. The other technique so called “semi- synthesis”, chemically converts porcine/bovine insulin to the human insulin sequence via substitution of the one amino acid in the primary sequence [11]. Lastly, in 1980, recombinant DNA technology was patented and introduced and human insulin became widely available commercially. This technique involves insertion of human DNA sequence into bakers’ yeast or bacteria Escherichia coli and thereafter genetically programmed to synthesize the insulin molecule [12, 13, 14]. Hence, this insulin is called human insulin. The insulin produced by this technique is then purified to ~ 99.9% via chromatography columns, ultimately eliminating immune - mediated side effects. Advancement from animal to human insulin has reported greater degree of hypoglycemia in some patients [15, 16]. But up to date systemic reviews and research studies have not proven this fact [17, 18].
Regarding Industrial Evolution of Insulin and soluble and long - Acting Insulin Preparations, in the past, duration of action of soluble insulin was prolonged by adding modifying agents [19]. But at the same time this was associated with pain and swelling at the site of injection. Therefore, clinically only one injection was given to the patient to meet daily insulin requirement. However, this methodology was clinically difficult because kinetics of absorption and insulin action were variable and unpredictable. Then later on, a new method was introduced of making insulin a poorly soluble complex thus reducing its absorption from site of injection [20, 21, 22]. Furthermore, small amount of zinc was added to stabilize this complex thus maintaining the duration of action for 24 hours. This resulted in constant rate of absorption and duration of action lasting for 12-24 hours, and was named isophane or neutral protamine Hagedorn (NPH) [115, 116]. In later years, semilente, and lente insulins were produced by the same methodologies [23, 24, 25]. This was one of the famous and widely used insulin preparations available at that time.
Regarding Human Soluble insulins and Rapid Acting insulin Analogs (RAI), also there was extensive research was conducted to make insulins more compatible for human use. Following injection, insulin containing fluid moves via osmosis, leading to dilution with dissociation of the insulin molecules. This gradual process facilitates insulin molecules to be transported across the capillary walls into circulation as monomers [26, 27]. Because of this slow process of diffusion, patients are advised to inject soluble insulin at least 30 minutes before a meal so that enough insulin is available to circulation when blood glucose levels rise, immediately after when meals is absorbed. For many patients this technique is difficult to follow i.e., to inject insulin prior meal approximately half an hour, especially in case of children with greater risk of hypoglycemia. Hence, great care and meal planning is required especially in type-1 diabetic children.
To overcome this difficulty, extensive research at molecular level was conducted during the last two to three decades. We have extensively reviewed pharmacokinetics and pharmacodynamics of different insulins. The biologic action of insulin can be reduced by producing specific changes in amino acid sequence of insulin molecule via genetic engineering recombinant DNA technology [28]; thus dissociation rate constants from receptors are increased relative to human insulin. These analogs dissociate faster and absorb rapidly from site of injection to the blood circulation and patient can inject insulin just 5-10 minutes prior to meal [29]. This technique is even more flexible for the patients and especially in case of type-1 diabetic children. This insulin is called Rapid Acting Insulin Analogs (RAI).
Currently, three such RAIs patents are available, namely, insulin lispro (Humalog®, Lilly Company), insulin aspart (Novorapid ®, Novo Nordisk Company) and insulin glulisine (Apidra®, Sanofi - Aventis Company) [30, 31]. These analogs dissociate faster and have quick onset (within 10 – 20 minutes), with shorter duration of action (3 - 5 hours) as compared to soluble insulin (30 - 60 minutes, and 6 – 8 hours, respectively) [32], thus limiting the chance of hypoglycemia 3-4 hours post prandially (after meals) or in post absorptive state. Combination of these insulins with protamine is also available (Novo Mix 30, Humalog Mix50, Humalog Mix25), also known as biphasic insulins [33]. All these RAIs and biphasic mix insulins have been patented to be used in diabetes management by insulin injections for both type-1 and type-2 diabetic subjects.
Discussion
There are several clinical studies which have demonstrated the safety and efficacy of RAI patents in both type-1 and type 2 diabetic subjects, when used with other intermediate acting insulins as a part of “ basal bolus” therapy, or as continuous subcutaneous insulin infusion (CSII) in insulin pumps [34]. The time - action profile of RAIs mimics exactly with physiological needs at meal time and controls post-prandial hyperglycemia more effectively and is easily applicable in clinical practice. Furthermore, patient are more compliant to use RAIs at home as compared to soluble insulin which must be injected half an hour before meals and may cause hypoglycemia sometimes after 3-4 hours post meals. In recent clinical trials, RAIs appear to be better than soluble insulins in achieving better glycemic control with less hypoglycemia, both in type-1 and type-2 DM subjects [35].
Regarding Long Acting Insulin Analogs, insulins such as isophane (NPH) and insulin lente can cover the 12 - 24 - hour period with much absorption variability from subcutaneous tissue injection depot [36]. Their pharmacokinetics and pharmacodynamics demonstrate great variabilities after absorption to subcutaneous tissue. Thus they may lead to hypoglycemia especially when peak activity is reached, and when combined with regular insulin, both may additively cause hypoglycemia post meals, e.g., before lunch or late mid night. As in case of RAIs with the applicability of genetic engineering technology, the primary amino acid sequence of insulin molecule can be modified with the change in pH. In addition, insulin first precipitates at injection site and absorbs more slowly and constantly with negligible variability for 24 hours mimicking basal insulin secretion from pancreas [37]. One of the novel insulin is Insulin “Glargine”, a long acting insulin up to 24 hours (or even more), with peak less activity, and achieving good glycemic control with less symptomatic hypoglycemia. Efficacy and safety of glargine has been demonstrated by laboratory research and clinical trials as well [38, 39, 40, 41, 42, 43, 44, 45]. This insulin glargine is U-100. In the recent years, Glargine U-300 is also available (called Toujeo) with better biological profile and acting up to 36 hours, with more flexibility regarding time of injection. Furthermore, another insulin, comparable to Toujeo, is now also available in the market with the name insulin degludec (Tresiba). These basal insulins have a duration of action of more than 30 hours and provides more flexibility, and are safer and efficacious than older NPH insulins in terms of hypoglycemia reductions and better HbA1c control.
Insulin Detemir is another long-acting insulin analogue that was developed using a different strategy i.e., binding to albumin. This technology has been patented such that aliphatic fatty acid has been acylated to the B29 amino acid with simultaneously removal of B30 amino acid [46]. This results in reversible binding of albumin with the fatty acid acylated to the insulin. Hence, after injection, 98% of the insulin bounds to albumin with gradual release from albumin binding, allowing sustained, prolonged action of insulin detemir. Pharmacokinetic and pharmacodynamic properties and bioavailability of different insulin preparations when injected are presented in Table 1 and graphically in Figure 1.
| Preparation | Time of action | ||
|---|---|---|---|
| Onset,h | Peak,h | Effective Duration, h | |
| Short Acting | |||
| Aspart | <0.25 | 0.5-1.5 | 2 to 4 |
| Glulisine | <0.25 | 0.5-1.5 | 2 to 4 |
| Lispro | <0.25 | 0.5-1.5 | 2 to 4 |
| Regular | 0.5-1.0 | 2 to 3 | 3 to 6 |
| Long Acting | |||
| Detemir | 1 to 4 | no peak | 12 to 24 |
| Glargine | 2 to 4 | no peak | 20 to 24 |
| NPH | 2 to 4 | 4 to 10 | 10 to 16 |
| Insulin Combinations | |||
| 75/25-75% Protamine lispro, 25% lispro | < 0.25 | Dual | 10 to 16 |
| 70/30-70% Protamine aspart, 25% aspart | < 0.25 | Dual | 15 to 18 |
| 50/50-50% Protamine lispro, 50% lispro | < 0.25 | Dual | 10 to 16 |
| 70/30-70% NPH, 30% regular | 0.5 to 1 | Dual | 10 to 16 |
Table 1: Properties and bioavailability of insulin preparations.
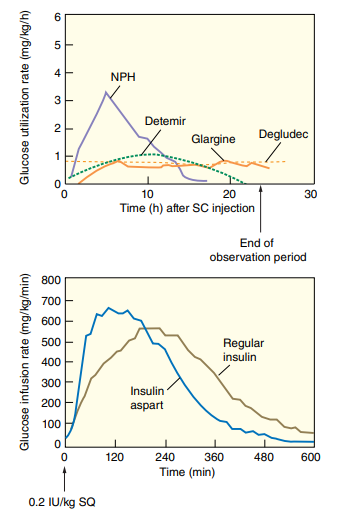
When injected, insulin detemir is in hexameric form. Thereafter at injection depot site it takes form of hexamer dihexamer equilibrium thus increasing self association state at depot and prolonged duration of action [46]. There is a relative peak activity at 6 to 8 hours after injection (versus peakless activity of glargine) and prolong duration of action up to 24 hours and in dose dependent fashion [47]. Clinical trials have shown less hypoglycemia and less variation in blood glucose levels with insulin detemir as basal insulin in intensive insulin regimens versus NPH insulin [48, 49, 50]. Both insulin glargine and levemir, are now approved to be used in diabetic patients [51, 52, 53]. RAIs have shortest time action profile, insulins NPH and lente intermediate, while insulin ultra lente, glargine, detemir, tojeo and tresiba have longest duration of action [54, 55, 56].
Human insulin analogs produced by genetic engineering and recombinant DNA technology are now most widely used clinically and available commercially in many countries and ultimately has replaced the animal insulins. Insulin is commercially available in unit concentrations of 100U/mL or 500 U/mL, designated U-100 or U-500 respectively. The U-500 with high concentration is used only in rare cases of insulin resistance when the patient requires extremely large doses of insulin to control blood sugar. 100 U/mL is commonly used in most of the countries. Physiologically, insulin secretion basally is low between meals with prandial peaks immediately after meals. As soon as meal is ingested and consumed, insulin is secreted in pulsatile manner accordingly with each meal, with usually no significant secretion overnight and during fasting state.
Considering the management of diabetes in outpatient
clinics, it is highly advisable to prescribe the patient an insulin regimen which mimics the normal physiological insulin release pattern, covering both the prandial and basal requirements, flexible, and that fits best with individual needs and lifestyle. Different regimens are now available and each regimen has different time action profiles and benefits. Patients should be educated about different insulin regimens and their special characteristics. Regimens are designed to meet the daily requirement of insulin in relation with food and basal pattern. Every patient, including adults, children and older age groups, has different eating patterns and different lifestyle. Each patient should be selected specifically for different available insulin regimens. However, basal bolus regimen is the priority if glycemic control is not optimal with conventional regimens. Selection of insulin, e.g., Regular insulin or RAIs, depends on the eating pattern, food density, and other factors as well including physician’s clinical experience. RAIs can cover and reduce post meal or postprandial hyperglycemia up to approximately 4 hours. Regular insulin can cover post prandial hyperglycemia up to 6 to 8 hours but may also cause hypoglycemia 3-4 hours post meals, especially in children and lean patients. RAIs should be considered if patients frequently develop day time hypoglycemia, while at work, with regular insulin. Hence, in these settings RAIs are recommended over human regular insulin. Similar is the case with NPH insulin; if patient have hypoglycaemia with NPH, it is preferable to shift the patient to longer acting insulin analogs (insulin detemir, glargine or degludec) [57, 58, 59, 60, 61, 62, 63, 64].
Conclusion and Recommendations
In conclusion, it has been demonstrated in the research studies that human insulins (regular and NPH or their combinations such as insulin mixtard 30/70) are not an appropriate option for diabetic patients especially type-1 diabetics; because they are associated with unpredictable pharmacokinetic profiles and also associated with erratic serum glucose values. They may be associated with more day- time, night-time, or late-night hypoglycemia when compared with insulin analogs. Analog insulins are compatible with normal pancreatic physiologic insulin secretion pattern with basal bolus regimens. It is highly recommended to prescribe insulin analogs in clinical practice especially if the patient is type-1 diabetic.
Furthermore, it is recommended to refer the newly diagnosed diabetic patient (after starting the appropriate therapy) to the tertiary care diabetic center for evaluation by diabetologist and diabetes specialist care team for proper management and adjustment of therapy. The diabetic educator and dietitian must be involved in diabetology clinics of tertiary or primary care diabetes centers for education about insulin/ OHA, meal planning, techniques of insulin injections, dosage adjustments according to the meals, SMBG, exercise, sick day management, and management of insulin complications (hypoglycemia, weight gain etc.) and diabetes related complications (neuropathy, retinopathy, nephropathy, foot complications, and others as well).
For type-1 diabetics, it is always advisable and recommended to use basal bolus regimen with available long acting and rapid acting insulin analogs. For type-2 diabetics, they may require combination of insulins with oral agents (such as metformin, DPP-4 inhibitors, SGLT-2 inhibitors, TZDs) [65, 66, 67, 68]. However type-2 diabetics may be controlled on simpler mixtures of insulins (Humalog Mix 50, Humalog Mix25, or Novomix 30); if glycemic control is poor, then they can be shifted to basal bolus regimens accordingly. Furthermore, these insulin analogs can be combines as well with GLP1-Receptor Agonists (exenatide, liraglutide, albiglutide, and dulaglutide), which provides good HbA1c control among obese patients with additional reductions of cardiovascular risk factors [69, 74].
In conclusive summary, currently available insulin analogues (RAIs, glargine, levemir, degludec) are clinically safer and efficacious for most of the patients as all these insulin analogues mimic physiological insulin release pattern. When combined as basal bolus regimen or MDI, is the best choice for type-1 diabetic patients and most of them type-2 diabetic patients uncontrolled on OHA. Multidisciplinary approach is recommended for the management of diabetes in tertiary care centers, which include diabetologist, endocrinologist, diabetes health educator and dietitian. It is also advisable that all diabetic patients should be screened for diabetes and vascular complications and to initiate appropriate additional therapies with early initiation of insulin to prevent further progress of diabetes related complications.
Conflict of Interest
All authors declare no conflict of interest.
Acknowledgement
Authors are thankful for Dr.Zainab Kamran (third year medical student, Jinnah Sindh Medical University, Karachi) and Dr. Khttab Kamran (first year medical student, Karachi Medical & Dental College, Karachi) for their valuable scientific support, literature review and extraction of references.
Funding
This project was not funded by any organization and authors themselves reviewed the medical literature, collected data, written and edited the manuscript.
References
-
Alberti KG, Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabetic Medicine 15(7): 539-553.
-
Himsworth HP (2013) Diabetes Mellitus: Its differentiation into insulin sensitive and insulin- insensitive types 1936. Int J Epidemiol 42(6) 1594-1598.
-
Pérez AL, Brugués-Brugués E, de Leiva-Hidalgo A (2010) From pancreatic extracts to artificial pancreas: history, science controversies about the discovery of the pancreatic antidiabetic hormone. Avances en diabetología 26(5): 373-382.
-
World Health Organization (1965) Expert Committee on Diabetes Mellitus: First Report. Technical Report Series 310: 1-44.
-
Ashcroft SJ, Bunce J, Lowry M, Hansen SE, Hedeskov CJ (1978) The effect of sugars on (pro) insulin biosynthesis. Biochemical Journal 174(2): 517-526.
-
Giorgino F, Laviola L, Leonardini A (2005) Pathophysiology of type 2 diabetes: rationale for different oral antidiabetic treatment strategies. Diabetes research and Clinical practice 68(S): 22-29.
-
Klöppel G, Löhr M, Habich K, Oberholzer M, Heitz PU (1985) Islet pathology and the pathogenesis of type 1 and type 2 diabetes mellitus revisited. Survey and synthesis of pathology research 4(2): 110-125.
-
Krentz AJ, Bailey CJ (2005) Oral antidiabetic agents: Current role in type 2 diabetes mellitus. Drugs 65(3): 385-411.
-
Schlichtkrull J, Brange J, Christiansen AH, Hllund O, Heding LG (1972) Clinical aspects of insulin antigenicity. Diabetes 21(S2): 649-656.
-
Andrade AS, Vilela L, Tunes H (1997) Purification of bovine pancreatic glucagon as a by-product of insulin production. Brazilian Journal of Medical and Biological Research 30(12): 1421-1426.
-
Morihara K, Oka T, Tsuzuki H (1982) Semi-synthesis of human insulin. United States patent US 4,320,196.
-
Chien YW (1996) Human insulin: Basic sciences to therapeutic uses. Drug Dev Ind Pharm 22(8): 753-789.
-
Markussen J, Fiil N, Hansen MT, Norris K, Annerer G, et al. (2020) DNA-sequence encoding biosynthetic insulin.
-
Fávero-Retto MP, Palmieri LC, Souza TA, Almeida FC, Lima LM (2013) Structural meta-analysis of regular human insulin in pharmaceutical formulations. European Journal of Pharmaceutics and Biopharmaceutics 85(3): 1112-1121.
-
Schernthaner G (1993) Immunogenicity and allergenic potential of animal and human insulins. Diabetes care 16(S3): 155-165.
-
Gentofte LT, Lyndby H (1990) Biosynthetic insulin precursors and process for preparing the insulin precursors and human insulin. US4916212.
-
Lazaryev AP, Markussen J, Fiil N, Hansen MT, Norris K, et al. (2012) Method for producing human recombinant insulin. US0058513.
-
Berger W, Keller U, Honegger B, Jaeggi E (1989) Warning symptoms of hypoglycaemia during treatment with human and porcine insulin in diabetes mellitus. Lancet 1(8646): 1041-1044.
-
Teuscher A, Berger WG (1987) Hypoglycaemia unawareness in diabetics transferred from beef/porcine insulin to human insulin. Lancet 2(8555): 382-385.
-
Richter B, Neises G (2005) “Human” insulin versus animal insulin in people with diabetes mellitus. Cochrane Database Syst Rev 1: CD003816.
-
Airey CM, William DR, Martin PG, Bennett CM, Spoor PA (2000) Hypoglycemia induced by exogeneous insulin: “human” and animal insulin compared. Diabet Med 17(6): 416-432.
-
Bauman L (1939) Clinical experience with globulin insulin. Proc Soc Exp Biol Med 40: 170-171.
-
Hagedorn HC, Jensen BN, Krarup NB, Woodstrup I (1936) Protamin insulinate. JAMA 106: 177-180.
-
Jackson RL (1975) Protamine insulin product. US3868358.
-
Olsen HB, Balschmidt P, Kaarsholm NC, Jakobsen P (2006) Novel NPH insulin preparation. US20060258561.
-
Brader ML (2002) Insoluble insulin composition. US006465426.
-
Hallas MK, Peterson K, Schlichtkrull J (1951) Crystalline and amorphous insulin-zinc compounds with prolonged action. Ugeskr Laeger 113(52): 1761-1767.
-
Hoffmann JA (1996) Insulin formulation. US005534488.
-
Langballe P, Norup E (2001) Stabilezed insulin compositions. US6174856.
-
Søeborg T, Rasmussen CH, Mosekilde E, Jørgensen M (2009) Absorption kinetics of insulin after subcutaneous administration. Eur J Pharm Sci 36(1): 78-90.
-
Brange J, Owens DR, Kang S, Volund A (1990) Monomeric insulins and their experimental and clinical implications. Diabetes Care 13(9): 923-954.
-
Kang S, Brange J, Burch A, Volund A, Owens DR (1991) Subcutaneous insulin absorption explained by insulin’ s physiochemical properties. Evidence from absorption studies of soluble human insulin and insulin analogues in humans. Diabetes Care 14(11): 942-948.
-
Heinemann L, Heise T, Jorgensen LN, Starke AA (1993) Action profile of the rapid acting insulin analogue: Human insulin B28Asp. Diabet Med 10(6): 535-539.
-
Howey DC, Bowsher RR, Brunelle RL, Woodworth JR (1994) [Lys (B28), Pro (B29)] - human insulin: A rapidly absorbed analogue of human insulin. Diabetes 43(3): 396-402.
-
Olsen HB, Kjeldsen TB, Balschmidt P, Glendorf T, Havelund S (2011) Rapid acting insulin analogues. US0021423.
-
Langkjaer L (2005) Novel insulin formulations. US0261168.
-
Hirsch IB. Insulin analogues (2005) N Engl J Med 352(2): 174-183.
-
Messadek J (2010) Insulin combinations. US7786077.
-
Bode BW (2007) Use of rapid - acting insulin analogues in the treatment of patients with type 1 and type 2 diabetes mellitus: Insulin pump therapy versus multiple daily injections. Clin Ther 29 (SD): 135-144.
-
Binder C, Lauritzen T, Faber O, Pramming S (1984) Insulin pharmacokinetics. Diabetes Care 7(2): 188-199.
-
Owens DR, Coates PA, Luzio SD, Tinbergen JP, Kurzhals R (2000) Pharmacokinetics of 125 I - labeled insulin glargine (HOE 901) in healthy men: Comparison with NPH insulin and the influence of different subcutaneous injection sites. Diabetes Care 23(6): 813-819.
-
Monami M, Marchionni N, Mannucci E (2008) Long- acting insulin analogues versus NPH human insulin in type 2 diabetes: A meta - analysis. Diabetes Res Clin Pract 81(2): 184 -189.
-
Lee WL, Zinman B (1998) From insulin to insulin analogs: Progress in the treatment of type 1 diabetes. Diabetes Rev 6: 73-88.
-
Rosskamp RH, Park G (1999) Long-acting insulin analogs. Diabetes Care 22(S2): B109-B113.
-
Luzio SD, Owens D, Evans M, Ogunku A, Beck P, et al. (1999) Comparison of the sc absorption of insulin glargine (HOE 901) and NPH human insulin type 2 diabetic subjects. Diabetes 48(S1): A111.
-
Heinemann L, Linkeschova R, Rave K, Hompesch B, Sedlak M, et al. (2000) Time-action profile of the long- acting insulin analog insulin glargine (HOE901) in comparison with those of NPH insulin and placebo. Diabetes Care 23(5): 644-649.
-
Ratner RE, Hirsch IB, Neifing JL, Garg SK, Mecca TE (2000) Less hypoglycemia with insulin glargine in intensive insulin therapy for type 1 diabetes. U.S. Study Group of Insulin Glargine in Type 1 Diabetes Diabetes Care 23(5): 639-643.
-
Rosenstock J, Park G, Zimmerman J (2000) US Insulin Glargine (HOE 901) Type 1 Diabetes Investigator Group. Basal insulin glargine (HOE 901) versus NPH insulin in patients with type 1 diabetes on multiple daily insulin regimens. Diabetes Care 23(8): 1137-1142.
-
Yki-Järvinen H, Dressler A, Ziemen M (2000) HOE 901/300s Study Group. Less nocturnal hypoglycemia and better post-dinner glucose control with bedtime insulin glargine compared with bedtime NPH insulin during insulin combination therapy in type 2 diabetes. Diabetes Care 23(8): 1130-1136.
-
Kurtzhals P (2004) Engineering predictability and protraction in a basal insulin analogue: the pharmacology of insulin detemir. Int J Obesity 28(S2): 23-28.
-
Heinemann L, Sinha K, Weyer C, Loftager M, Hirschberger S, et al. (1999) Time-action profile of the soluble, fatty acid acylated, long-acting insulin analogue NN304. Diabet Med 16(4): 332-338.
-
Barnett AH (2003) A review of basal insulins. Diabet Med 20(11): 873-885.
-
Home P, Bartley P, Russell-Jones D, Hanaire-Broutin H, Heeg JE, et al. (2004) Insulin detemir offers improved glycemic control compared with NPH insulin in people with type 1 diabetes: A randomized clinical trial. Diabetes Care 27(5): 1081-1087.
-
Vague P, Selam JL, Skeie S, De Leeuw I, Elte JW, et al. (2003) Insulin detemir is associated with more predictable glycemic control and reduced risk of hypoglycemia than NPH insulin in patients with type 1 diabetes on a basal- bolus regimen with premeal insulin aspart. Diabetes Care 26(3): 590-596.
-
Sutton G, Minguet J, Ferrero C, Bramlage P (2014)U300, a novel long-acting insulin formulation. Expert Opinion on Biological Therapy 14(12): 1849-1860.
-
Habermann P, Seipke G, Kurrle R, Muller G, Sommerfeld M, et al. (2011) Novel insulin derivatives having extremely delayed time action profile. US0077197.
-
Jonassen I, Jansen TH, Havelund S, Madsen UR, Tagmose TM, et al. (2010) Novel insulin derivatives. US0009899.
-
Mudaliar SR, Lindberg FA, Joyce M, Rave K, Hompesch B, et al. (1999) Insulin aspart (B28 asp-insulin): A fast acting analog of human insulin- absorption kinetics and action profile compared with regular human insulin in healthy non-diabetic subjects. Diabetes Care 22(9): 1501-1506.
-
Heinemann L, Linkeschova R, Rave K, Hompesch B, Sedlak M, et al. (2000) Time-action profile of the long- acting insulin analog insulin glargine (HOE 901) in comparison with those of NPH insulin and placebo. Diabetes Care 23(5): 644-649.
-
Heineman L, Richter B (1993) Richter B. Clinical pharmacology of human insulin. Diabetes Care 16(S3): 90-101.
-
Blair HA, Keating GM (2016) Insulin glargine 300 U/mL: a review in diabetes mellitus. Drugs 76(3): 363-374.
-
Wiesli P, Schories M (2018) Improved glycemic control with insulin glargine 300 U/mL (Toujeo®) in patients with type 2 diabetes: real-world effectiveness in Switzerland. Diabetes Therapy 9(6): 2325-2334.
-
Keating GM (2013) Insulin degludec and insulin degludec/insulin aspart: a review of their use in the management of diabetes mellitus. Drugs 73(6): 575-593.
-
Rendell M (2013) Insulin degludec: a long-acting modern insulin analogue with a predictable pharmacokinetic/ pharmacodynamic profile. Drugs of Today (Barcelona, Spain: 1998) 49(6): 387-397.
-
Riddle MC (2005) Glycemic management of type 2 diabetes: An emerging strategy with oral agents, insulins, and combinations. Endocrinol Metab Clin N Am 34(1): 77-98.
-
Feinglos MN, Thacker CH, English J, Bethel MA, Lane JD (1997) Modification of postprandial hyperglycemia with insulin lispro improves glucose control in patients with type 2 diabetes. Diabetes Care 20(10): 1539-1542.
-
UK Prospective Diabetes Study (UKPDS) Group (1998) Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). The Lancet 352(9131): 854-865.
-
Riddle MC (2004) Timely initiation of basal insulin. Am J Med 116(3A): 3S-9S.
-
Yki-Jarvinen H, Kauppila M, Kujansuu E, Lahti J, Marjanen T, et al. (1992) Comparison of insulin regimens in patients with non-insulin-dependent diabetes mellitus. N Engl J Med 327(20): 1426-1433.
-
Kennedy L, Herman WH, Strange P, Harris A, Goal A1C Team (2006) Impact of active versus usual algorithmic titration of basal insulin and point-of-care versus laboratory measurement of HbA1c on glycemic control in patients with type 2 diabetes: the Glycemic Optimization with Algorithms and Labs at Point of Care (GOAL A1C) trial. Diabetes Care 29(1): 1-8.
-
Roach P, Woodworth JR (2002) Clinical Pharmacokinetics and pharmacodynamics of insulin lispro mixtures. Clini Pharmacokinet 41(13): 1043-1057.
-
Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, et al. (2009) Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes care 32(1): 193-203.
-
Meier JJ (2012) GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nature Reviews Endocrinology 8(12): 728-742.
-
Yeh HC, Brown TT, Maruthur N, Ranasinghe P, Berger Z, et al. (2012) Comparative effectiveness and safety of methods of insulin delivery and glucose monitoring for diabetes mellitus: a systematic review and meta- analysis. Annals of internal medicine 157(5): 336-347.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance