Validation of Patient-Oriented Risk Assessment Tool in Indian Patients with Obesity: Results from the Large-Scale Evaluation of the Novel Concept Tool
Aim and Background: The global upsurge of the obesity epidemic has led to an urgent need for measurement tools for obesity research and practice. Patient-oriented tools are important for determining the effectiveness of management and treatment of obesity. The current study objective was to evaluate the clinical validity of an obesity risk assessment tool in a large sample of patients suffering from obesity in India. Methods: This study was conducted between August 2021-August 2022 in which a user-friendly, patient-oriented obesity risk assessment questionnaire was digitally administered to patients suffering from obesity. Data was analysed using a multivariate ordered logistic regression model (OLM), and discriminant analysis was performed to validate the model’s predictability. Results: The questionnaire was completed by 1046 patients includes 639 (61.09%) female and 407 (38.91%) male participants. The mean age of patients was 41.29±12.4 years (age range: 15–97 years), and the mean BMI was 46.75±19.41 kg/m2. The ordered regression model predicted bariatric surgery for 66.63% of patients, diet and exercise for 6.9%, and pharmacotherapy for 4.6% of patients. Overall, our findings suggest that the model had an accuracy of 78%, providing evidence for the validity of the tool and suggesting next action steps to be taken by patient. Conclusion: The obesity risk assessment tool has potential as a patient-oriented tool because of its ease of use for the assessment and providing guidance to seek next steps for appropriate management of obesity. It can be applied to both sexes at all ages and may provide the simplest and most valid risk assessment tool to enable patients to move from awareness to action.
Introduction
Obesity is reaching epidemic proportions globally and has been observed across all ages, genders, ethnic and socio- economic groups. In developing countries like India, the prevalence of obesity has been forecasted to reach 9.5% among men and 13.9% among women by 2040 [1]. This upsurge in the burden of obesity is believed to be largely driven by the country’s rapid urbanization and the adoption of western lifestyles such as reduced physical activity and high-calorie diet consumption. Even more worrying, the increase in obesity prevalence will contribute to several metabolic aberrations that increase risk for cardiovascular diseases, type 2 diabetes, cancers, and other conditions [2]. This upward trend in the levels of obesity have led to an increased need for measurement tools for research, management, and treatment of these patients.
Overweight and obesity are usually evaluated using the body mass index (BMI) in clinical settings [3]. However, evidence suggests that BMI and anthropometric measurements are unreliable target indices that do not accurately reflect the presence or severity of obesity-related health risks, and hence, are inadequate for guiding effective treatment interventions [4]. This has led to the development of clinical staging systems to assist in the clinical decision- making process for obesity treatments. Of these, the most practical and popular is the Edmonton Obesity Staging System (EOSS) which is a novel risk-stratification tool that evaluates obesity related comorbidities into 5 graded categories, based on their morbidity and health-risk profile [5]. Several studies have confirmed its clinical utility based on its prediction of complications following surgical and non-surgical weight loss, health service usage, and mortality compared to BMI [6, 7, 8]. However, the application of EOSS is mainly clinician- driven and its use in routine clinical practice is hampered, particularly due to the fact that patients’ life context is not integrated in its clinical assessment. Conversely, while self- reported online BMI calculators are widely used by patients which provide an excellent indicator of overweight and obesity, these BMI calculators fall short in directing patients to next appropriate action steps. Thus, it is imperative to facilitate the use of patient-friendly and user-friendly tools and craft more patient-centered means of evaluation and management of obesity.
We have previously aimed to address this limitation by developing an obesity risk assessment concept after considering all the patient-related factors that can be used directly by patients without the need for expert advice [9]. This concept note, which was published in January 2021, was validated by key opinion leaders (KOLs) conceptually. Furthermore, we have evaluated the predictability of the tool by piloting it in a small sample population, thereby facilitating its relative importance at the individual level. The questionnaire which could be easily administered to patients, provides a more economical and reliable framework for the assessment of the level of obesity, identifies the risks, and simplifies the appropriate obesity management pathway [9]. Though the preliminary findings of this tool are promising, it is necessary to assess its clinical reliability on a large- scale population in order to determine its usability as an individually tailored, patient-centric tool for the management of obesity and promotion of population health. The objective of this study is to evaluate the performance of the obesity risk assessment questionnaire and report on the clinical reliability of this patient-oriented risk assessment concept in a larger sample, with the aim of further establishing its usefulness as a health assessment tool for obesity.
Materials and Methods
Study Design and Participants
This survey-based study was conducted in August 2021-August 2022, involving patients suffering from obesity across different regions of India. The novel obesity risk assessment questionnaire was digitally administered among 1046 patients, after conducting a pilot study among 21 participants for validation. Informed consent was obtained from all participants. Privacy and confidentiality were respected, and access to all files was limited to the research team.
Questionnaire
The obesity risk assessment scale is a simplified, patient- oriented tool based on the EOSS clinical staging system that provides risk assessment related to obesity [Appendix I]. The tool is developed by generating a number of items by performing an extensive literature review of articles for a wide range of patient related risk factors for obesity such as age, BMI, physical limitations, presence of comorbidities, quality of life, mental health, mechanical, and genetic factors. The initial concept validation of the tool was performed using a two-phase Delphi method with five experts from different regions of India, where the questionnaire and weightage for each respective question were finalized [9]. The calculated weights for each variable are presented in Appendix II.
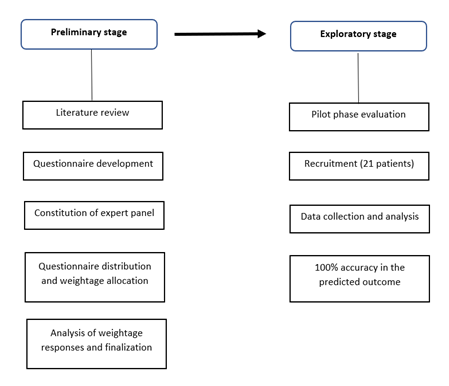
Furthermore, a pilot study using logistic regression was conducted between August 2021 and September 2021 to validate the questionnaire and predict its suitability for large scale evaluation. The findings from the pilot phase suggest that this is an easy to complete, patient-friendly, and self- reporting tool with 100% accuracy in predicting the outcome and provides value in assessing multiple risk factors for obesity. The construction, finalization, and preliminary validation of the obesity risk assessment questionnaire took place in two distinct stages (Figure 1).
Data Analysis
The baseline variables such as age, weight, height, and BMI were summarized using percentage values. In addition, summary statistics were calculated with the mean values, wherever applicable. A multivariate ordered logistic regression model (OLM) was fitted, to get the model coefficient for the predicted treatment outcomes (Appendix III). To validate the model predictability, discriminant analysis for classification was performed. Data analysis was conducted using the IBM SPSS statistics software version 20 (IBM Corp, Armonk, NY: IBM Corp).
Results
A total of 1046 patients suffering from obesity responded to the questionnaire, of which 639 (61.09%) were females and 407 (38.91%) were males. Mean age of patients was 41.29±12.4 years (age range: 15–97 years) and the mean BMI was 46.75±19.41 kg/m2. Mean height (cm) and weight (kg) of the patients was 161.87±9.48 and 113.24±27.58, respectively.
| Sample (N=1046) | n (%)/Mean ± SD | Min - Max |
|---|---|---|
| Female (n, %) | 639 (61.09%) | |
| Male (n, %) | 407 (38.91%) | |
| Age (In Years) | 41.29 ± 12.40 | 15 - 97 |
| Weight (In Kg) | 113.24 ± 27.58 | 56 - 255 |
| Height (In cm) | 161.87 ± 9.48 | 125 - 193 |
| BMI (In Kg/m2) | 46.75 ± 19.41 | 19.15 - 96 |
Table 1: ** Background characteristics of the participants.
BMI: Body Mass Index. Table 1: Background characteristics of the participants.
An OLM is used to investigate the influence of various determinants on the predicted treatment outcomes. In Appendix III, the coefficients of the model are displayed and the regression with the coefficients offers a first insight of the sign and significance of the variables on model output. Based on the final scores of OLM predictions, patients’ final assessment scores were calculated and the criteria for the appropriate management of obesity is classified (Table 2). Patients with a final OLM score of <1.12 are recommended to follow a diet and exercise program, and patients with a score of 1.12 – 2.34 are recommended to consider pharmacological treatment. Patients with a final OLM score of >2.35 are recommended to consider bariatric surgery.
Case Example
For example, consider a female patient aged 35-60 years, with multiple comorbidities and a family history of obesity.
$$ G e n d e r = F E M A L E, \quad A g e = 3 5 - 6 0, \quad B M I = 3 5 - 3 9, $$
Breathlessness=OCCASIONALLY, Sleep (OSA) = FREQUENTLY,
Depression=ALMOST EVERYDAY, Type 2 Diabetes =YES,
$$ \text{Hypertension} = \text{YES}, \text{Joints Health issues} = \text{YES}, \text{PCOS} / $$
Infertility=YES, Family History =YES
Score = -0.4714 - 0.3104 + 2.0114 + 0.7802 + 0.6001 + 0.4134 + 0.8461 + 0.4322 + 0.5585 + 0.5311 + 0.2760 = 5.67 The preceding case example demonstrates that bariatric surgery is the recommended treatment modality to consider as an associated intervention for the management of obesity.
| Classification criteria | |
|---|---|
| <1.12 | Diet and Exercise |
| 1.12 – 2.34 | Pharmacotherapy |
| >2.35 | Bariatric Surgery |
Table 2: Total score and the classification criteria.
Based on the discriminant analysis for categorization, we have evaluated the model’s predictive abilities to see how well it can correctly predict the outcomes of treatments such as diet and exercise, pharmacotherapy, and bariatric surgery. Of 1046 participants, three patients’ observed category data were not available. By using an ordered regression model, we found that we could correctly predict bariatric surgery for 66.63% of patients, diet and exercise, and pharmacotherapy for 6.9% and 4.6% of patients, respectively. The findings showed that the model had an overall accuracy of 78%, indicating that it was effective in predicting the outcome variable (Table 3).
| Predicted Category | Total | ||||
|---|---|---|---|---|---|
| Diet and Exercise | Pharmacotherapy | Bariatric Surgery | Total | ||
| Observed Category | Diet and Exercise | 72(6.9%) | 46(4.41%) | 58(5.56%) | 176(16.87%) |
| Pharmacotherapy | 38(3.64%) | 48(4.6%) | 33(3.16%) | 119(11.41%) | |
| Bariatric Surgery | 11(1.05%) | 42(4.03%) | 695(66.63%) | 748(71.72%) | |
| Total | 121(11.6%) | 136(13.04%) | 786(75.36%) | 1043(100%) |
Table 3: ** Discriminant analysis for classification.
*Three patients observed category data were not available. Table 3: Discriminant analysis for classification.
Discussion
Self-reported risk assessment tools will remain crucial in assessing patients’ health and determining the most effective treatments for obesity due to the growing number of patients suffering from obesity worldwide, especially in India. This extensive follow-up to pilot research of a risk assessment tool measuring multiple patient related factors for obesity has demonstrated the tool’s good predictive power and potential utility in evaluating these factors in relation to obesity management. To our knowledge, the obesity risk assessment tool is one of the few patient-facing tools that individuals can use to evaluate their obesity without professional assistance.
Obesity risk assessment is an important step in the management process and is paramount to designing individualized and targeted treatment procedures. The diagnostic and predictive power of different anthropometric measures of obesity and obesity‐related comorbidities is still a matter of continuous debate [10, 11]. Recognizing the escalating challenge of obesity, several guidelines highlighted the need for comprehensive clinical assessment using classification based on BMI and stage of disease [12]. EOSS is one such clinical staging system that considers physical, psychological, and metabolic parameters to determine the optimal obesity treatment [5]. However, EOSS is clinician oriented and is mainly undertaken by clinicians or obesity practitioners. Assessing the risk of obesity using measures most relevant to obesity patients in their everyday lives can provide greater importance for the successful management of surgery. In fact, previous research using self-reported data on anthropometric measures demonstrated high accuracy rates and was associated with successful outcomes [13]. The obesity risk assessment scale used in this study allows patients to understand their level of obesity, identify the risks, and suggest the stratified action for an appropriate obesity management pathway.
As the cause of obesity is multifaceted, multiple modalities of treatment, including lifestyle modifications such as diet and exercise, pharmacotherapy, and bariatric surgery, should be considered for its management [14, 15, 16, 17]. Implications of this obesity risk assessment validation study include contributing to the body of literature on the use of objective patient related factors such as age, BMI, physical limitations, presence of comorbidities, quality of life, mental health, mechanical, and genetic factors for robust validation and to expand their value in the guidance of treatment modalities. The accuracy came out of the ordered logistic regression model with a value of approximately 78%. Following a large number of research articles, we observed that there has been a tremendous amount of work done for predicting the risk of obesity using machine learning regression models, particularly in children. The accuracy rates of the proposed obesity risk assessment systems in these studies were reported at 85% [18] and 81.8% vs 76.1% (girls vs. boys) [19]. In line with these findings, it appears that our accuracy of 78% is relatively comparable to predicting the treatment outcome, which is deemed to be a satisfactory result. Using our model, patients will be able to correlate the objective effect of related factors and the associated management option with considerable reliability, based on each patient’s own profile. This study is also rewarding because it established a model that can present a well-calibrated probability that has a practical meaning for the users.
The limitations of this study warrant consideration. We must not forget that the data from the questionnaire are self- reported, which may be subject to biased reporting. Another limitation is the cross-sectional design of the study, which makes detecting causal inferences difficult. The strengths of our study include the use of objective robust analytical approaches to establish the validity of the tool. Further, our data is the representation of patients with obesity from different classes and age-groups in the Indian context. While our conclusions are not generalizable to all patients living with obesity, they are foundational to the wide-ranging application of the tool and to establishing its appropriateness as next step to patient awareness to patients initiating action to address the issues with obesity.
Conclusion
Our findings reveal that although many clinician-driven assessment tools have emerged in the assessment of obesity, to our knowledge, there is no single patient centric method adequate for the evaluation of obesity directly by patients in India. The logistic regression model showed notable results in predicting treatment outcomes with an accuracy of 78%. The obesity risk assessment tool may be instrumental in directing patients to seek further steps in the appropriate management of obesity. We hope that our research will likely contribute to scalable improvements in the standards of care for obesity in the Indian health care system. However, we suggest prospective long-term studies be carried out to confirm the results of this study and to describe the variation in the results for individual regions.
Funding
The present study supported by Ethicon, a part of Johnson & Johnson Private Limited.
References
-
Luhar S, Timæus IM, Jones R, Cunningham S, Patel SA, et al. (2020) Forecasting the prevalence of overweight and obesity in India to 2040. PLoS One 15(2): e0229438.
-
National Institutes of Health (2000) The Practical Guide Identification, Evaluation, and Treatment of Overweight and Obesity in Adults.
-
Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, et al. (2014) 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 129(25-S2): S102-S138.
-
Gurunathan U, Myles PS (2016) Limitations of body mass index as an obesity measure of perioperative risk. Br J Anaesth 116(3): 319-321.
-
Sharma AM, Kushner RF (2009) A proposed clinical staging system for obesity. Int J Obes (Lond) 33(3): 289- 295.
-
Atlantis E, Sahebolamri M, Cheema BS, Williams K (2020) Usefulness of the Edmonton Obesity Staging System for stratifying the presence and severity of weight-related health problems in clinical and community settings: A rapid review of observational studies. Obes Rev 21(11): e13120.
-
Janssen I, Katzmarzyk PT, Ross R (2004) Waist circumference and not body mass index explains obesity- related health risk. Am J Clin Nutr 79(3): 379-384.
-
Kuk JL, Ardern CI, Church TS, Sharma AM, Padwal J, et al. (2011) Edmonton Obesity Staging System: association with weight history and mortality risk. Appl Physiol Nutr Metab 36(4): 570-576.
-
Bhaskar AG, Peters A NC, Jammu G S, Ravikanth K, Khaitan M, et al. (2021) Obesity Risk Assessment Concept. Diabetes Obes Int J 6(1): 000238.
-
Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, et al. (1990) A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr 51(2): 241-247.
-
Frankenfield D, Roth-Yousey L, Compher C (2005) Comparison of predictive equations for resting metabolic rate in healthy nonobese and obese adults: a systematic review. J Am Diet Assoc 105(5): 775-789.
-
Wharton S, Lau DCW, Vallis M, Sharma AM, Biertho L, et al. (2020) Obesity in adults: a clinical practice guideline. CMAJ. 192(31): E875-E891.
-
Harvey-Berino J, Krukowski RA, Buzzell P, Ogden D, Skelly J, et al. (2011) The accuracy of weight reported in a web-based obesity treatment program. Telemed J E Health 17(9): 696-699.
-
Jakicic JM (2009) The effect of physical activity on body weight. Obesity (Silver Spring) 17(S3): S34-S38.
-
Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, et al. (2009) American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc 41(2): 459-471.
-
Bray GA, Ryan DH (2012) Medical therapy for the patient with obesity. Circulation 125(13): 1695-1703.
-
Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, et al. (2004) Bariatric surgery: a systematic review and meta-analysis. JAMA 292(14): 1724-1737.
-
Dugan TM, Mukhopadhyay S, Carroll A, Downs S (2015) Machine Learning Techniques for Prediction of Early Childhood Obesity. Appl Clin Inform 6(3): 506-520.
-
Hammond R, Athanasiadou R, Curado S, Aphinyanaphongs Y, Abrams C, et al. (2019) Predicting childhood obesity using electronic health records and publicly available data. PLoS One 14(4): e0215571.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance