Consequence of Diabetes, Obesity and Atherosclerosis in the Episodes of Impaired Dental Health: A Brief Review on Periodontitis
Periodontium refers to the supporting tooth structures which keep the tooth intact in its position for chewing, speaking, etc. Microbial infection can cause complex inflammation on the gum of the teeth and thus affects the supporting tooth structures. Reports from the survey on dental health and hygiene have shown that the intrusion of such inflammation might have detrimental effects both at local and global level. Diabetes and obesity plays a significant role in the severity of periodontal infection. It is documented that periodontal intervention can potentially improve glycemic standard. In fact, there is a bidirectional relationship between T2DM and periodontitis. Diabetic subjects are more prone in periodontitis related complications than non-diabetics. Since diabetes is a common co-morbidity in obese people; bone loss and periodontitis are even found interlinked with diabetes and obesity. Like diabetes and obesity, periodontitis is also found to be prone to atherosclerotic burst in many occasions. This article represents a brief review on the link of the local lesion, called periodontitis, to the global effects viz. diabetes, obesity and atherosclerosis, the co-morbidities that can even flare up cardiovascular complications.
Introduction
Periodontitis in general a disease of concern with dental health and its unhygienic maintenance but, pre- existence of morbidities like diabetes and obesity may also be the cause of ministering the onset of this microbe infected pathogenesis at teeth periphery. Besides poor dental hygiene, the link between diabetes, obesity and periodontitis is now extensively studied and reported [1, 2, 3, 4, 5, 6, 7, 8]. An additional link of developing atherosclerosis, in cases of long run suffering with periodontitis, is also an emerging area in the prevailing dental research [9] Associated co- morbidities like diabetes and obesity in the incidence of periodontitis can flare up the atherosclerotic affair even at a more critical end of systemic health including cardiovascular impairments and heart attack [10, 11]. In reality, there are two types of periodontitis e.g. staged and aggressive variety. While staged periodontitis can be graded as per the stage of severity, the aggressive periodontitis is the most critical situation associated very seriously with other ailments like atherosclerosis and cardiovascular disease. The prevalence of atherosclerosis and cardiovascular disease in staged and aggressive periodontitis infection from adolescent to older population is among the highest reported concern in the survey of dental health worldwide.
Periodontitis: A Complex Inflammation of Teeth
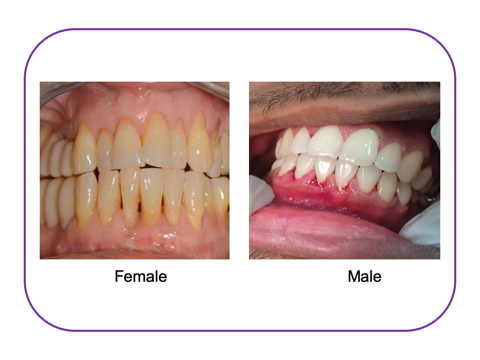
Periodontitis (PD) is a chronic inflammatory disease of the surrounding tissues of the teeth [12] (Figure-1). The most common illness of periodontium, the supporting tooth structures, is the inflammation in teeth scaffold beneath gingiva and called as periodontitis which leads to pocket formation, bone destruction and loosening of teeth. PD is an outcome of the growth of periopathogens in oral biofilm through complex pathogen–host interactions [12, 13]. PD affects up to 90% of the worldwide population and is ranked the sixth most prevalent disease in humans [12]. In fact, periodontitis is not an infection caused by any single type of microorganism; rather, a group of bacteria is involved in this infection. The long lasting pathogenic bacteria such as porphyromonas gingivalis and aggregatibacter actinomycetemcomitans with many others adhere to the oral scaffolds for long, causing a permanent lesion over the teeth-supporting gum. The deterioration of affected periodontium gets accelerated in presence of systemic diseases such as poorly controlled diabetes, diabetic obesity, immunocompromised conditions, mental stress and many others among which atherosclerosis is a major partner. Recent concerns on dental health around the world have shown the incidence of cardiovascular disorders in subjects having periodontitis [11]. Sanz, et al. has shown independent associations between severe periodontitis and cardiovascular mortality in several different populations [14]. Atherosclerosis is a chronic progressive narrowing of arteries that may lead to their occlusion due to lipid deposition and atheroma formation in the arterial wall [15]. This kind of abnormality in the peripheral blood vessels around the teeth structure may be a reason to adopt the infectious organisms in the periphery of teeth resulting in the occurrence of periodontitis. The link between periodontal disease and atherosclerosis was first introduced in 1963 when a 25% higher risk of atherosclerotic plaque formation in patients with periodontitis was demonstrated [16]. Since then, there are growing evidences regarding the contribution of chronic periodontal inflammation to the risk of atherosclerosis [16, 17, 18, 19, 20]. Although the exact mechanism of this association is not yet very transparent and likely to be very complex; there are at least two accepted models: microbial invasion and infection of atheromas, or inflammatory/immunological mechanisms [16].
Atherosclerosis: A Potential Outcome in the Severity of Periodontitis
Atherosclerosis is the process of atherogenesis that results in endothelial dysfunction, arterial stiffness, and hypertension causing ultimately an ischemic event which can worsen the life process [17, 18, 19, 20, 21]. A notable portion of periodontitis infected subjects are found prone to cardiovascular disease (CVD), a post event incidence of endothelial dysfunction in cases of persistent periodontitis episode. In many occasions periodontal therapy provided partial relief to atherosclerotic condition and fairly improved endothelial function [22] without any clearly known reason.
Studies have correlated incidence of graded association between stroke, cardiovascular death, stable coronary artery disease and tooth loss in periodontitis affected subjects [23]. Bacteraemia, due to poor oral hygiene may result in bacterial growth over atherosclerotic coronary artery plaques within the blood vessels and worsen coronary artery disease condition [24]. Therefore, it is apparent that periodontitis may be a modifiable non-traditional risk factor for CVD. To explain the association between periodontal ailment and atherosclerosis, several mechanisms have been studied, both locally (within mouth cavity) and on systemic immune responses. Systemic inflammatory incident or immune response to periodontal infection, has been found to increase the cardiovascular risk.
Microbes (Porphyromonas gingivalis) from the oral cavity via blood stream may enter the atherosclerotic plaques, and which in turn can promote an inflammatory or immune response within the atherosclerotic plaque. This pathogen increases the atherosclerotic plaque volume with the accumulation of cholesterol esters and inflammatory mediators.
Oxidative stress plays a central role in the pathogenesis of apical periodontitis (AP) and its association with atherosclerosis [25].
Diabetes, Obesity and Periodontitis: The Fostering Arms of Atherosclerosis
Impairment of insulin action against the backdrop of insulin resistance characterizes type 2 diabetes mellitus (T2DM). Insulin resistance and T2DM are linked with atherosclerotic diseases. It is now reported that insulin resistance and atherosclerosis have identical genetic roots [26]. From the perspective of cardio- and cerebrovascular risk, diabetes and atherosclerosis are two complementary conditions. Beyond common characteristics like inflammation and oxidative stress, there are numerous molecular mechanisms through which they reinforce one another. Early signs of insulin resistance-detected endothelial dysfunction (ED) may be the cause of the development of atherosclerosis. Pro-inflammatory cytokines encoding genes are affected in the cases of ED. Potential genetic indicators of insulin resistance and atherosclerosis include single nucleotide variants (SNPs) of those genes themselves [27]. Chronic hyperglycemia and advanced glycosylation end- products (AGE) promote “accelerated atherosclerosis” by causing endothelial damage and cellular dysfunction. The risks of having cardio- and cerebrovascular events are found to be obvious as a result of atherosclerosis within the vascular system; the proof of this strong correlation dates back several decades in the post era of 1970s [26].
Risk factors include smoking, physical inactivity, poor nutrition, high blood pressure, type 2 diabetes, dyslipidemia, and obesity. Obesity is a major risk factor for arteries and the primary cause of obstructive sleep apnea (OSA). OSA is a separate CVD risk factor [28, 29, 30].
Obesity is a disease brought on by the abnormal or excessive accumulation of adipose tissue which results in variety of metabolic disorders and illnesses, such as insulin resistance and atherogenic dyslipidemia. The risk of getting type 2 diabetes increases over the time in tandem with an increase in BMI, which serves as an indicator of adiposity [31].
Cardiovascular disease caused by microvascular and macrovascular malfunctioning is the main factor in the incidence and mortality of diabetics. Hypertension and other comorbidities, such as obesity and dyslipidaemia, worsen the vascular consequences of diabetes [32].
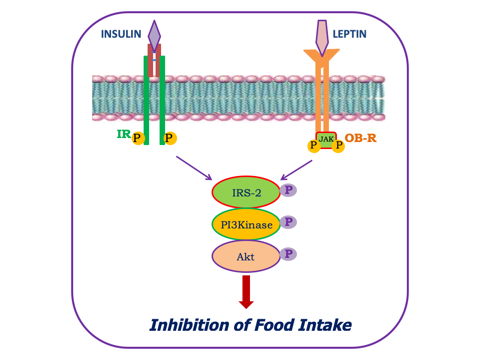
Being a member of metabolic syndrome-X, obesity entangles hyperglycemia and dyslipidemia [33, 34, 35, 36] over the period of time. In human obesity hyperleptinemia and leptin resistance are inevitable [33, 34, 37, 38, 39] phenomenon. Since insulin and leptin shares a common IRS2-PI3K-Akt mediated signaling path (Figure-2) for their mechanism of action; inactivity of this signalling route makes the receptors of both the ligands resistant to their activity. Hence hyperleptinemia and hyperinsulinimia are the simultaneous phenomenon in human obesity. It has been documented in an earlier report that hyperinsulinimia associated insulin resistance is an outcome of the incidence of IR-LDLR (IR: insulin receptor, LDLR: LDL receptor) interlocking [40, 41]. Thus, the inter-association of insulin resistance with increasing concentration of leptin with the progress of human obesity strengthens the impact of IR-LDLR complex [42] that leads the complexities related to atherosclerosis. It is also reported that insulin receptor tyrosine kinase activity also gets reduced because of reduced expression of receptor associated tyrosine kinase protein in human obesity [43]. This is the other reason of insulin resistance and favouring the chances of strengthening IR-LDLR association. In most cases, type-2 diabetes is an associated incidence of human obesity and IR-LDLR complex association is the characteristic feature of type-2 diabetes [43]. Thus IR-LDLR association is also a leading earmark for developing atherosclerosis in the backdrop of the illness in human obesity. Since periodontitis is a trader for atherosclerosis; diabetes and obesity will be the co-fuel for increasing atherosclerotic severity. In fact, diabetes will also be a fuel for microbial growth on the wound of periodontium. Thus the synergistic effect of diabetes and obesity in conjugation with periodontitis will exploit the atherosclerotic events of dental ailment.
Does Periodontitis Costs Atherosclerosis or Vice Versa?
It has been a long time question whether periodontitis precipitates atherosclerosis or atherosclerosis makes environment for infecting organisms to develop periodontitis. Extensive research on dental health has finally explored out that the persistent and resistant form of periodontitis can act as the risk factor for atherosclerosis [44, 45, 46]. Millions of people world wide, adolescent, young and old, are now affected with either staged (SPD) or aggressive type of periodontitis (AgPD) [47, 48, 49]. Follow up of periodontitis patients have documented that many of these subjects in long run developed atherosclerosis [50]. On the other hand, dental health survey in patients with coronary heart attack has shown pre-existed old lesions of periodontitis [20]. For decades, researchers have probed the plausible links between periodontitis and cardiovascular health [51, 52]. Actually periodontal disease increases the body’s burden of inflammation. Atherosclerosis is a disease of inflammatory molecules. In fact, bacteria infected acute inflammation in periodontitis involves an outpouring of immune cells that attack irritants and microbial invader causing a stable lesion on the gingival periphery. Persistence of periodontitis induced chronic inflammation may be a key contributor for augmenting atherosclerosis among many other health problems; of course a genetic susceptibility for contributing atherosclerosis and poor cardiovascular health in periodontitis infected subjects may not be ignored [53, 54, 55].
Discussion and Conclusion
This review is an excerpt of the prevailing reports on periodontitis and the associated severities in the affairs of pre- and post-comorbidities. One emerging phenomenon of dental research focuses on the events of atherosclerosis [9, 16] in cases of persisting ailment like periodontitis. The severity of atherosclerosis can even go up to the stage of cardiovascular abnormalities [10, 11, 19, 20]. The incidence of periodontitis onset atherosclerosis can also get exaggerated in the cases of pre-existed diabetes and obesity in those infection affected subjects. On the other hand, interventions to periodontitis affected diabetic subjects have shown improvement of their glycemic status [1]. A bidirectional relationship between type-2 diabetes mellitus and periodontitis has been found apparent in latest report of dental research [3]. Since obesity is also a detrimental co-morbidity for periodontitis [2], medical professionals in their therapeutic intent should try to prevent periodontitis by controlling patient body mass. The compelling pattern of increased risk of periodontitis in overweight or obese individuals has proved a consistent co-association between obesity and periodontitis [7]. Although the exact mechanism is not yet clear, the associated chronic inflammatory state and oxidative stress during the course of diabetes and/or obesity are assumed to be the expected reasons to malaise the pathophysiology of periodontal infection to the more harmful situation.
References
-
Rapone B, Ferrara E, Corsalini M, Qorri E, Converti I, et al. (2021) Inflammatory Status and Glycaemic Control Level of Patients with Type 2 Diabetes and Periodontitis: A Randomized Clini-cal Trial. Int J Environ Res Public Health 18(6): 3018.
-
Kim CM, Lee S, Hwang W, Son E, Kim TW, et al. (2022) Obesity and periodontitis: A systematic review and updated meta-analysis. Front Endocrinol 13: 999455.
-
Wu C, Yuan Y, Liu H, Li S, Zhang B, et al. (2020) Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral Health 20: 204.
-
Baeza M, Morales A, Cisterna C, Cavalla F, Jara G, et al. (2020) Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta- analysis. J Appl Oral Sci 28: e20190248.
-
Nibali L, Gkranias N, Mainas G, Pino AD (2022) Periodontitis and implant complications in diabetes. Periodontology 2000; 90(1): 88-105.
-
Arboleda S, Vargas M, Losada S, Pinto A (2019) Review of obesity and periodontitis: an epidemiological view. British Dental Journal 227(3): 235-239.
-
Martinez-Herrera M, Silvestre-Rangil J, Silvestre FJ (2017) Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med Oral Patol Oral Cir Bucal 22 (6): e708-715.
-
Zhao P, Xu A, Leung WK (2022) Obesity, Bone Loss, and Periodontitis: The Interlink. Biomolecules 12(7): 865.
-
Herrera D, Molina A, Buhlin K, Klinge B (2020) Periodontal diseases and association with atherosclerotic disease. Periodontology 2000; 83(1): 66-89.
-
Doughan M, Chehab O, de Vasconcellos HD, Zeitoun R, Varadarajan V, et al. (2023) Periodontal Disease Associated With Interstitial Myocardial Fibrosis: The Multiethnic Study of Atherosclerosis. JAHA 12(3): e8146.
-
Czerniuk MR, Surma S, Romańczyk M, Nowak JM, Wojtowicz A, et al. (2022) Unexpected Relationships: Periodontal Diseases: Atherosclerosis–Plaque Destabilization? From the Teeth to a Coronary Event. Biology 11(2): 272.
-
Newman MG, Takei HH, Klokkevold PR (2019) Clinical Periodontology. In: 13th (Edn.), Fermin A Carranza (Ed.), Elsevier Inc.
-
Fleming TF (1999) Periodontitis. Ann Periodontol 4(1): 32-38.
-
Sanz M, Castillo AMD, Jepsen S, Gonzalez-Juanatey JR, D’Aiuto F, et al. (2020) Periodontitis and cardiovascular diseases: Consensus report. J Clin Periodontol 47(3): 268-288.
-
Alsalleeh F, Alhadlaq AS, Althumiri NA, AlMousa N, BinDhim NF (2023) Public awareness of the association betwee Periodontal Disease and Systemic Disease. Healthcare 11(1): 88.
-
Schenkein HA, Papapanou PN, Genco R, Sanz M (2020) Mechanisms underlying the association between periodontitis and atherosclerotic disease. Periodontology 2000; 83(1): 90-106.
-
Piconi S, Trabattoni D, Luraghi C, Perilli E, Borelli M, et al. (2008) Treatment of periodontal disease results in improvements in endothelial dysfunction and reduction of the carotid intima-media thickness. FASEB J 23(4): 1196-1204.
-
Awan Z, Genest J (2015) Inflammation modulation and cardiovascular disease prevention. Eur J Prev Cardiol 22(6): 719-733.
-
Nicolosi LN, Lewin PG, Rudzinski JJ, Pompeo M, Guanca F, et al. (2017) Relation between periodontal disease and arterial stiffness. J Periodontal Res 52(1): 122-126.
-
Wojtkowska A, Zapolski T, Wysoki ́nska-Miszczuk J, Wysoki ́nski AP (2021) The inflammation link between periodontal disease and coronary atherosclerosis in patients with acute coronary syndrome: Case-control study. BMC Oral Health 21(1): 5.
-
Teeuw WJ (2017) Periodontitis, diabetes mellitus, cardiovascular disease: a Bermuda triangle. Nederlands Tijdschrift Voor Tandheelkunde 124(10): 511-513.
-
Han YW, Houcken W, Loos BG, Schenkein HA, Tezal M (2014) Periodontal disease, atherosclerosis, adverse pregnancy outcomes, and head-and-neck cancer. Advances in dental research 26(1): 47-55.
-
Stewart R, West M (2016) Increasing evidence for an association between periodontitis and cardiovascular disease. Circulation 133(6): 549-551.
-
Priyamvara A, Dey AK, Bandyopadhyay D, Katikineni V, Zaghlol R, et al. (2020) Periodontal inflammation and the risk of cardiovascular disease. Current atherosclerosis reports 22(7): 28.
-
Hernández-Ríos P, Pussinen PJ, Vernal R, Hernández M (2017) Oxidative stress in the local and systemic events of apical periodontitis. Frontiers in Physiology 8: 869.
-
Perumalsamy S, Huri HZ, Abdullah BM, Mazlan O, Wan Ahmad WA, et al. (2023) Genetic Markers of Insulin Resistance and Atherosclerosis in Type 2 Diabetes Mellitus Patients with Coronary Artery Disease. Metabolites 13(3): 427.
-
Maida CD, Daidone M, Pacinella G, Norrito RL, Pinto A, et al. (2022) Diabetes and Ischemic Stroke: An Old and New Relationship an Overview of the Close Interaction between These Diseases. International Journal of Molecular Sciences 23(4): 2397.
-
Poznyak AV, Sadykhov NK, Kartuesov AG, Borisov EE, Melnichenko AA, et al. (2022) Hypertension as a risk factor for atherosclerosis: Cardiovascular risk assessment. Front Cardiovasc Med 9: 959285.
-
Touyz RM, Eluwole O, Livia L, Francisco JR, Alves-Lopes R, et al. (2023) Molecular Mechanisms Underlying Vascular Disease in Diabetes. In: Berbari AE, Mancia G (Eds.), Blood Pressure Disorders in Diabetes Mellitus. Updates in Hypertension and Cardiovascular Protection. Springer pp: 105-118.
-
Cai PY, Zheng YL, Zhou YF, Li MM, Shi YC, et al. (2022) Research progress on the role of exosomes in obstructive sleep apnea-hypopnea syndrome-related atherosclerosis. Sleep Medicine Reviews 17: 101696.
-
Klein S, Gastaldelli A, Yki-Järvinen H, Scherer PE (2022) Why does obesity cause diabetes?. Cell metabolism 34(1): 11-20.
-
Meng H, Ruan J, Chen Y, Yan Z, Liu J, et al. (2023) Trace Elements Open a New Direction for the Diagnosis of Atherosclerosis. Rev Cardiovasc Med 24(1): 23.
-
Beriwal P, Chandra NC (2020) Human obesity: A noxious sequel of inverse intents of ligands and receptors. Diabetes Obes Int J 4(4): 1-12.
-
Beriwal P, Chandra NC (2020) Hyperlipidimia, hyperleptinemia and insulin resistance: Intercorrelation with obesity. Diabetes Obes Int J 5(1): 1-6.
-
Al-Goblan AS, Al-Alfi MA, Khan MZ (2014) Mechanism linking diabetes mellitus and obesity. Diabetes Metab Syndr Obes 7: 587-591.
-
Klop B, Elte JWF, Cabezas MC (2013) Dyslipidemia in obesity: Mechanisms and potential targets. Nutrients 5(4): 1218-1240.
-
Leon-Cabrera S, Solis-Lozano L, Suarez-Alvarez K, Gonzalez-Chavez A, Bejar YL, et al. (2013) Hyperleptinemia is associated with parameters of low- grade systemic inflammation and metabolic dysfunction in obese human beings. Front Integr Neurosci 7: 62.
-
Myers MG, Leibel RL, Seeley RJ, Schwartz MW (2010) Obesity and leptin resistance: Distinguishing cause from effect. Trends Endocrinol Metab 21(11): 643-651.
-
Ren J (2004) Leptin and hyperleptinemia-from friend to foe for cardiovascular function. Journal of Endocrinology 181(1): 1-10.
-
Suneja S, Ramakrishnan G, Tandon N, Chandra NC (2011) Modulation by insulin of the co-localized LDL receptor in normal and type-I diabetic subjects. Int J Clin Medicine 2(3): 231-245.
-
Suneja S, Christian Y, Chandra NC (2018) Milieu of diabetes in the 2nd decade of 21st century. J Diabetes Metab 9(9): 1-14.
-
Yadav NK, Arjuman A, Chandra NC (2014) Role of leptin on the expression of low density lipoprotein receptor. Indian J Med Res 140(4): 524-530.
-
Ramakrishnan G, Beriwal P, Sangam, Chandra NC (2019) Low density lipoproteinemia in obese and type- 2 diabetics from association of IR and LDLR. Diabetes Obes Int J 4(1): 1-6.
-
Haynes WG, Stanford C (2003) Periodontal Disease and Atherosclerosis From Dental to Arterial Plaque. Arterioscler Thromb Vasc Biol 23(8): 1309-1311.
-
Bartova J, Sommerova P, Lyuya-Mi P, Mysak J, Prochazkova J, et al. (2014) Periodontitis as a Risk Factor of Atherosclerosis. Journal of Immunology Research 2014: 636893.
-
Czerniuk MR, Surma S, Roman ́czyk M, Nowak JM, Wojtowicz A, et al. (2022) Unexpected Relationships: Periodontal Diseases: Atherosclerosis–Plaque Destabilization? From the Teeth to a Coronary Event. Biology 11(2): 272.
-
Cicmil S, Cicmil A, Pavlic V, Krunic ́J, Puhalo DS, et al. (2023) Periodontal Disease in Young Adults as a Risk Factor for Subclinical Atherosclerosis: A Clinical, Biochemical and Immunological Study. J Clin Med 12(6): 2197.
-
Peeran SW, Ranjith Singh AJ R, Alagamuthu G, Naveen Kumar P G (2013) Periodontal status and its risk factors among young adults of the Sebha city (Libya). Dental Research Journal 10(4): 533-538.
-
News (2005) BDJ 199(7): 411-419.
-
Lockhart PB, Bolger AF, Papapanou PN, Osinbowale O, Trevisan M, et al. (2012) Periodontal Disease and Atherosclerotic Vascular Disease: Does the Evidence Support an Independent Association? A Scientific Statement From the American Heart Association. Circulation 125(20): 2520-2544.
-
Zardawi F, Gul S, Abdulkareem A, Sha A, Yates J (2021) Association Between Periodontal Disease and Atherosclerotic Cardiovascular Diseases: Revisited. Front Cardiovasc Med 7: 625579.
-
Beukers NGFM, Van der Heijden GJMG, Van Wijk AJ, Loos BG (2017) Periodontitis is an independent risk indicator for atherosclerotic cardiovascular diseases among 60 174 participants in a large dental school in the Netherlands. J Epidemiol Community Health 71(1): 37-42.
-
Marroquin TY, Guauque-Olarte S (2023) Integrative analysis of gene and protein expression in atherosclerosis- related pathways modulated by periodontal pathogens. Systematic review. Japanese Dental Science Review 59: 8-22.
-
Loos BG, Dyke TEV (2020) The role of inflammation and genetics in periodontal disease. Periodontology 2000; 83(1): 26-39.
-
Aarabi G, Zeller T, Seedorf H, Reissmann DR, Heydecke G, et al. (2017) Genetic Susceptibility Contributing to Periodontal and Cardiovascular Disease. Journal of Dental Research 96(6): 610-617.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance