Knowledge, Attitudes and Practices of Healthcare Provider’s Regarding Physical Activity during Pregnancy
Objective: To assess knowledge, attitudes, and clinical practices of healthcare providers (HCP) regarding physical activity (PA) during pregnancy. Methodology: A convenient sample of 132 HCP, including General Practitioners, Obstetricians/Gynaecologists and Registered Nurses participated in this cross sectional, descriptive study. Data pertaining to their knowledge, beliefs, and practices regarding PA during pregnancy was collected using interviewer-administered 36 item questionnaire. Descriptive statistics and frequency tables were calculated and compared for the responses. Result: Overall 97% of participants believed that PA during pregnancy is beneficial but 58.3% agreed that advising patients regarding PA during pregnancy is not a major component of their antenatal care and 63.5% doesn’t include any individualized recommendation on exercise for pregnant women. Although HCPs beliefs and attitude responses were largely positive regarding exercise in pregnancy however there was misalignment between the published recommendations and clinical practice. Conclusion: HCPs can serve an important role in women's health behaviours through promotion of physical activity adherence during and after pregnancy by providing appropriate advice and counselling regarding PA during pregnancy. The current study found that HCPs lacked adequate knowledge and awareness of the optimal PA during pregnancy and were unable to provide proper counselling for the same despite of majority of them having positive belief and attitude towards PA during pregnancy. In order to effectively promote prenatal PA in clinical or community settings, more research is required to study the PA prescription and counselling practices of HCPs and knowledge of challenges impeding successful delivery of the aforementioned.
Introduction
Physical activity (PA) is useful for one’s health at all stages of life and pregnancy is no exception. The benefits of PA during pregnancy are well known with studies showing improved cardiovascular function, reduced risk of hypertension and diabetes, improved mental state, improved fitness, and less complicated delivery [1, 2, 3, 4]. In addition, it has been shown to reduce excessive gestational weight gain (GWG), which is an important predictor of several immediate and longterm adverse fetomaternal outcomes [4, 5, 6, 7]. Thus prescribing PA during the pregnancy will not only provide a protection against these modifiable risk factors but will also improve metabolic and cardiovascular health of the mother as well as the child and will contribute in mitigating short- term, long-term and intergenerational effects of obesity and excess GWG.
Although no nationwide data currently exists on the PA levels of Indian women during pregnancy, literature suggests that women are particularly vulnerable to inactivity, and misconceptions regarding PA during pregnancy are quite rampant [8]. Moreover, pregnant women’s knowledge and attitudes have been found to be a significant predictor of outcome measures in studies and meta-analyses aimed at improving perinatal outcomes through dietary and lifestyle changes [9, 10]. Despite the fact that the ACOG recommends pregnant women who are free of obstetrical complications to engage in PA and has become increasingly less restrictive [1, 11], there is growing evidence to suggest that neither pregnant women themselves engage in sufficient PA nor they are routinely prescribed PA during pregnancy by their HCPs. The reasons can be manyfold. Women may have unknown dangers and myths associated with PA during pregnancy [12]. HCP may lack knowledge or skills to undertake this type of counselling or consider PA to be of less significance in the setting of a typical antenatal care [13, 14, 15, 16]. A significant communication gap between patients and HCPs during prenatal visits is another potential barrier [12, 16].
HCPs play an imperative role in promoting women’s health behaviours [17, 18] and are in a good position to educate women about PA during pregnancy and resolving their concerns and myths. Brief counselling from a HCPs has been shown to be a successful and cost-effective way to increase exercise levels in the general population [17]. Evidence also suggests that women greatly relies on their HCPs for advices regarding nutrition and PA during pregnancy [8]. Moreover studies have reported that women receiving counselling from their HCPs regarding nutrition and PA during pregnancy tend to have lower risk of inappropriate GWG and macrosomia [19, 20]. Thus, HCPs serves as an integral source of information for pregnant women in promoting healthy lifestyle behaviours and have a significant impact in primary care disease prevention not just for the pregnant population but also the health of future generations. To better support HCPs in having positive PA counselling interactions with pregnant women, a thorough grasp of current practices and the factors influencing them is necessary but little is known on this subject. A recent review Okafor, et al. [21] on advice and counselling on PA by HCPs, highlighted significant factors limiting prenatal physical activity counselling by HCPs. The authors concluded that more research is required to study the prenatal PA prescription practices from HCPs and on the challenges impeding their successful delivery, in order to effectualy promote prenatal PA in both clinical or community settings and properly attain their stated benefits. Thus, future studies are required from greater number of healthcare professionals, from various specialities and experiences, belonging to different countries and regions and catering to pregnant women of different races and ethenicity in order to generate more robust data for future implementation. Therefore, we planned our study with the purpose to assess the practices, attitudes and knowledge of Indian HCPs towards PA during pregnancy.
Materials and Methods
Study Design
A cross-sectional, descriptive survey study, utilizing quantitative methods was conducted to determine HCP’s knowledge, beliefs, and practices regarding PA during pregnancy. Considering the nature of data to be gathered, it was decided that the descriptive survey was the optimum design for achieving the study’s goals. The design has been deemed reliable by numerous investigations on exercise counselling behaviour [15, 22]. Furthermore, the logistical and time constraints also influenced study’s design.
Study Instrument
A semi structured questionnaire was prepared by the study team based on the study objectives, using published guidelines [23] and adapted from previous studies [13, 14], according to the variables that were to be tested in this study, was used. The questionnaire was piloted for content validity and usability.
The Questionnaire had 3 Sections and consisted of likert-scale type questions, selected responses and open-ended questions. Section A dealt mainly, with the background information of the participants, including their gender, age, occupational specialty, practice location, level of care and duration of clinical experience. Section B was designed to asses HCP’s beliefs and attitude towards PA during pregnancy. A 4-point Likert scale was employed to assess how much the provider agree or disagree with the statement. In order to lessen response bias, questions were worded in both positive and negative tones. Since a neutral response has been shown to be a dubious scaling choice, it was not included in the Likert scale. Section C was designed to assess current provider practice regarding PA advice to patients. The providers were asked about what advice, counseling and restrictions are discussed with pregnant patients about exercise during antenatal period. The majority of questions used a Likert scale to rate how frequently a provider gives advice or restrictions about PA during pregnancy, with responses ranging from never, seldom, often, and always. The latter questions focused on the awareness of providers regarding recent ACOG guidelines for PA in pregnancy [1] and would they be interested in attending workshops or symposium on PA during pregnancy, if offered.
Recruitment and Data Collection
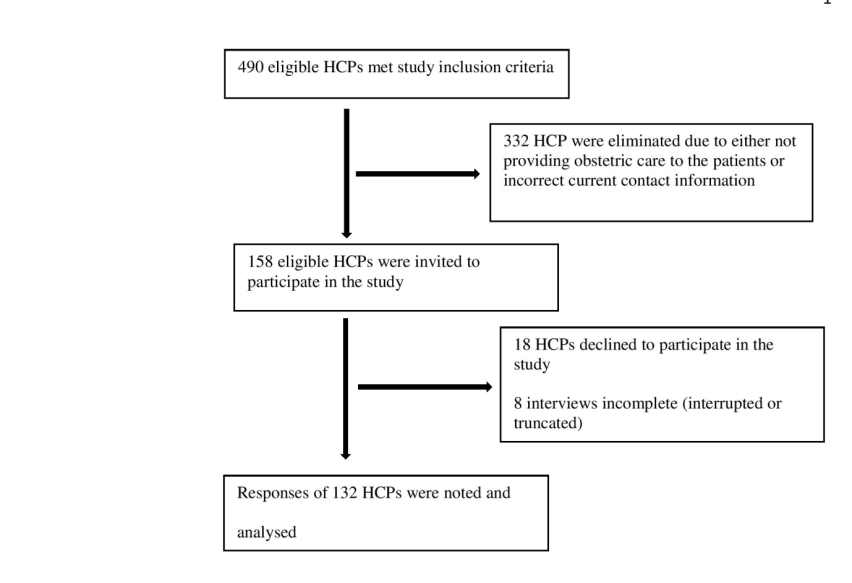
A HCP was eligible to participate in the study if he/she was a general practitioner (GP), obstetrician/ gynecologist (OBG) or a registered nurse providing obstetric care to pregnant women. Eligible HCPs who fulfilled the study inclusion criteria were identified through local hospital and clinical directories and initial search yielded 490 HCPs but a final sample of 132 HCP’s responses were noted and analysed. Figure 1 shows the recruitment flowchart of study participants. Prior to conducting the study, approval was taken from the Institutional Ethical Committee. All participants provided informed consent for participation in the study.
The study questionnaire was administered to all subjects by the same investigator (a final year medical student) to avoid inter-observer variations. Data was cross-checked by other investigators. Each participant was surveyed using a pen and paper instrument and all the questions were mandatory which ensured the completeness of the survey.
To maintain confidentiality no personal identifying information was collected. The data from the questionnaire was checked manually for completeness, coded, entered in MS excel sheet and analysed. Descriptive statistics and frequency tables were calculated.
Result
Participant Characteristics
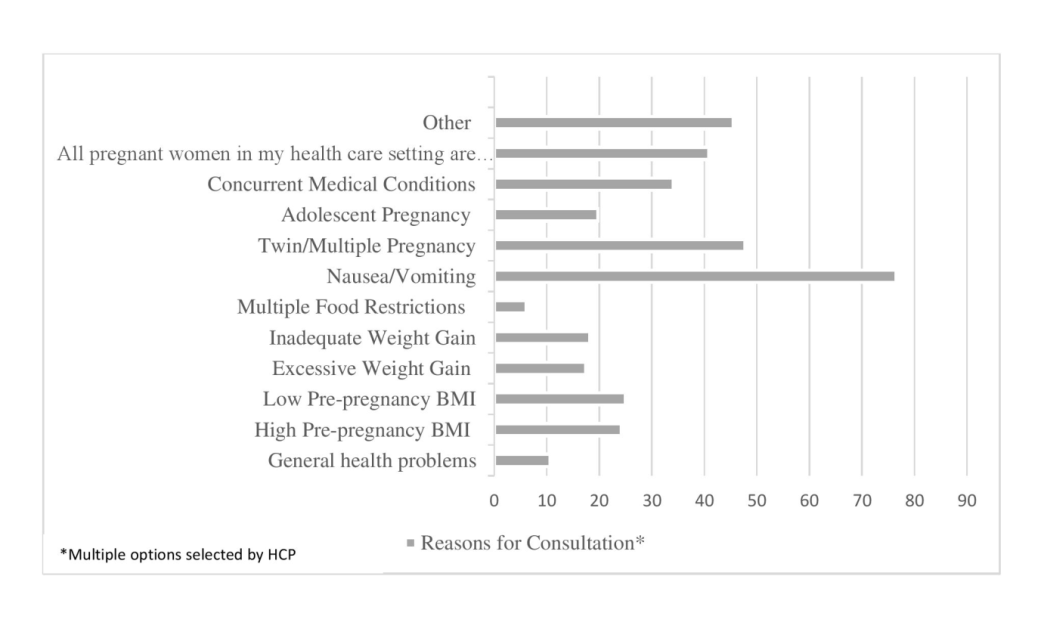
Background participant characteristics are reported in Table 1. The majority of HCPs were women (96.2%), OBG specialists (68.2%), and between the ages of 20 to 39 years (68.2%). Common reasons cited by HCPs for consultation and referral of pregnant women included common pregnancy ailments, complications or medical comorbidities and no HCPs has mentioned counselling on physical activity as one of the reason for consultation or referral of pregnant women (Figure 2).
| Variable | n | % |
|---|---|---|
| Provider Discipline | ||
| Obstetrician/ Gynaecologist | 90 | 68 |
| General Practitioner | 25 | 19 |
| Registered Nurse | 17 | 13 |
| Gender | ||
| Male | 5 | 3.8 |
| Female | 127 | 96 |
| Age (years) | ||
| <20 | 14 | 11 |
| 20-29 | 59 | 45 |
| 30-39 | 31 | 24 |
| 40-49 | 25 | 19 |
| >50 | 3 | 2.3 |
| Location of Practice | ||
| Urban | 93 | 71 |
| Semiurban | 34 | 26 |
| Rural | 5 | 3.8 |
| Practice Setting | ||
| Primary care | 35 | 27 |
| Secondary care | 38 | 29 |
| Tertiary care | 59 | 45 |
| Duration of Practice (years) | ||
| 1-5 | 41 | 31 |
| 6-10 | 31 | 24 |
| 11-15 | 32 | 24 |
| 16-20 | 17 | 13 |
| >20 | 11 | 8.3 |
Table 1: Background Characteristics of participating Indian Healthcare Providers (n=132).
Attitude of HCPs Regarding PA during Pregnancy
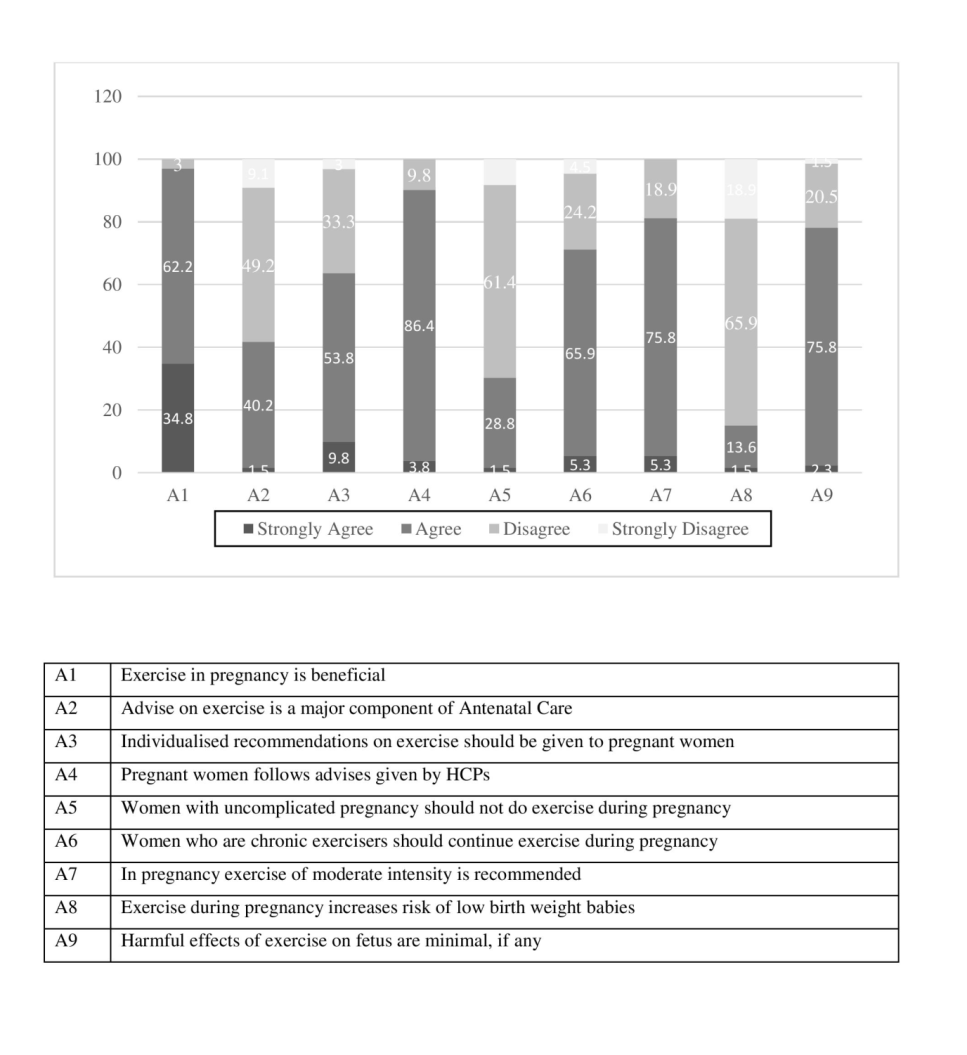
Although 97% of participants agreed that exercise during pregnancy is advantageous but 58.3% believe that advising patients on exercise during pregnancy is not a major component of their antenatal care and 63.5% doesn’t include any individualized recommendation on exercise for pregnant women. A breakdown of key question responses by providers is reported in Figure 3.
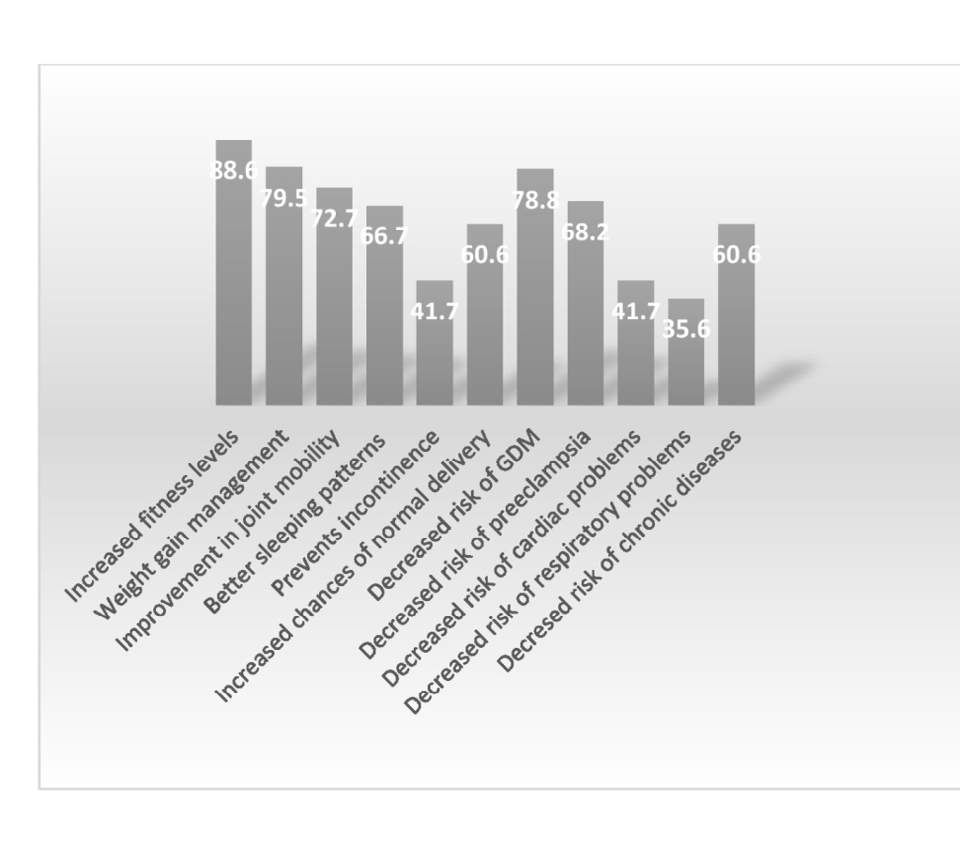
Regarding benefits of PA during pregnancy as observed by HCPs, majority believed that exercise improved general health of pregnant women like increased fitness level (88.6%), weight gain management (79.5%), better sleeping patterns (66.7%) and improved joint mobility (72.7%) (Figure 4). Besides they also believe that PA during pregnancy also increases chances of normal delivery and decreases risk of some maternal complications like Gestational Diabetes Mellitus(GDM) (78.8%) and preeclampsia (68.2%) (Figure 4).
Practices of HCPs Regarding PA during Pregnancy
When enquired about their practices regarding exercise prescription during pregnancy, 70%(n=93) of the HCPs reported that they give some or other form of advice about exercise in pregnancy to their patients. HCPs beliefs and attitude responses were largely positive regarding exercise in pregnancy however there appears to be a misalignment between the published recommendations and clinical practice. Responses regarding practice of exercise prescription of HCPs who advice PA during pregnancy are shown in Table 2. 60.2 % of HCPs advise their patients low intensity of exercise in their clinical practice, 39.8% advice exercise of moderate intensity and none of them advice vigrous intensity of exercise to the patients. The study also revealed that more than 90 % practitioners never provide informational pamphlets or individualized exercise program to their patients. Furthermore, about 70% never obtain any exercise history on their pregnant patients. The possible reasons for these disparities as cited by various respondents included high patient load, lack of time, priority level as compared to other grave issues during pregnancy and deficiency of detailed knowledge of practice guidelines. When assessing antenatal referral practices approximately half of the respondents stated that they don’t refer patients to other specialists for exercise. Among those who refer to other specialists for exercise, 48.5% refer to a physiotherapist, 1.5% to personal trainers and none to the biokineticists (Clinical Exercise Specialist).
| Variable | n | % |
|---|---|---|
| Stage of Pregnancy at which Counselling for Exercise is Done | ||
| 1st Trimester | 28 | 30 |
| 2nd Trimester | 47 | 51 |
| 3rd Trimester | 18 | 19 |
| Duration of Counselling Session on Exercise Prescription | ||
| 5-10 mins | 58 | 62 |
| 11-20 mins | 27 | 29 |
| 21-30 mins | 7 | 7.5 |
| >30 mins | 1 | 1.1 |
| Intensity Of Exercise Recommended | ||
| Low | 56 | 60 |
| Moderate | 37 | 40 |
| Vigorous | 0 | 0 |
| Informational Pamphlets on Exercise given to Patients | ||
| Never | 86 | 92 |
| Seldom | 7 | 7.6 |
| Often | 0 | 0 |
| Always | 0 | 0 |
| Exercise History taken in Pregnancy | ||
| Never | 66 | 71 |
| Seldom | 17 | 18 |
| Often | 9 | 9.7 |
| Always | 1 | 1.1 |
| Individualized Exercise Program Provided | ||
| Never | 84 | 90 |
| Seldom | 9 | 9.7 |
| Often | 0 | 0 |
| Always | 0 | 0 |
Table 2: Exercise Counselling Practices routinely undertaken by Healthcare Providers (n=93).
Knowledge of HCPs Regarding PA during Pregnancy
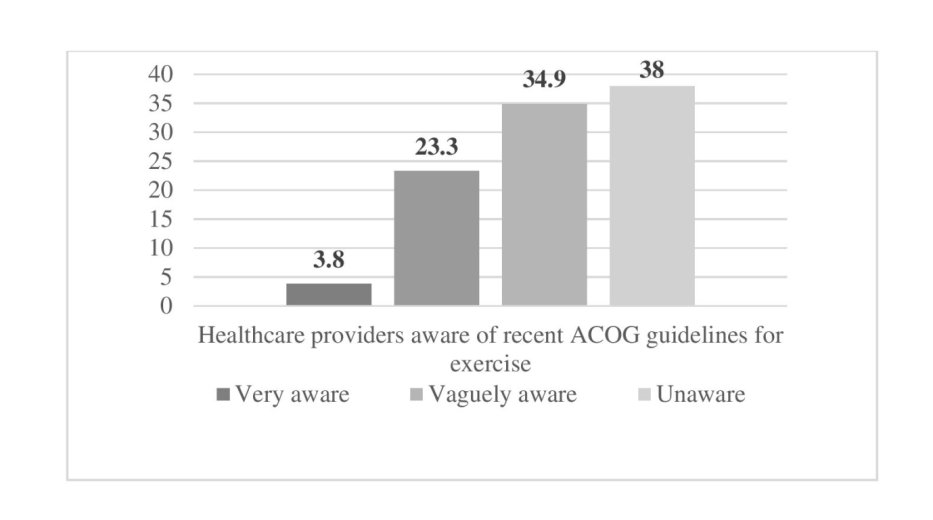
Although majority of HCPs in our study had positive beliefs and attitudes towards PA during pregnancy, a large number (72.9%) of them are either unaware or vaguely aware of the recent ACOG Guidelines regarding Exercise during pregnancy (Figure 5). However, an encouraging number of HCPs (84.8%) reported they want to update their knowledge in this field and would like to attend symposium/ workshop on exercise and pregnancy.
Discussion
PA during pregnancy is a public health concern and there is ample evidence to suggest that regular PA during pregnancy, promotes both short and long term health benefits. The responsibility of HCPs in disseminating this information however, remains unclear owing to paucity of literature on HCPs’ attitudes, beliefs, and current practices regarding antenatal physical activity. The current cross-sectional study addressed this gap by providing a comprehensive assessment of HCPs knowledge, attitudes and practices regarding PA during pregnancy. We found that although majority of HCPs had positive attitude regarding PA during pregnancy, but still large number of them agreed that giving advice regarding exercise during pregnancy is not a major component of their prenatal care. They don’t spend sufficient time during counselling sessions and often provide misinformation. Moreover, most of the participants, regardless of their age, speciality and duration of practice, lacked knowledge and awareness of current exercise recommendations. These findings emphasize the need for a paradigm shift regarding how pregnancy-related PA is perceived and improvement in the accuracy of the advices offered. We also found that >60% of HCPs spent maximum 5–10 minutes during counselling sessions on exercise prescription, supporting the results found by Lewis, et al. [24] and Bauer, et al. [13]. Among those that prescribe PA, large proportion of HCPs advise low intensity PA to the pregnant women. This is coherent with studies by Evenson, et al. [25] and Watson, et al. [14], where most HCPs prescribed mild PA during pregnancy and is in line with the belief of majority of HCPs that pregnancy is a high risk state and avoidance of minutest risk to the foetus should be preferred over the maternal benefits of PA [24]. We believe these to be significant findings as inadequate time given to the patients, as well as inaccurate information provided by HCPs, can have a negative impact on a woman’s PA behaviour during pregnancy.
In addition, our study reported that over half of the participants had fairly positive views regarding some benefits of PA in pregnancy like GWG management, better sleeping patterns, improved joint mobility, increased chances of normal delivery and decreased risk of some maternal complications like GDM and preeclampsia, which coincided with previously reported views by many studies [2, 3, 4]. However, we found that many HCPs were ignorant about the benefits of PA in preventing and treating incontinence and in decreasing cardiac and respiratory problems. This showed that though providers were fairly knowledgeable of most of the benefits of PA during pregnancy but still there is need to establish and reinforce awareness on many other aspects.
There appears to be a wide gap between recommendations and guidelines related to PA during pregnancy and their clinical understanding and prescription. Consistent with prior research [13, 25, 26] emphasising the lack of knowledge of ACOG guidelines among HCPs, this study also found that only a minor proportion of the study’s participants were aware of the ACOG recommendations. And probably this lack of knowledge could explicate why many HCPs in this study didn’t routinely provided proper and recommended counselling for PA during pregnancy. But what is encouraging that majority of study participants indicated a keenness and enthusiasm towards attending workshops and symposiums on the subject. This interest in continuing education of HCPs, has been confirmed by prior research [13, 25] and has the potential to significantly increase the frequency and effectiveness of physician guidance, which can be crucial in raising activity levels at the primary healthcare level [24]. Thus improved communication of recent research and guidelines about PA during pregnancy, to the HCPs appears to be highly necessary and trainings for the same, in the form of symposium and workshops is necessary.
Although related work have been done in other countries in the past, but very few have assessed Indian HCPs beliefs, attitudes and knowledge towards PA during pregnancy and to the best of our knowledge this study is the one of its kind assessing North Indian HCPs exercise prescription practices. Few countries have their own guidelines for PA during pregnancy and even provide guidance to their HCPs in order to support them in providing physical activity and nutrition counselling to pregnant women but most of the developing countries doesn’t have any national guidelines on PA during pregnancy. Owing to the importance of PA during pregnancy on one hand and significant sociocultural differences from developed countries on the other hand, there is a necessity to formulation and adoption of national guidelines by different countries. Studies like ours will help administrators and policy makers in better understanding the problem and to determine how these implementations can be applied. Also our study recruited diverse set of the HCPs rather than just focusing on OBG Specialists which is conducive to the development of comprehensive initiatives. Moreover, we used interview method, which increases participation compared with written surveys. Also a single researcher executed all the interviews, excluding inter observer variation. The study however had many limitations. A major limitation is the small sample size and convenience sample. Our convenient sample of HCPs, due to its non- representative nature, might hinder generalisation of the results and owing to the nonrandom sample, there may be possible response bias also. In addition, selectivity bias such that only those HCPs who were interested in the topic of antenatal physical activity agreed to participate in the study, may also be a possible limitation. Finally, a qualitative study design could have offered better information about hurdles and facilitators of counselling practices.
Conclusion
Prenatal PA prescription is critical in promoting adherence to PA during and after pregnancy and promoting public health. This necessitates awareness of interventions for dissemination of knowledge regarding PA during pregnancy and adequate knowledge of PA prescriptions practices among prenatal HCPs. The current study found that HCPs lacked adequate knowledge and awareness of the optimal PA needed during pregnancy and were unable to provide proper counselling for the same despite of majority of them having positive belief and attitude towards PA during pregnancy. Our findings highlight the importance of HCPs knowledge regarding recent recommendations on PA during pregnancy and emphasize the need for additional continuing education opportunities for the same, in order to improve the likelihood and overall quality of antenatal PA counselling among HCPs.
We believe that results of our study will help healthcare professionals and administrators to shape future approaches in promoting antenatal physical activity counselling in order to improve both mothers’ and newborns’ health outcomes. Furthermore future large scale studies, from regional or national cohorts are required to investigate provider education or training interventions in order to assess their issues and challenges and patient compliance to get a better understanding and dissemination of the subject.
Ethical Approval
The study has been approved by the Institutional Ethics Committee [Reference No. IECJNMC/653].
Conflict of Interest
There is no conflict of interest regarding this study.
References
-
ACOG (2020) Physical Activity and Exercise During Pregnancy and the Postpartum Period. Acog.org.
-
Meander L, Lindqvist M, Mogren I, Sandlund J, West CE, et al. (2021) Physical activity and sedentary time during pregnancy and associations with maternal and fetal health outcomes: an epidemiological study. BMC Pregnancy and Childbirth 21: 166.
-
Davenport MH, Ruchat SM, Poitras VJ, Jaramillo Garcia A, Gray CE, et al. (2018) Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: a systematic review and meta- analysis. British Journal of Sports Medicine 52(21): 1367-1375.
-
Prather H, Spitznagle T, Hunt D (2012) Benefits of exercise during pregnancy. PM&R 4(11): 845-50.
-
Thorsdottir I, Torfadottir JE, Birgisdottir BE, Geirsson RT (2002) Weight gain in women of normal weight before pregnancy: complications in pregnancy or delivery and birth outcome. Obstet Gynecol 99(5): 799-806.
-
Houghton LC, Ester WA, Lumey LH, Michels KB, Wei Y, et al. (2016) Maternal weight gain in excess of pregnancy guidelines is related to daughters being overweight 40 years later. Am J Obstet Gynecol 215(2): 246.e1-246.e8.
-
Gilmore LA, Klempel Donchenko M, Redman LM (15) Pregnancy as a window to future health: excessive gestational weight gain and obesity. Semin Perinatol 2039(4): 296-303.
-
Rafat D, Sulaiman M, Nawab T (2022) Knowledge and Perception of Pregnant Women regarding Excess Maternal Weight, Gestational Weight Gain and their Impact on Foetomaternal Outcomes: A Cross-sectional Study. Journal of Clinical and Diagnostic Research 16(2): QC04-QC08.
-
Desai D, Kandasamy S, Limbachia J, Zulyniak MA, Ritvo P, et al. (2021) Studies to Improve Perinatal Health through Diet and Lifestyle among South Asian Women Living in Canada: A Brief History and Future Research Directions. Nutrients 13(9): 2932.
-
Teede HJ, Bailey C, Moran LJ, Khomami MB, Enticott J, et al. (2022) Association of Antenatal Diet and Physical Activity–Based Interventions With Gestational Weight Gain and Pregnancy Outcomes: A Systematic Review and Meta-analysis. JAMA Intern Med 182(2): 106-114.
-
Artal R, O’Toole M (2003) Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br J Sports Med 37(1): 6-12.
-
Delgado A, Stark LM, Macri CJ, Power ML, Schulkin J (2018) Provider and Patient Knowledge and Views of Office Practices on Weight Gain and Exercise during Pregnancy. Am J Perinatol 35(2): 201-208.
-
Bauer PW, Broman CL, Pivarnik JM (2010) Exercise and pregnancy knowledge among healthcare providers. J Womens Health 19(2): 335-341.
-
Watson ED, Oddie B, Constantinou D (2015) Exercise during pregnancy: knowledge and beliefs of medical practitioners in South Africa: a survey study. BMC Pregnancy Childbirth 15(245).
-
Olutende OM, Bukhala PW, Wesonga B (2018) Exercise Prescription: Practices of Healthcare Professionals in Hospital Setting, Kenya. Journal of Physical Activity Research 3(1): 47-54.
-
Ferrari RM, Siega Riz AM, Evenson KR, Melvin CL, Moos M, et al. (2010) Provider advice about weight loss and physical activity in the postpartum period. J Womens Health 19(3): 397-406.
-
Garrett S, Elley CR, Rose SB, Dea DO, Lawton BA, et al. (2011) Are physical activity interventions in primary care and the community cost-effective? A systematic review of the evidence. Br J Gen Pract 61(584): 125-133.
-
Burns KE, Duffett M, Kho ME, Meade MO, Adhikari NK, et al. (2008) A guide for the design and conduct of self- administered surveys of clinicians. Can Med Assoc J 179(3): 245-252.
-
Cole KOW, Gudzune KA, Bleich SN, Bennett WL, Cheskin LJ, et al. (2017) Influence of the 5A’s counseling strategy on weight gain during pregnancy: an observational study. J Womens Health 26: 1123-1130.
-
Peccei A, Blake Lamb T, Rahilly D, Hatoum I, Bryant A, et al. (2017) Intensive prenatal nutrition counseling in a community health setting: a randomized controlled trial. Obstet Gynecol 130(2): 423-432.
-
Okafor UB, Goon DT (2021) Physical Activity Advice and Counselling by Healthcare Providers: A Scoping Review. Healthcare 9(5): 609.
-
Galaviz KI, Jauregui E, Fabrigar L, Latimer Cheung A, Lopez y, et al. (2015) Physical activity prescription among Mexican physicians: a structural equation analysis of the theory of planned behavior. International Journal of Clinical Practice 69(3): 375-383.
-
Burns KE, Duffett M, Kho ME, Meade MO, Adhikari NK, et al. (2008) A guide for the design and conduct of self- administered surveys of clinicians. Can Med Assoc J 179(3): 245-252.
-
Lewis BS, Lynch WD (1993) The effect of physician advice on exercise behavior. Prev Med 22(1): 110-121.
-
Evenson KR, Pompeii LA (2010) Obstetrician Practice Patterns and Recommendations for Physical Activity During Pregnancy. Journal of Women’s Health 19(9): 1733-1740.
-
Leiferman J, Gutilla M, Paulson J, Pivarnik J (2012) Antenatal physical activity counseling among healthcare providers. Open Journal of Obstetrics and Gynecology 2(4): 346-355.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance