Antidiabetic Therapy in Patients Related to CKD (Chronic Kidney Disease)
Patients with type 2 diabetes mellitus (T2DM) are more likely to have chronic kidney disease (CKD) in stages 3-5 (glomerular filtration rate [GFR] 60 mL/min) by roughly 25–30%. Despite the limits of most oral anti-diabetic medications in people with CKD, incretin-based treatments are being utilized more frequently to treat type 2 diabetes. This study examines the impact of CKD on the pharmacokinetics of glucagon-like peptide-1 (GLP-1) receptor agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors, as well as the efficacy/safety profile of these medications when used in patients with T2DM and CKD. Sitagliptin, Vildagliptin, Saxagliptin, and Alogliptin are the most common DPP-4 inhibitors that are primarily excreted by the kidneys. This led to recommendations for appropriate dose reductions based on the severity of CKD after pharmacokinetic studies revealed that total exposure to the medication is increased in proportion to the fall in GFR. Clinical investigations found that patients with CKD had a high effectiveness and safety profile under these circumstances. Lintagliptin, on the other hand, is primarily excreted through the hepatobiliary system. No dose adjustment of lintagliptin is necessary in the setting of CKD because a pharmacokinetic investigation revealed that lower GFR had a negligible impact on total exposure. Patients with CKD have less experience using GLP-1 receptor agonists. Exenatide should not be administered to patients with severe CKD because it is excreted through renal processes. Due to the limited experience with CKD patients, ligarglutide should be administered with caution even if the kidneys do not remove it from the body. For lixisenatide, exenatide long-acting release (LAR), and other once-weekly GLP-1 receptor agonists now under development, only scant pharmacokinetic data are also available. GLP-1 receptor agonists have been implicated in several case reports of acute renal failure, which was most likely brought on by dehydration brought on by gastrointestinal side effects. Nevertheless, improving GLP-1 may also have advantageous renal effects that could help lower the incidence of diabetic nephropathy. In conclusion, the physician has new chances due to the DPP-4 inhibitors' broad and encouraging experience in CKD patients, whereas the limited experience with GLP-1 receptor agonists in this population calls for greater caution.
Introduction
Diabetes Mellitus
A heterogeneous, complicated metabolic condition called diabetes is characterized by increased blood glucose levels brought on by either resistance to the action of insulin, inadequate insulin secretion, or both [1]. Type 1 diabetes, Type 2 diabetes, and gestational diabetes are the three most widely used classifications.
The symptoms of type 2 diabetes (T2DM) include insulin resistance and a relative lack of insulin production [2]. Even if the absolute plasma insulin concentration (during fasting and after meals) is typically higher, it is typically insufficient to sustain healthy glucose homeostasis” relative”: to the degree of insulin resistance. In the majority of T2DM patients, insulin secretion capability gradually declines over time [3]. Diabetes mellitus is a group of physiological dysfunctions characterized by hyper-glycaemia resulting directly from insulin resistance, inadequate insulin secretion, or excessive glucagon secretion [4]. Type 1 Diabetes (T1D): Typically diagnosed in childhood or young adulthood, T1D results from an autoimmune reaction that destroys the insulin-producing beta cells in the pancreas. People with T1D require lifelong insulin therapy to survive [5].
- Is destruction of pancreatic beta cells
- It is auto immune disorder Type 2 Diabetes (T2D): The most common form, T2D is often linked to insulin resistance and lifestyle factors. It can develop at any age but is more common in adults. It may be managed through lifestyle changes, medication, or insulin.
- It is progressively impaired glucose regulation due to a combination of dysfunctional pancreatic beta cells and insulin resistance [6].
Chronic Kidney Disease
Chronic Kidney Disease (CKD), also known as chronic renal disease, is a long-term condition characterized by the gradual loss of kidney function over time [7].
CKD is typically categorized into stages, with each stage representing different levels of kidney damage and reduced function. The most common system used to classify CKD is the Kidney Disease Improving Global Outcomes (KDIGO) staging, which includes stages 1 to 5: Stage 1: Kidney damage with normal or increased glomerular filtration rate (GFR). GFR is a measure of kidney function. Stage 2: Kidney damage with mild reduction in GFR. Stage 3: Mild to moderate reduction in GFR. Stage 4: Severe reduction in GFR. Stage 5: End-stage kidney disease (ESKD) with very low GFR. At this stage, patients typically require dialysis or a kidney transplant to survive.
The most common causes of CKD include diabetes, high blood pressure (hypertension), glomerulonephritis (inflammation of the kidney’s filtering units), and polycystic kidney disease. Other factors that can contribute to CKD include autoimmune diseases, recurrent kidney infections, urinary tract obstructions, and certain medications [8].
Diabetic Nephropathy
Diabetic nephropathy is typically slow and progressive , also known as diabetic kidney disease, is a progressive kidney condition that develops as a complication of diabetes, primarily diabetes mellitus. It is a major cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) worldwide. Diabetic nephropathy is characterized by kidney damage and deterioration in kidney function as a result of prolonged high blood sugar levels associated with diabetes [8]. Association with Diabetes: Diabetic nephropathy is a specific type of kidney disease that occurs in individuals who have diabetes, particularly when the diabetes is poorly controlled. Both type 1 and type 2 diabetes patients are susceptible to diabetic nephropathy, although it is more commonly associated with type 1 diabetes [9]. Progressive Kidney Damage: Over time, persistently high blood sugar levels in diabetes can cause damage to the small blood vessels (glomeruli) in the kidneys. This damage impairs the kidneys’ ability to filter waste and excess fluids from the blood effectively. As a result, waste products accumulate in the bloodstream, and protein may leak into the urine [10]. Stages of Diabetic Nephropathy: Diabetic nephropathy typically progresses through stages, from mild kidney damage to more severe impairment: Microalbuminuria: In the initial stage, small amounts of the protein albumin begin to appear in the urine, which is an early sign of kidney damage. Proteinuria: As the condition advances, larger amounts of protein leak into the urine. Decline in Kidney Function: Over time, kidney function continues to decline, potentially leading to chronic kidney disease (CKD) or end-stage kidney disease (ESKD) [11].
The relationship between diabetes and CKD is significant and multifaceted. Diabetes is one of the leading causes of chronic kidney disease. Over time, the consistently high levels of glucose in the blood associated with diabetes can damage the delicate blood vessels and nephrons (the filtering units) in the kidneys. This damage impairs the kidneys’ ability to function properly and ultimately leads to CKD. Therefore, individuals with diabetes are at a substantially higher risk of developing CKD [12].
Anti-Diabetic Medication in CKD
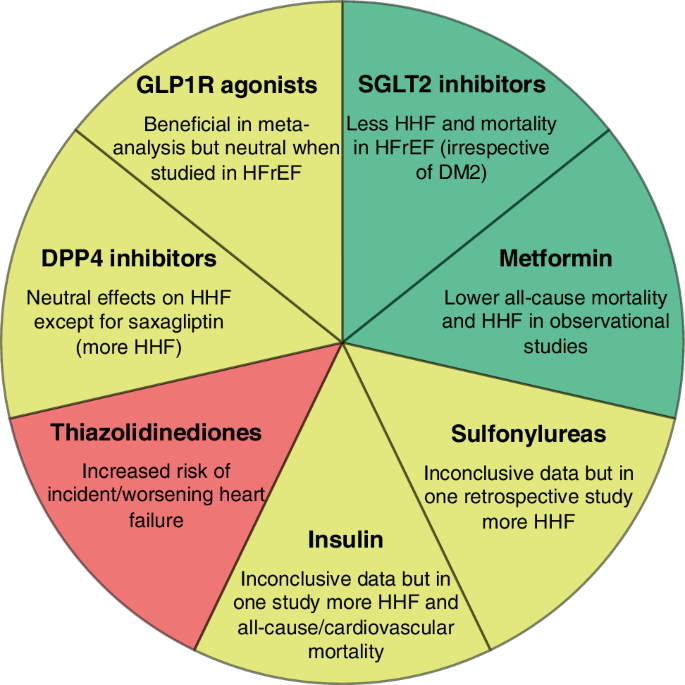
Dialysis is being used by more and more people with primary diabetic nephropathy. In addition to having a worse prognosis than patients with primary glomerular nephropathy, diabetics with chronic kidney disease (CKD) who are receiving dialysis also have a higher risk of cardiovascular morbidity and a more convoluted course of the disease [13]. According to recent clinical evidence, rigorous glycaemia management lowers the risk of cardiovascular disease, which is the leading cause of death in diabetes patients (Figure 1) [14].
Due to the risk of persistent hypoglycaemia, conventional oral hypoglycaemic drugs such sulfonylurea (SU) are unsuitable, and metformin is also not recommended. In order to establish effective glycaemic control in diabetic patients with moderate to advanced CKD, particularly in those receiving dialysis therapy, insulin injection therapy continues to be the cornerstone of treatment. However, several medications have been tried on CKD patients and were proven to be safe and effective, even for those receiving dialysis. Consequently, several medications could be beneficial therapeutic choices for the control of diabetes [15].
Classification of Antidiabetic Agents
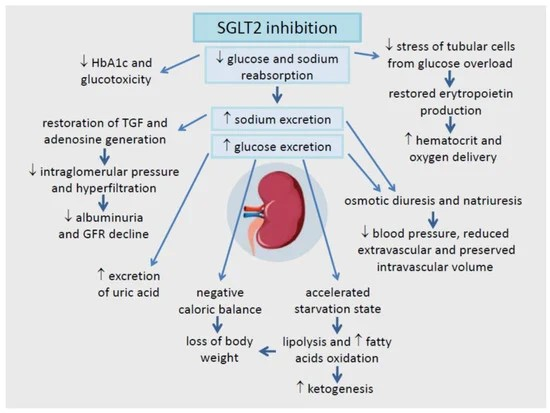
Several pharmacologic treatments, besides insulin preparations, are available for the therapy of type 2 diabetes, as illustrated in below. All of these medications lower blood sugar levels, but there is growing knowledge that they may alter the course of diabetes naturally in various ways. Sulphonylureas (SUs) and Meglitinides are two types of insulin secretagogues. Insulin sensitivity is increased by Thiazolidinedione’s whereas glucose absorption is modified by alpha-glucosidase inhibitors [16]. Dipeptidyl peptidase-4 (DPP-4) inhibitors and incretin mimics are two treatments related to incretin. DPP-4 inhibitors are oral diabetes medications, whereas incretin mimics are administered subcutaneously. Metformin: Metformin is generally considered safe in CKD, but its use may be restricted in severe CKD (Stage 4 or 5) due to the risk of lactic acidosis. Dose adjustments are necessary, and it is typically avoided if the glomerular filtration rate (GFR) falls below 30 mL/min [17]. Sulfonylureas: Sulfonylureas are associated with an increased risk of hypoglycemia and may need dose adjustments in CKD. They are usually avoided in severe CKD [18]. Meglitinides (Repaglinide, Nateglinide): These drugs are primarily eliminated by the liver and are considered safe for use in CKD. Dose adjustments may be necessary if there is concomitant liver impairment. Dipeptidyl Peptidase-4 Inhibitors (DPP-4 Inhibitors): DPP-4 inhibitors are considered safe in CKD and do not require dose adjustments. Sodium-Glucose Co-Transporter-2 Inhibitors (SGLT-2 Inhibitors): SGLT-2 inhibitors can be beneficial in CKD, as they have been shown to reduce proteinuria and slow down the progression of kidney disease. However, they should be initiated and monitored carefully, especially with regard to volume depletion and the risk of diabetic ketoacidosis [19]. Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 Receptor Agonists): GLP-1 receptor agonists are generally safe in CKD, and some (e.g., Liraglutide) have shown cardiovascular and renal benefits. Thiazolidinedione’s (TZDs) (e.g., Pioglitazone, Rosiglitazone): Thiazolidinedione’s are generally safe in CKD but should be used with caution in patients with fluid retention and heart failure. Use in CKD: TZDs can be used in CKD patients but should be used cautiously, as they can cause fluid retention, which may exacerbate edema and hypertension in individuals with compromised kidney function [20]. Alpha-Glucosidase Inhibitors (e.g., Acarbose, Miglitol):
Use in CKD: Alpha-glucosidase inhibitors can be used in CKD patients. However, their effectiveness may be reduced in advanced CKD stages [21]. Bile Acid Sequestrants (e.g., Colesevelam): Use in CKD: Bile acid sequestrants can be used in CKD patients. They have minimal systemic absorption and are not excreted by the kidneys [22]. Pharmacokinetics in Chronic Kidney Disease: Characteristics: Numerous medications bind to albumin and other serum proteins. However, because renal insufficiency often results in a decrease in albumin content in the plasma, unbound medication concentrations rise in these patients. The rate of elimination for substances with low hepatic extraction rates and high protein binding rates is influenced by unbound plasma levels and intrinsic liver clearance [23]. For medications like phenytoin and warfarin, overall clearance will rise and half-life will typically shorten assuming no change in the intrinsic capacity of the liver. Additionally, the liver and gastrointestinal tract’s metabolic enzymes are variably affected by kidney illness, alterations that are probably brought on by uremic toxins [24].
Reduced gastrointestinal absorption, which has been shown in individuals with severe renal impairment for cyclosporine, ibuprofen, and levocabastine, may contribute to a shift in systemic bioavailability [25]. The expression of hepatic P-GP and multidrug resistance-associated protein-2 was found to be increased and hepatic organic anion- transporting polypeptide, (OATP) expression was found to be decreased in uremia when intestinal P-glycoprotein (P-GP) and multidrug resistance-associated protein-2 expression and function were decreased. Numerous publications demonstrating changed pharmacokinetics of recognized OATP, P-GP, and/or cytochrome P450 (CYP) substrates in patients with kidney illness imply that uremia impacts these elimination pathways and highlight the clinical significance of altered nonrenal clearance. Because uremia variably impacts these pathways in the liver and gastrointestinal tract and results in a lower protein level, vigilance is necessary [26].
Insulin
Renal gluconeogenesis is impaired in patients with progressive kidney disease because of reduced kidney mass, which increases the risk of hypoglycemia. Insulin clearance is further compromised in conjunction with some diabetic treatments. A prolonged insulin half-life and a decrease in insulin needs as GFR drops are linked to lower renal function. The kidney is responsible for approximately 30 to 80% of insulin elimination [27].
Patients with CKD can take any available insulin formulation, and there is no recommended dosage reduction for insulin users. For each patient, a customized insulin type, dosage, and administration strategy is needed to reach target glycemic levels while minimizing hypoglycemia.
Aspart, lispro, and glulisine are the fastest-acting insulin analogues that can be used for prandial insulin demands or for fast treatment of high blood sugar [28]. Their rapid absorption closely mimics the process of physiologic insulin secretion. Their duration is 5 hours on average, with a 5 to 15-minute start and 30 to 90-minute peak. Compared to the other two rapid-acting insulins, glycine appears to have a slightly longer duration of action, according to certain studies [29]. These insulins can be administered up to 15 minutes before a meal. They are utilized in continuous subcutaneous insulin infusions, sometimes referred to as insulin pumps, and in “basal-bolus therapy,” also known as multiple daily injections (MDI) [30].
Giving rapid-acting insulin after a meal may be useful in synchronising the insulin peak with the postprandial blood glucose peak, as patients with Stage 4–5 CKD and dialysis patients frequently experience some delayed stomach emptying [31]. Postprandial rapid-acting insulin dosage can be something to consider for people with nausea who might not know how much they will consume. Similarly, postprandial dosage may be beneficial for patients receiving peritoneal dialysis because these patients typically consume less food than they may anticipate and get a high quantity of calories from their dialysis fluid [32].
Regular crystalline insulin is the kind of short-acting insulin that is readily available. It acts for up to 5-8 hours, peaking at 2-4 hours after administration. Ideally, regular insulin should be administered half an hour before a meal [33].
Isophane, often known as NPH, is the available intermediate-acting insulin. It acts for 2-4 hours, peaks in concentration between 4 and 10 hours, and lasts for up to 18 hours. It is dosed twice a day to obtain sufficient basal coverage. Its use can be limited by its highly variable absorption. It costs about the same as regular insulin [34].
Both glargine and detemir are long-acting insulin analogues. Glargine is typically dosed once day and has a low peak and duration of 20–24 hours. Its commencement of effect occurs at 2-4 hours. The absence of a distinct peak is one of glargine’s distinctive characteristics. Detemir acts for 18 to 22 hours, peaking for a brief period at 7-8 hours [35]. It starts working at 1-3 hours. In patients with type 1 diabetes, a twice-daily dose of detemir provides appropriate basal coverage; in patients with type 2 Different premixed insulin preparations are available, each containing a predetermined proportion of both rapid- or short-acting and intermediate-acting insulin. They have two distinct peaks because they contain two different insulins [36]. “70/30,” which is composed of 70% NPH and 30% normal insulin, is one example.
With twice-daily dosage, these preparations are more convenient for the patient; however, there is less flexibility and greater restriction on insulin titration. The patient needs to take it at set intervals and eat consistently. When a patient is receiving 12-hour cycled tube feedings, 70/30 insulin may be beneficial. Diabetes, a once-daily dose may be sufficient [37].
U-100, or 100 units of insulin per milliliter, is the standard for all insulin. Insulin U-500 is the sole exception; it comes exclusively in normal form and contains 500 units of insulin per milliliter. The pharmacokinetics of ordinary insulin are different due to the alteration of its characteristics caused by the high concentration of U-500 insulin. It acts similarly, starting to take effect in around 30 minutes, but it peaks in 5-8 hours and lasts for 14–15 hours [38]. It is normally administered two or three times a day, without the need for basal insulin, and it can be taken up to thirty minutes before meals. It can be injected subcutaneously or administered via a pump, and it is typically utilized in patients who exhibit significant insulin resistance [39].
Pharmacology of Insulin
The pharmacokinetics of different insulin formulations in individuals with different degrees of renal impairment have not been thoroughly investigated, and there are no hard and fast rules specifying the proper insulin dosage modifications based on GFR [40].
In patients with severe renal failure, some writers have advised against using long-acting insulin preparations; nevertheless, other authors have suggested using them. When comparing the pharmacokinetics of insulin lispro, a more recent insulin, and regular insulin in patients with type 1 diabetes mellitus and diabetic nephropathy, found that patients with nephropathy (mean GFR 54 ml/min/1.73 m2) had a 30- to 40% decrease in insulin lispro’s clearance [41].
However, patients with kidney disease had lower overall and peak insulin metabolic effects, indicating that higher injection doses would be needed for comparable metabolic control to those without renal disease. The discovery that insulin lispro, a novel short-acting insulin analogue, preserved comparable pharmacodynamics in individuals with and without renal disease, as determined by effects on glucose metabolism, is significant [42].
In order to prevent hypoglycemia, it is evidently crucial to regularly monitor the patient’s blood glucose levels, especially if renal function deteriorates over time. As a general guideline, the insulin dosage should be lowered by 25% when the GFR falls to between 10 and 50 ml/min and by 50% when the GFR falls to less than 10 ml/min.
Peripheral insulin resistance improves with dialysis starting, thus patients typically require less insulin after they begin. Subcutaneous injections of insulin generally result in a higher insulin demand for glycemic control than intraperitoneal insulin administration for patients receiving peritoneal dialysis, according to multiple studies [43].
Oral Medications
Sulphonylureas: For many years, the primary treatment for treating type 2 diabetes mellitus has been the sulfonylureas. Although it has been suggested that they may also have extra pancreatic effects, drugs in this class mainly function by stimulating the pancreatic beta cells’ secretion of insulin through interaction with a receptor that is a subunit of an ATP-sensitive potassium channel (K+-ATP) [44]. Following oral administration, these drugs are strongly protein bound in plasma and are then well absorbed. Other drugs with stronger protein-binding affinities can decrease this protein binding, raising the quantities of free plasma.
Acetohexamide, chlorpropamide, tolazamide, and tolbutamide are among the so-called first-generation sulfonylureas. Due to the accumulation of the parent medication (chlorpropamide) and its metabolites, which have strong hypoglycaemic action (chlorpropamide, acetohexamide, tolbutamide, and tolazamide), several of these older agents were linked to prolonged and severe hypoglycaemia in patients with renal dysfunction [45].
The glipizide (Glucotrol), glimepiride (Amaryl), and glyburide (Micronase, DiaBeta, Glynase) are examples of second-generation sulfonylureas that are presently available. When these newer agents are used chronically, their elimination half-lives range from 7 to 14 hours, and their effective half-lives can reach 24 hours.
In a dialysis population, gliclazide and glipizide are the preferred agents, and no dose change has been required. Approximately 90% of a dose of glipizide is excreted as biotransformation products in urine (80%) and faeces (10%), with just 10% of a dose being excreted in urine and faeces as unmodified medication [46].
When GFR decreases, there is a higher chance of hypoglycemia due to the renal clearance of sulfonylureas and their metabolites. Because glimepiride and glyburide contain two active metabolites that are partially removed by the kidney, hypoglycemia is significantly enhanced in patients with GFR <60 ml/min/1.73 m2 [47]. When eGFR is less than 60 ml/min/1.73 m2, glyburide should be avoided. Glimepiride should not be used with an eGFR of less than 30 ml/min/1.73 m2 and should be used cautiously if it is <60 ml/min/1.73 m2. Because of the risk of hypoglycemia, glipizide should be taken cautiously in patients with an eGFR less than 30 ml/min/1.73 m2 (Figure 2). Less than 10% of glipizide is eliminated renally [48].
Pharmacology of Sulphonyl-Ureas
The pharmacokinetics and/or pharmacodynamics may change in patients with renal impairment due to the strong protein binding of glipizide and the fact that hepatic biotransformation is the main route of elimination. Therefore, care must be used when administering SU agents in patients with advanced stage CKD and those who are receiving dialysis to prevent hypoglycaemia.
Long-term hepatic metabolism of glyburide produces a number of metabolites, which are then equally excreted by the kidneys and liver. The majority of a dose is eliminated as metabolites in the urine, with around 50% of the dose appearing in the faeces. Less than 5% of the parent chemical was recovered from the urine [49].
Glyburide does not seem to accumulate in people with renal impairment, and its clearance does not seem to be correlated with kidney function levels. The haemodialysis patients had a higher insulin AUC, despite a small increase in the glyburide elimination half-life from 3.3 hours to 5.0 hours. However, glyburide metabolites that have some hypoglycaemic activity tend to accumulate in individuals who have renal failure and may therefore increase the risk of hypoglycaemia while using glyburide in these patients. Many studies warn that using glyburide in patients with severe renal insufficiency can result in hypoglycaemia, most likely as a result of an active metabolite.
Glipizide should likely be the preferred sulfonylurea in patients with severe renal failure due to its favourable pharmacokinetics in those with decreased GFR, yet avoided its sustained-release form has been advised. Two main metabolites of glimepiride are also produced by the liver, and one of these has been demonstrated to have some pharmacologic effect in animals. There is a 5-8-hour elimination half-life. A dosage is excreted in faeces and shows in the urine around 60% of the time [50].
With little to no parent medication secreted in the urine, almost all urinary excretion is as metabolites. While glimepiride does not build up in patients with renal failure, its metabolites are excreted less often in the urine [51]. Glimepiride use has been associated with prolonged hypoglycaemia in individuals with renal impairment; hence, patients with decreased GFR should use the medication with caution and at a lower dose [52].
Meglitinides
Nateglinide, repaglinide, and mitiglinide are three insulin secretagogues that are now used in clinical settings due to their quick onset of action and improvement in hyperglycaemia. Repaglinide is almost fully metabolised in the liver by CYP enzymes after oral treatment, primarily CYP2C8 (70%) and CYP3A4 (30%). Repaglinide is converted by CYP3A4 by oxidative biotransformation into the inactive metabolites M2 (dicarboxylic acid) and M1 (aromatic amine), or it is directly conjugated with glucuronic acid to generate M7 (acyl glucuronide) [53]. Following hepatic Organic anion transporting polypeptide 1B1 (OATP1B1)-mediated absorption, repaglinide is subsequently metabolised by CYP2C8 and CYP3A4 before being eliminated in the bile, which is likely mediated, at least in part, by P-GP. Only 8% of the parent medication is excreted unchanged in the urine.
In patients with advanced CKD (creatinine clearance (CrCl) 30 mL/min), the drug exhibits a nearly 4-fold increase in half-life after 1 week of treatment, and significantly increases the area under the curves (AUCs) after both single and multiple dosing [23]. This is in contrast to subjects with normal renal function (CrCl >80 mL/min). Since there was no difference in maximal plasma concentrations, it is likely that kidney disease has no impact on the drug’s bioavailability and that gastrointestinal tract metabolism and transport are unaffected [54].
These findings imply that patients with severe CKD have impaired hepatic clearance of repaglinide, which may be mediated via OATP1B1, CYP2C8, CYP3A4, and/or P-GP. As a result of lower protein and gene expression, uraemia also causes hepatic and intestinal CYPs, particularly CYP3A, to function less efficiently [55].
Mitiglinide has a stronger affinity for Kir6.2/SUR1 than it does for the other two insulin tropic SU receptor ligands (mitiglinide > repaglinide > nateglinide), allowing it to specifically inhibit Kir6.2/SUR1 in pancreatic beta cells.
These findings imply that mitiglinide has little negative effects on the cardiovascular system and operates selectively on pancreatic beta cells to increase the production of insulin.
Mitiglinide is therefore thought to have a lower risk of causing hypoglycaemia than nateglinide, even in patients with renal impairment. In patients receiving dialysis, mitiglinide has a time to maximum concentration (Tmax) and a half-life of roughly 0.41 and 11.7 hours, respectively [56].
Mitiglinide has a half-life of 1.48 and 3.22 h in patients with normal renal function and stage 3 CKD, respectively, hence caution must be used while administering the drug to patients with renal impairment to prevent excessive blood glucose lowering.
Due to the extended half-life of mitiglinide in patients on dialysis compared to those with normal renal function, adequate blood glucose levels can be maintained even at a low dose of mitiglinide, not only during the postprandial period but also before meals. Even when given for a brief period of time, mitiglinide dramatically improved glycaemic control, lipid levels, and intradialytic weight gain. We concluded that mitiglinide significantly reduced fasting plasma glucose in dialysis patients as well as haemoglobin A1C and glycated albumin, the overall index of glycaemic management in type 2 diabetes [57].
Biguanides
The Biguanides are a class of medications that includes Phenformin and Metformin (Glucophage). One of the many well-established benefits of metformin, the first-line oral treatment for type 2 diabetes, is a lower risk of macro vascular problems. Patients with renal impairment have not been prescribed it by doctors because to concerns about the possibility of lactic acidosis, which is made worse by multiple case reports where it is mentioned. A comprehensive examination of this research casts doubt on the validity of these claims, since metformin usually acts as a “innocent bystander” in patients who are critically ill and in conditions like sepsis or hypovolemia that are known to cause lactic acidosis. Actually, the data supports the safe use of metformin by highlighting the notably higher risks associated with the alternatives, such as severe hypoglycaemia in patients on sulphonylureas and/or insulin and fluid retention in those taking thiazolidinedione [58].
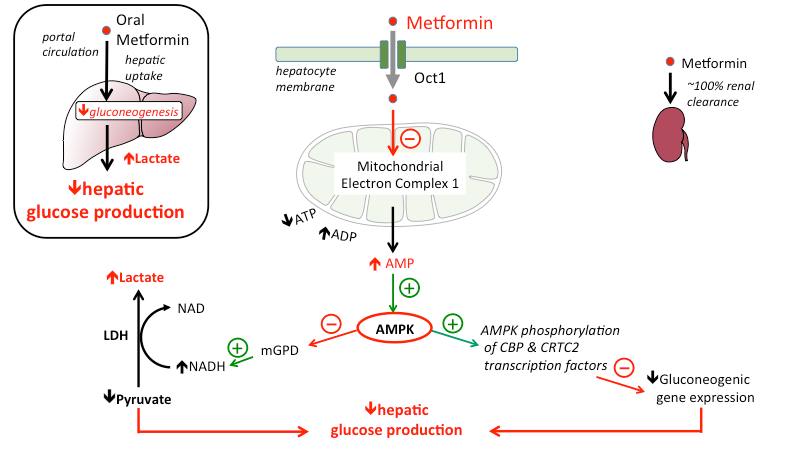
Type 2 diabetes can be effectively managed with the medication metformin. It has also been shown to control blood sugar and mitigate the long-term consequences of diabetes, including macro vascular disease. Because of the drug’s delayed clearance and consequent accumulation, there is a persistent and widespread worry about administering metformin to patients with chronic renal impairment [59]. This is because the medication may cause lactic acidosis. On the other hand, a critical analysis of the available data suggests that metformin has minimal impact on lactic acidosis and that tissue hypoxia is the primary risk factor (Figure 3).
Without the need for insulin, the biguanide metformin decreases blood sugar levels primarily by blocking hepatic gluconeogenesis [60]. It is the first-choice oral treatment for type 2 diabetes mellitus, and there is growing interest in its possible use to treat type 1 diabetes as well. Extensive clinical experience has been complemented by positive findings from the UK-PDS, which showed that metformin can lower the incidence of macro vascular complications (myocardial infarction, angina, stroke, sudden death, and peripheral vascular disease) in overweight patients with type 2 diabetes. This advantage was unaffected by other traditional cardiovascular risk factors or by managing blood sugar levels. Unlike oral replacements and insulin, metformin does not increase body weight or increase the risk of hypoglycaemia [61].
The dose of metformin should be evaluated if the serum creatinine level is greater than 130 mmol/l (or the estimated GFR is less than 45 ml/min/1.73 m2), according to the most recent NICE guidelines and metformin should be discontinued in patients whose creatinine level reaches 150 mmol/l or whose eGFR drops to less than 30 ml/min/1.73 m2. According to the most recent NICE guidelines, if the serum creatinine level is greater than 130 mmol/l (or the estimated GFR is less than 45 ml/min/1.73 m2), the dose of metformin should be evaluated. Metformin should never be administered to patients whose liver function, oxygenation, tissue perfusion, or both are severely compromised. However, clinicians are doing their patients harm when they abruptly and improperly halt metformin medication in patients with stable chronic renal illness and type 2 diabetes [62].
With an elimination half-life that has been reported to range from 1.5 to 8.7 hours, metformin is not protein bound and is removed unmodified by the kidney by both glomerular ultrafiltration and tubular secretion. In 12 to 24 hours, 90% of a dosage is eliminated. Metformin does not go through hepatic metabolism, in contrast to phenformin. Metformin elimination is decreased in people whose GFRs are lower. Cimetidine inhibits metformin’s tubular secretion and total clearance. Metformin has been used in individuals with reduced kidney function with dose adjustments; however, as will be addressed below, metformin is contraindicated in patients with renal insufficiency due to its link to the development of lactic acidosis [63].
Metformin should not be administered to patients whose blood creatinine levels are 1.4 mg/dl or higher in women or 1.5 mg/dl in males due to the risk of lactic acidosis. Metformin can be effectively removed from the bloodstream during haemodialysis. Metformin-associated lactic acidosis has been managed with moderate success using haemodialysis, which corrects the acidosis and eliminates metformin [64].
Thiazolidinedione’s
The peroxisome proliferator-activated receptor (PPAR) is the mechanism of action for the thiazolidinedione pioglitazone (Actos) and rosiglitazone (Avandia), which reduce insulin resistance. They also reduce hepatic gluconeogenesis and boost peripheral insulin utilisation. Following the reporting of numerous fatal hepatotoxicity instances, the medication troglitazone, another in this class, was taken off the market.
Both pioglitazone and rosiglitazone create several metabolites upon nearly total hepatic metabolism. Both medications have a strong protein binding, mostly to albumin. Less than 1% of the original medication is found in the urine in its undisturbed form, and rosiglitazone has two primary metabolites, none of which is active and an elimination half- life of 3.4 hours. Pioglitazone has six metabolites, three of which are active, and an elimination half-life of between three to seven hours [65].
When renal insufficiency is present, neither the parent medication nor its primary metabolites, pioglitazone or rosiglitazone, accumulate. In fact, the area under the curve (AUC) for both medications is lower in individuals with severe renal failure, maybe as a result of decreased protein binding. There is no impact of haemodialysis on the pharmacokinetics of these medications. Therefore, in individuals with reduced GFR, it is not required to lower the doses of rosiglitazone and pioglitazone. Congestive heart failure (CHF) and edema are two thiazolidinedione side effects that may be significant to nephrologists.
Hemodilution causes a decrease in haematocrit and haemoglobin, while some individuals using this class of drug have an increase in plasma volume. In 3-5% of patients using these medications as monotherapy, edema develops. This frequency is slightly higher in patients receiving insulin concurrently than in individuals receiving other oral hypoglycaemias in combination therapy mode [66].
The pathophysiology of thiazolidinedione-induced edema development is likely complex and may involve increased sympathetic nervous system activity, decreased vascular permeability, and renal salt and water retention. thiazolidinedione’s and insulin may work together to cause vasodilatation, which increases the absorption of sodium and causes edema. Patients treated with thiazolidinedione monotherapy have a low incidence of CHF; however, patients who also take insulin and have risk factors for CHF are more likely to develop the condition, particularly when thiazolidinedione dosages are increased [67].
Alpha Glucosidase Inhibitors
Postprandial hyperglycaemia is reduced by the α-glucosidase inhibitors miglitol (Glyset) and acarbose (Precose), which prevent the intestinal conversion of oligosaccharides into simpler sugars. The most well-known member of this category, acarbose, is absorbed very little from the gastrointestinal system because intestinal flora and enzymes mostly break it down into at least 13 metabolites, at least one of which has some biological function. Acarbose and its active metabolite are somewhat absorbed, but less than 2% of the dose is detected in the urine. About two hours is the half-life of elimination [68]. It is unknown what therapeutic significance this has, but patients with decreased renal function may have several-fold increases in the drug’s and its metabolites’ plasma levels.
It is not advised to use acarbose in individuals with severe renal impairment due to the paucity of information regarding long-term use in this population with impaired kidney function [69].
Approximately 50–100% of a dose of miglitol is absorbed systemically, which is higher than that of acarbose. Up to 95% of a dose can be found in the urine after renal elimination of this medication, which has little protein binding and is not metabolised. A prolonged terminal elimination phase that might last several days precedes the plasma elimination half- life, which is between 0.4 and 1.8 hours. When a patient has severe renal impairment, the administration of miglitol is not advised since it can accumulate in those people. Acarbose and miglitol have the potential to decrease the absorption of further oral hypoglycaemic medications [70].
The main adverse effects of these drugs are jaundice and increased liver enzymes, both of which can be resolved by discontinuing the medicine. The majority of the other side effects are gastrointestinal, such as diarrhoea and flatulence [71].
Acarbose
Acarbose is only broken down in the digestive system, primarily by intestinal bacteria but also by digestive enzymes. 51% of an oral dose was excreted in the faces as unabsorbed drug-related radioactivity within 96 hours of consumption. Since acarbose only affects the gastrointestinal tract locally, a low systemic bioavailability of the parent substance is preferred from a therapeutic standpoint [72].
About 34% of the dose of these metabolites were ingested, with the remainder being eliminated in the urine. The main metabolites, which are conjugates of sulphate, methyl, and glucuronide, have been discovered as 4-methylpyrogallol derivatives. Additionally, one metabolite that is produced when acarbose is broken down into a glucose molecule also possesses alpha-glucosidase inhibitory action.
Together with the original substance, which was also extracted from the urine, this metabolite makes up around 2% of the total dose that was given. Patients with severe renal impairment (CrCl 25 mL/min) reached rises roughly 5-fold higher for peak plasma concentrations of acarbose and 6-fold higher for AUC values than subjects with normal renal function, even though only 2% of an oral dose of acarbose was absorbed as active medication.
Acarbose therapy for diabetic individuals with substantial renal failure is not advised due to the lack of long- term clinical trials in these patients [73].
Miglitol
Another alpha-glucosidase inhibitor called miglitol is not metabolised in people or any other animal species that has been investigated thus far. Plasma, urine, and faeces have not revealed any metabolites, demonstrating the absence of either presystemic or systemic metabolism. By renal excretion, miglitol is removed as an unaltered medication. When compared to subjects with CrCl >60 mL/min, patients using miglitol 25 mg three times a day showed plasma levels of the medication to be more than 2-fold higher. Miglitol operates locally, therefore adjusting the dose to account for the higher plasma concentrations is not possible. However, because the safety of miglitol in these patients has not yet been clarified, treating patients with CrCl 25 mL/min with it is not advised [74].
However, none of the preceding research examined the effectiveness of an alpha glucosidase inhibitor used alone in CKD patients receiving dialysis.
In type 2 diabetics receiving dialysis, our team has previously contrasted the effects of voglibose monotherapy with an add-on medication, pioglitazone combination with voglibose. In patients receiving dialysis, we discovered that alpha-glucosidase inhibitor monotherapy decreased haemoglobin A1C levels by about 0.4%. Furthermore, our findings suggested that voglibose is beneficial for maintaining the glycaemic state because, during the course of treatment, it did not exacerbate or improve glycaemic control in patients with a high level of insulin resistance. To achieve good glycaemic control in type 2 diabetes patients with, we showed that combination therapy with pioglitazone is more successful than voglibose monotherapy [75].
DPP-4 Inhibitors
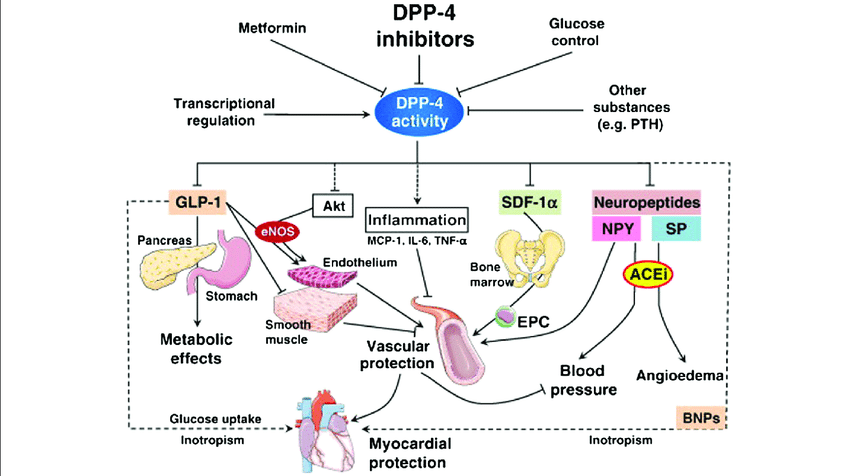
New drugs that target the so-called incretin hormone pathway may have certain advantages over current oral glucose-lowering medications in terms of many side effects. Insulin production is stimulated by the intestinal hormone glucagon-like peptide-1 (GLP-1) in a glucose-dependent way. However, type 2 diabetic patients typically have lower levels of this secretion after meals, which could amplify postprandial hyperglycaemia. The enzyme dipeptidylpeptidase-4 (DPP-4) quickly inactivates GLP-1. Consequently, using selective DPP- 4 inhibitors is a successful method of enhancing postprandial GLP-1 response (Figure 4). The main differences among DPP- 4 inhibitors that can be utilised to treat type 2 diabetes [76].
Sitagliptin
Sitagliptin is a DPP-4 inhibitor that is administered orally once daily to individuals with type 2 diabetes. It is extremely selective. Incretins, GLP-1, and glucose- dependent insulinotropic polypeptide are all degraded and rendered inactive more slowly by DPP-4 inhibitors. While GLP-1 also inhibits glucagon release, these two incretins regulate glucose homeostasis via promoting insulin release. These two incretin actions depend on blood glucose levels. The main CYP isozyme, CYP3A4, and CYP2C8 both have a small role in the restricted oxidative metabolism of sitagliptin. However, because the CYP system plays such a tiny role in sitagliptin metabolism, clinically significant drug-drug interactions mediated by CYP3A4 or CYP2C8 are likely to be insignificant. This is in contrast to studies done on sulfonylureas, meglitinides (repaglinide), and thiazolidinedione’s (rosiglitazone), which are other glucose- lowering medications [77].
Sitagliptin is predominantly removed by the kidneys, with 80% of the oral dose being excreted unaltered in urine. Excretion is assumed to occur by glomerular filtration and active secretion. According to 24-h CrCl, plasma sitagliptin exposure increases after a single oral dosage of sitagliptin as renal function declines. Patients with moderate renal insufficiency (CrCl 30–50 mL/min), severe renal insufficiency (CrCl 30 mL/min, not on dialysis), or end-stage renal disease (ESRD) on dialysis had roughly 2.3–, 3.8–, or 4.5–fold higher plasma sitagliptin exposures, respectively, and the Cmax increased by 1.4– to 1.8–fold.
Based on these results, sitagliptin dose adjustments are advised for patients with type 2 diabetes, moderate to severe renal insufficiency, as well as those with ESRD needing dialysis, in order to achieve plasma sitagliptin concentrations comparable to those in patients with normal renal function. In individuals with moderate to severe renal insufficiency, including those receiving peritoneal dialysis, sitagliptin dose-adjustment therapy lowered haemoglobin A1C by 0.7% at 54 weeks [78].
Linagliptin
Linagliptin is significantly protein bound (>80% at the therapeutic dose), unlike the other DPP-4 inhibitors. DPP- 4 is expressed in a variety of tissues and is also available in plasma as soluble DPP-4, hence binding to soluble DPP-4 may affect the pharmacokinetics of linagliptin. At therapeutic plasma concentrations of linagliptin, the concentration-dependent plasma-protein binding was principally accounted for by the high-affinity but quickly saturable binding of linagliptin to its target DPP-4. Despite the persistence of modest levels in the body, accumulation of linagliptin in tissues is improbable because the DPP-4 binding capacity is saturated at low dosages. With 84.7 and 58.2% of the dose, faecal elimination was the main excretion pathway; renal excretion was responsible for 5.4 and 30.8% of the dose given intravenously or orally, respectively. The most prevalent radioactive species in all of the studied matrices was unaltered linagliptin. After oral treatment, the major metabolite CD1790 (pharmacologically inactive) was seen with >10% of the parent compound’s systemic exposure. Although additional metabolites were found, their impact on the drug’s overall disposition and elimination was minimal. After administering 5 mg, the amount of unmodified linagliptin excreted by the kidneys was 1%. In contrast to other DPP-4 inhibitors, linagliptin’s absolute bioavailability was found to be around 30%, making renal excretion a minor route of elimination at therapeutic dose levels. As a result, a dose adjustment in patients with renal impairment is not intended for linagliptin [79].
Glycaemic Control in CKD
Delaying the onset of diabetes complications requires strict adherence to glucose control, which can be difficult for even highly skilled medical professionals. Controlling blood sugar in people with chronic kidney disease (CKD) introduces an additional layer of complexity. An in-depth understanding of the drugs that can be used safely as well as how kidney illness impacts the way these drugs are metabolised is necessary. Furthermore, since renal illness can change our ability to read the data, the glycaemic target needs to be customised for each patient.
Glycaemic Goal in CKD
Reduced A1C values are linked to an increased risk of hypoglycaemia, therefore various people require varied A1C objectives. The most vulnerable groups to the consequences of hypoglycaemia include the elderly and fragile, those on insulin and sulfonylureas, those with CKD, and those with irregular eating patterns. These conditions can result in damage, myocardial infarction, seizures, stroke, or even death. Higher A1C objectives must to be taken into account in children, those with CKD, those with shorter life expectancies, and those with a history of severe hypoglycaemia or hypoglycaemia unawareness [80].
The Diabetic Kidney Disease (DKD) Controversies Conference, organised by KDIGO, tackled several topics related to DKD, such as the proper targets for glycaemic control. Regarding the optimal glucose target in patients with stage 3 or worse CKD, there are not enough studies or data available. A1C values >9% and <6.6% were linked to higher mortality in the presence of non-dialysis dependent CKD stage 3 or worse, according to one study. Maintaining an A1C in the 7–8% range is beneficial for diabetic ESRD patients, as A1C values above or below 7% are associated with higher risks of cardiovascular and all-cause mortality [81].
A recent observational study discovered that there was no difference in survival between older and younger patients; those who began dialysis before the age of 60 had a lower chance of surviving with an A1C >8.5% (HR 1.5) than those with an A1C 6.5–7.4%.
Strategy for glycaemic control and other risk factors: Everybody wants to minimise the development of microvascular and macro vascular problems by maximising glycaemic control. The patient’s comfort and the doctor’s advice should guide the pharmaceutical regimen, which should be tailored to each patient’s needs, particularly when renal function varies. Injections four times a day on average are administered by MDI to individuals who require insulin. With an insulin pump providing a continuous subcutaneous infusion, the closest approximation of physiologic insulin secretion can be reached. The pump only uses one kind of insulin, such as a rapid-acting analogue, which functions as the correction, bolus, and basal forms of the hormone. Endocrinologists and skilled diabetes educators should supervise the use of insulin pumps, which call for monitoring on the part of the patient.
There are devices called Continuous Glucose Monitoring Systems (CGMS) that can monitor glucose levels continuously. The glucose is measured every five minutes by a tiny plastic catheter that is implanted subcutaneously. The glucose may be seen in real time, and patients can see both rising and decreasing patterns. The ability to set alarms for high and low readings is an additional bonus [82].
A holistic approach to care is recommended in addition to glucose control. In order to manage weight, enhance nutrition, alter food consumption, and keep an eye on blood sugar levels, behavioural and lifestyle adjustments are crucial. Nephropathy should be treated with the right medication, sometimes in consultation with a nephrologist. Blood pressure management also needs to be closely monitored. The primary cause of death in this population is cardiovascular disease (CVD), which is largely caused by diabetes and is a major cause of death for those with chronic kidney disease (CKD). Microalbuminuria, albuminuria, and a decreasing GFR are recognised indicators of cardiovascular disease.
Diabetes and CKD together have a very strong effect on CVD risk, which calls for strict management of risk variables. Dyslipidaemia and weight management should be taken care of in addition to hypertension. In those with diabetic kidney disease, nutrition is crucial because intake of sugars and harmful fats must be balanced with intake of salt, potassium, phosphorus, and protein. Increased activity and weight loss are often advised for patients who are overweight or obese, taking cardiac stress tests into consideration. To safely achieve nutritional, activity, and weight loss objectives, it is helpful to work with a certified diabetes educator and professional dietician. Some of the concerns related to managing diabetic kidney disease, such as controlling blood pressure and dyslipidaemia, are covered at the KDIGO Controversies Conference. The American Diabetes Association also offers guidelines for controlling dyslipidaemia and blood pressure [83].
Medical therapy in dialysis and post-transplant patients: A small number of oral medications are safe for use in dialysis patients, especially if their diabetes is quite mild. For glycaemic management, however, the majority of people will require insulin. Individuals undergoing haemodialysis (HD) may exhibit varying insulin clearance rates, which could be influenced by the dialysis schedule. Continuous glucose monitoring during HD is something we have done on patients, and what we have discovered is that each patient has a distinct glycaemic response during HD, thus insulin regimes must be customised to prevent hyper- and hypoglycaemia both during and after HD. Large levels of glucose in the dialysate are exposed to by patients receiving peritoneal dialysis (PD), which increases the risk of uncontrolled hyperglycaemia. It is ideal for individuals getting PD on a regular basis to follow a typical basal/bolus insulin regimen.
A fixed mixture insulin combination, like 70/30 or 75/25 insulins, administered at the start of PD, may be the most effective way to address the increased glucose load in night- time PD utilising a cycler. Dialysate glucose concentrations are frequently altered by the nephrologist prescribing PD due to the necessity for varying degrees of fluid clearance; these modifications must be communicated to the endocrinologist in order to adjust insulin dosages accordingly. Glycaemic control may drastically deteriorate in the first few months following transplantation. This is because insulin resistance has increased along with the use of anti-rejection medications such as sirolimus, calcineurin inhibitors, and glucocorticoids. Additionally, patients may notice other changes in their daily schedules, such as modifications to their diet or level of activity. Furthermore, patients can encounter further variations in their daily schedules, such as modifications to their food, level of exercise, and prescriptions. Glycaemic control might vary significantly due to the numerous factors involved, involving frequent blood glucose checks and medication modifications [84].
Conclusion
The last several years have seen the introduction of numerous medications for the management of hyperglycaemia in people with diabetes mellitus. It’s crucial to understand that insulin and glucose metabolism might change over time, affecting a patient’s need for insulin and oral treatments in the context of chronic kidney disease (CKD) and diabetes mellitus. In patients with impaired renal function, certain of the more recent medications, including biguanides, may be more hazardous. Others, like several sulfonylureas, have the potential to cause individuals with lower GFRs to have severe and sustained hypoglycaemia.
Although therapeutic possibilities with oral agents in type 2 diabetes mellitus are increasing, the presence of CKD is an important limitation for using the majority of the currently available oral antidiabetic drugs. In recent years, several promising drugs have been introduced in the therapeutic armamentarium of affected patients. However, recommended oral antidiabetic agents differ between countries. Therefore, kidney function of each patient should be assessed before initiating antidiabetic therapy, and careful monitoring against hypoglycaemia is necessary, in particular when using insulin secretagogues or combination therapy. Whether the pharmacokinetic differences outlined above will translate into clinically relevant differences concerning the efficacy and safety profiles of these drugs in patients with type 2 diabetes with CKD or ESRD remains to be determined. Furthermore, the long-term efficacy and safety of the DPP- 4 inhibitors remain largely unknown. Clinical data are still needed, in particular on the long-term safety of CKD patients receiving dialysis and the durability of glucose control, cardiovascular outcomes, diabetes complications, and all- cause mortality.
Several areas of patient care must be addressed in the management of patients with diabetes and nephropathy. Glycemic management must be achieved in a safe, supervised manner, with special attention paid to the patient’s needs in order to minimise problems. Regular nephropathy screening is necessary to detect microalbuminuria or GFR declines, and the diabetes treatment plan should be adjusted based on the results. Diabetic nephropathy and its complications require multifactorial treatment and prevention. A multifaceted care programme that slows the progression of the disease can be provided by a dialectologist, nephrologist, dietician, diabetes educator, and other specialists with experience in diabetic complications.
As a result, careful observation is necessary, and when feasible, oral medications with minimal to no pharmacokinetic alteration should be used in the context of compromised renal function.
References
-
Kaul K, Tarr JM, Ahmad SI, Kohner EM, Chibber R (2013) Introduction to diabetes mellitus. Adv Exp Med Biol 771: 1-11.
-
Farmaki P, Damaskos C, Garmpis N, Garmpi A, Savvanis S, et al. (2020) Complications of the Type 2 Diabetes Mellitus. Current cardiology reviews 16(4): 249-251.
-
Goyal R, Singhal M, Jialal I (2023) Type 2 Diabetes. In: StatPearls. Treasure Island (FL): StatPearls Publishing.
-
Blair M (2016) Diabetes mellitus review. Urologic nursing 36(1): 27-36.
-
Katsarou A, Gudbjörnsdottir S, Rawshani A, Dabelea D, Bonifacio E, et al. (2017) Type 1 diabetes mellitus. Nature reviews Disease primers 3(1): 17016.
-
Olokoba AB, Obateru OA, Olokoba LB (2012) Type 2 diabetes mellitus: a review of current trends. Oman medical journal 27(4): 269-273.
-
Leahy JL (2005) Pathogenesis of type 2 diabetes mellitus. Archives of medical research 36(3): 197-209.
-
Mahler RJ, Adler ML (1999) Type 2 diabetes mellitus: update on diagnosis, pathophysiology, and treatment. The Journal of Clinical Endocrinology & Metabolism 84(4): 1165-1171.
-
Sagoo MK, Gnudi L (2020) Diabetic nephropathy: an overview. Methods Mol Biol 2067: 3-7.
-
Dronavalli S, Duka I, Bakris GL (2008) The pathogenesis of diabetic nephropathy. Nature clinical practice Endocrinology & metabolism 4(8): 444-452.
-
Duran-Salgado MB, Rubio-Guerra AF (2014) Diabetic nephropathy and inflammation. World journal of diabetes 5(3): 393-398.
-
Tervaert TWC, Mooyaart AL, Amann K, Cohen AH, Cook HT, et al. (2010) Pathologic classification of diabetic nephropathy. Journal of the American Society of Nephrology 21(4): 556-563.
-
Umanath K, Lewis JB (2018) Update on diabetic nephropathy: core curriculum 2018. American journal of kidney diseases 71(6): 884-895.
-
Busch M, Nadal J, Schmid M, Paul K, Titze S, et al. (2016) Glycaemic control and antidiabetic therapy in patients with diabetes mellitus and chronic kidney disease– cross-sectional data from the German Chronic Kidney Disease (GCKD) cohort. BMC nephrology 17(1): 59.
-
Migdalis IN, Papanas N, Ioannidis IM, Sotiropoulos AE, Raptis AE, et al. (2021) Antidiabetic and other therapies used in subjects with diabetes and chronic kidney disease in a hospital-based clinic population in Greece. Journal of Clinical Medicine 10(10): 2104.
-
Elnaem MH, Mansour NO, Nahas AF, Baraka MA, Elkalmi R, et al. (2020) Renal outcomes associated with the use of non-insulin antidiabetic pharmacotherapy: a review of current evidence and recommendations. International Journal of General Medicine 13: 1395-1409.
-
Gor D, Gerber BS, Walton SM, Lee TA, Nutescu EA, et al. (2020) Antidiabetic drug use trends in patients with type 2 diabetes mellitus and chronic kidney disease: A cross‐ sectional analysis of the National Health and Nutrition Examination Survey. Journal of Diabetes 12(5): 385-395.
-
Mane PB, Antre RV, Oswal RJ (2012) Antidiabetic drugs: An overview. Int J Pharm Chem Sci 1(1): 301-306.
-
Deruiter JACK (2003) Overview of the antidiabetic agents. Endocrine Pharmacotherapy Module pp: 1-33.
-
Oliveria SA, Koro CE, Yood MU, Sowell M (2008) Cancer incidence among patients treated with antidiabetic pharmacotherapy. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 2(1): 47-57.
-
Washam JB, Herzog CA, Beitelshees AL, Cohen MG, Henry TD, et al. (2015) Pharmacotherapy in chronic kidney disease patients presenting with acute coronary syndrome: a scientific statement from the American Heart Association. Circulation 131(12): 1123-1149.
-
Barreto FC, de Oliveira RA, Oliveira RB, Jorgetti V (2011) Pharmacotherapy of chronic kidney disease and mineral bone disorder. Expert Opinion on Pharmacotherapy 12(17): 2627-2640.
-
Chen L, Yang T, Lu DW, Zhao H, Feng YL, et al. (2018) Central role of dysregulation of TGF-β/Smad in CKD progression and potential targets of its treatment. Biomedicine & Pharmacotherapy 101: 670-681.
-
Raymond CB, Wazny LD, Honcharik PL (2008) Pharmacotherapeutic options for the treatment of depression in patients with chronic kidney disease. Nephrology Nursing Journal 35(3): 257-263.
-
Patel HR, Pruchnicki MC, Hall LE (2005) Assessment for chronic kidney disease service in high-risk patients at community health clinics. Annals of Pharmacotherapy 39(1): 22-27.
-
Long CL, Raebel MA, Price DW, Magid DJ (2004) Compliance with dosing guidelines in patients with chronic kidney disease. Annals of Pharmacotherapy 38(5): 853-858.
-
Kemp JA, Leeson PD (1993) The glycine site of the NMDA receptor—five years on. Trends in Pharmacological Sciences 14(1): 20-25.
-
Bolli GB, Di Marchi RD, Park GD, Pramming S, Koivisto VA (1999) Insulin analogues and their potential in the management of diabetes mellitus. Diabetologia 42(10): 1151-1167.
-
Luijf YM, van Bon AC, Hoekstra JB, DeVries JH (2010) Premeal injection of rapid-acting insulin reduces postprandial glycemic excursions in type 1 diabetes. Diabetes care 33(10): 2152-2155.
-
Lampe J, Penoyer DA, Hadesty S, Bean A, Chamberlain L (2014) Timing is everything: results to an observational study of mealtime insulin practices. Clinical Nurse Specialist 28(3): 161-167.
-
Scott DA, Fisher AM (1935) Crystalline insulin. Biochemical Journal 29(5): 1048-1054.
-
Horvath K, Jeitler K, Berghold A, Ebrahim SH, Gratzer TW, et al. (2007) Long‐acting insulin analogues versus NPH insulin (human isophane insulin) for type 2 diabetes mellitus. Cochrane database of systematic reviews 2.
-
Swinnen SG, Simon AC, Holleman F, Hoekstra JB, DeVries JH (2011) Insulin detemir versus insulin glargine for type 2 diabetes mellitus. Cochrane Database of Systematic Reviews 2011(7).
-
Dailey G, Admane K, Mercier F, Owens D (2010) Relationship of insulin dose, A1C lowering, and weight in type 2 diabetes: comparing insulin glargine and insulin detemir. Diabetes technology & therapeutics 12(12): 1019-1027.
-
Lane WS, Cochran EK, Jackson JA, Scism Bacon JL, Corey IB, et al. (2009) High-dose insulin therapy: is it time for U-500 insulin. Endocrine practice 15(1): 71-79.
-
Van den Berghe G, Wouters PJ, Bouillon R, Weekers F, Verwaest C, et al. (2003) Outcome benefit of intensive insulin therapy in the critically ill: Insulin dose versus glycemic control. Critical care medicine 31(2): 359-366.
-
Kolb H, Kempf K, Röhling M, Martin S (2020) Insulin: too much of a good thing is bad. BMC medicine 18(1): 1-12.
-
Hoffman A, Ziv E (1997) Pharmacokinetic considerations of new insulin formulations and routes of administration. Clinical pharmacokinetics 33(4): 285-301.
-
Svehlikova E, Mursic I, Augustin T, Magnes C, Gerring D, et al. (2021) Pharmacokinetics and pharmacodynamics of three different formulations of insulin aspart: a randomized, double-blind, crossover study in men with type 1 diabetes. Diabetes Care 44(2): 448-455.
-
Patton JS, Bukar JG, Eldon MA (2004) Clinical pharmacokinetics and pharmacodynamics of inhaled insulin. Clinical pharmacokinetics 43(12): 781-801.
-
Hübinger A, Weber W, Jung W, Wehmeyer K, Gries FA (1992) The pharmacokinetics of two different concentrations of short-acting insulin, intermediate- acting insulin, and an insulin mixture following subcutaneous injection. The clinical investigator 70(7): 621-626.
-
Rendell M (2004) The role of sulphonylureas in the management of type 2 diabetes mellitus. Drugs 64(12): 1339-1358.
-
Dills DG, Schneider J (1996) Clinical evaluation of glimepiride versus glyburide in NIDDM in a double-blind comparative study. Glimepiride/Glyburide Research Group. Hormone and metabolic research 28(9): 426- 429.
-
Szoke E, Gosmanov NR, Sinkin JC, Nihalani A, Fender AB, et al. (2006) Effects of glimepiride and glyburide on glucose counterregulation and recovery from hypoglycemia. Metabolism 55(1): 78-83.
-
McCall AL (2001) Clinical review of glimepiride. Expert Opinion on Pharmacotherapy 2(4): 699-713.
-
Pantalone KM, Kattan MW, Yu C, Wells BJ, Arrigain S, et al. (2010) The risk of overall mortality in patients with type 2 diabetes receiving glipizide, glyburide, or glimepiride monotherapy: a retrospective analysis. Diabetes care 33(6): 1224-1229.
-
Melander A (1996) Clinical Pharmacology of Sulfonylureas. Metabolism 36(2): 12-16.
-
Zhai S, Georgy A, Liang Z, Zhi J (2016) Pharmacokinetic and pharmacodynamic drug interaction study of piragliatin, a glucokinase activator, and glyburide, a sulfonylurea, in type 2 diabetic patients. Clinical pharmacology in drug development 5(6): 552-556.
-
Lebovitz HE (1985) Glipizide: A Second‐generation Sulfonylurea Hypoglycemic Agent; Pharmacology, Pharmacokinetics and Clinical Use. Pharmacotherapy 5(2): 63-77.
-
Cvetković RS, Plosker GL (2007) Exenatide: a review of its use in patients with type 2 diabetes mellitus (as an adjunct to metformin and/or a sulfonylurea). Drugs 67(6): 935-954.
-
Deacon CF, Lebovitz HE (2016) Comparative review of dipeptidyl peptidase‐4 inhibitors and sulphonylureas. Diabetes Obesity and Metabolism 18(4): 333-347.
-
Malaisse WJ (2003) Pharmacology of the meglitinide analogs: new treatment options for type 2 diabetes mellitus. Treatments in endocrinology 2: 401-414.
-
Jijakli H, Ulusoy S, Malaisse WJ (1996) Dissociation between the potency and reversibility of the insulinotropic action of two meglitinide analogues. Pharmacological research 34(4): 105-108.
-
Meneses MJ, Silva BM, Sousa M, Sá R, Oliveira PF, et al. (2015) Antidiabetic drugs: mechanisms of action and potential outcomes on cellular metabolism. Current pharmaceutical design 21(25): 3606-3620.
-
Pfeiffer AF (2016) Oral hypoglycemic agents: Sulfonylureas and meglitinides. Type 2 Diabetes, CRC Press, pp: 111-120.
-
Manski-Nankervis JA, Thuraisingam S, Sluggett JK, Kilov G, Furler J, et al. (2019) Prescribing of diabetes medications to people with type 2 diabetes and chronic kidney disease: a national cross-sectional study. BMC Family Practice 20(1): 1-11.
-
Abe M, Okada K, Soma M (2011) Antidiabetic agents in patients with chronic kidney disease and end-stage renal disease on dialysis: metabolism and clinical practice. Current drug metabolism 12(1): 57-69.
-
Zanchi A, Lehmann R, Philippe J (2012) Antidiabetic drugs and kidney disease. Swiss medical weekly 142(3738): 13629-13629.
-
Bouchi R, Sugiyama T, Goto A, Imai K, Ihana Sugiyama N, et al. (2022) Retrospective nationwide study on the trends in first‐line antidiabetic medication for patients with type 2 diabetes in Japan. Journal of Diabetes Investigation 13(2): 280-291.
-
Huri HZ, Lim LP, Lim SK (2015) Glycemic control and antidiabetic drugs in type 2 diabetes mellitus patients with renal complications. Drug design development and therapy 9: 4355-4371.
-
Deng Y, Ghamsari F, Lu A, Yu J, Zhao L, et al. (2022) Use of real-world evidence data to evaluate the comparative effectiveness of second-line type 2 diabetes medications on chronic kidney disease. Journal of Clinical Translational Endocrinology 30: 100309.
-
Reilly JB, Berns JS (2010) Selection and dosing of medications for management of diabetes in patients with advanced kidney disease. Seminars in dialysis 23(2): 163-168.
-
Yki-Järvinen H (2004) Thiazolidinediones. New England Journal of Medicine 351(11): 1106-1118.
-
Niemeyer NV, Janney LM (2002) Thiazolidinedione‐ induced edema. Pharmacotherapy 22(7): 924-929.
-
Sunder M, Chang AR, Henry RR (2003) Thiazolidinediones, peripheral edema, and type 2 diabetes: incidence, pathophysiology, and clinical implications. Endocrine Practice 9(5): 406-416.
-
Lebovitz HE (1997) Alpha-glucosidase inhibitors. Endocrinology and metabolism clinics of North America 26(3): 539-551.
-
Kalra S (2014) Alpha glucosidase inhibitors. The Journal of the Pakistan Medical Association 64(4): 474-476.
-
Van de Laar FA, Lucassen PL, Akkermans RP, Van de Lisdonk EH, Rutten GE, et al. (2005). Alpha‐glucosidase inhibitors for type 2 diabetes mellitus. Cochrane database of systematic reviews 2005(2): CD00363.
-
Leroux-Stewart J, Rabasa‐Lhoret R, Chiasson JL (2015) Chapter 45: α‐Glucosidase inhibitors. International textbook of diabetes mellitus.
-
Rosak C, Mertes G (2012) Critical evaluation of the role of acarbose in the treatment of diabetes: patient considerations. Diabetes, metabolic syndrome and obesity: targets and therapy 5: 357-367.
-
Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, et al. (2002) Acarbose for prevention of type 2 diabetes mellitus: the STOP-NIDDM randomised trial. The Lancet 359(9323): 2072-2077.
-
Campbell LK, Baker DE, Campbell RK (2000) Miglitol: assessment of its role in the treatment of patients with diabetes mellitus. Annals of Pharmacotherapy 34(11): 1291-1301.
-
Scott LJ, Spencer CM (2000) Miglitol: a review of its therapeutic potential in type 2 diabetes mellitus. Drugs 59(3): 521-549.
-
Ahren B (2007) DPP-4 inhibitors. Best Practice & Research Clinical Endocrinology & Metabolism 21(4): 517-533.
-
Scott LJ (2017) Sitagliptin: a review in type 2 diabetes. Drugs 77(2): 209-224.
-
Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, et al. (2015) Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine 373(3): 232-242.
-
Scott LJ (2011) Linagliptin: in type 2 diabetes mellitus. Drugs 71(5): 611-624.
-
Lewin A, DeFronzo RA, Patel S, Liu D, Kaste R, et al. (2015) Initial combination of empagliflozin and linagliptin in subjects with type 2 diabetes. Diabetes care 38(3): 394- 402.
-
Galindo RJ, Beck RW, Scioscia MF, Umpierrez GE, Tuttle KR (2020) Glycemic Monitoring and Management in Advanced Chronic Kidney Disease. Endocrine reviews 41(5): 756-774.
-
Corcillo A, Pivin E, Lalubin F, Pitteloud N, Burnier M, et al. (2017) Glycaemic, blood pressure and lipid goal attainment and chronic kidney disease stage of type 2 diabetic patients treated in primary care practices. Swiss medical weekly 147: 14459.
-
Schernthaner G, Ritz E, Schernthaner GH (2010) Strict glycaemic control in diabetic patients with CKD or ESRD: beneficial or deadly?. Nephrology Dialysis Transplantation 25(7): 2044-2047.
-
Lima RF, Fontbonne A, Carvalho EMFD, Montarroyos UR, Barreto MNSDC, et al. (2016) Factors associated with glycemic control in people with diabetes at the Family Health Strategy in Pernambuco. Revista da Escola de Enfermagem da USP 50(6): 937-945.
-
Tanabe H, Masuzaki H, Shimabukuro M (2021) Novel strategies for glycaemic control and preventing diabetic complications applying the clustering-based classification of adult-onset diabetes mellitus: a perspective. Diabetes Research and Clinical Practice 180: 109067.
-
Pickup J (2014) Insulin pumps. Diabetes technology & therapeutics 16(1): 17-22.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance