Anaemia and Erythropoietic Stress in Diabetes Mellitus
Patients with diabetes get anaemia more frequently than those without the disease, and the issue is worse in those who have impaired renal function. Patients with diabetes who also have anaemia may be more vulnerable to the negative effects of diabetic retinopathy, nephropathy, neuropathy, and cardiovascular disease. In addition to kidney failure, the multifactorial aetiology of anaemia in diabetes includes inflammation, nutritional inadequacies, concurrent autoimmune disorders, medications, and hormonal abnormalities. For those with nephropathy or heart failure, anaemia linked to erythropoietin insufficiency may have prognostic implications. Anaemia and erythropoietin insufficiency may arise from injury to the peritubular fibroblasts in early diabetic nephropathy, before filtration loss occurs. Chronic hyperglycemia caused by diabetes may result in a hypoxic environment in the renal interstitium, which lowers erythropoietin synthesis by peritubular fibroblasts and causes anaemia. In individuals with diabetes mellitus, anaemia may exacerbate diabetic retinopathy and nephropathy as well as have a role in the aetiology and development of cardiovascular disease. Compared to people without diabetes who have chronic kidney disease, persons with diabetic renal disease experience anaemia earlier. The ideal target haemoglobin level is still up for debate, despite the fact that erythropoietin has been used to treat renal anaemia for almost 20 years. According to the majority of guidelines, haemoglobin levels should be kept between 105 and 125 g/l. It is still unknown how correcting anaemia may help people with diabetes mellitus avoid developing left ventricular hypertrophy. In addition to screening for other diabetes-related issues, regular anaemia screening may help these patients' vascular difficulties from progressing more slowly. Retinopathy, diabetic nephropathy, postural hypotension from autonomic neuropathy, and other microvascular and macrovascular problems are all thought to be slowed down in their progression by treating anaemia.
Introduction
Globally, diabetes mellitus is becoming more common; by 2025, 300 million individuals are expected to have the illness. Anemia and erythropoietin stress in diabetes mellitus refer to the conditions where individuals with diabetes experience a decrease in the number of red blood cells or a decrease in the amount of haemoglobin in the blood, leading to symptoms such as fatigue, weakness, and shortness of breath [1]. Erythropoietin stress refers to the increased production of red blood cells by the bone marrow in response to the decreased oxygen-carrying capacity of the blood. This can occur in individuals with diabetes due to a variety of factors, including chronic inflammation, kidney disease, and the use of certain medications. Patients’ lifespans have been extended through better medical care and scientific advancements in patient treatment. But higher survival might put these individuals at risk for long-term issues and subsequently lower quality of life. One of these chronic side effects is anaemia, which is defined as having lower haemoglobin levels (less than 130 g/l in men and less than 120 g/l in women) [2]. Anaemia may be a contributing factor in the onset and advancement of diabetic retinopathy and other diabetes complications. It is also an independent risk factor for the development and progression of cardiovascular disease, congestive heart failure, and chronic kidney disease. Individuals who have diabetes mellitus may be more susceptible to the negative consequences of anaemia when they also have cardiovascular disease and damage to their organs from hypoxia.
Chronic anaemia may result in fatigue, malaise, dyspnea, and palpitations in addition to having a negative impact on cognitive function, appetite, exercise tolerance, and physical and psychological development.
Individuals with normal hematocrits are less likely than those with anaemia and coronary artery disease to experience inducible ischemia and heart failure. Furthermore, anaemia can result in artificially low HbA1c values, which can lead to under treatment of hyperglycemia and accelerate the development of diabetic problems that are both microvascular and macro vascular [3].
Keypoints
Anaemia is a frequent side effect of diabetes mellitus and a factor that independently influences the etiology and development of additional problems associated with the disease.
- In patients with diabetes mellitus, correction of anaemia improves quality of life and may delay the progression of diabetic complications.
- Elevated levels of advanced glycation end products, oxidative stress, endothelial dysfunction, abnormal red blood cells, and reduced bioavailability of nitric oxide are possible causes of erythropoietic stress in this population.
- Anaemia occurs earlier in patients with diabetic nephropathy than in nondiabetic individuals with comparable renal function.
- Treatment should seek to achieve levels of 105g/l– 125g/l until definitive proof of optimal haemoglobin levels is obtained.
Definition
Chronic kidney disease (CKD) impairs the secretion and function of erythropoietin (EPO), a hematopoietic cytokine that is mostly produced in the renal cortex. Given that glomerular filtration rate (GFR) is maintained by diabetes- induced nephron hypertrophy and that raised plasma creatinine concentration is a relatively late symptom of diabetic nephropathy, early renal injury in diabetes mellitus (DM) is typically undetected. Anaemia does, however, occur more commonly in DM people than in non-DM subjects with renal illness. Iron deficiency, autonomic neuropathy, and chronic inflammation are major additional variables, even though lower production and a muted response to EPO occur in DM with early renal impairment. Even in the early phases, recombinant human erythropoietin (rhEPO) seems to work better in individuals with diabetes mellitus (DM) than in those with CKD anaemia. However, iron deficiency poses a challenge to the efficacy of rhEPO therapy for DM patients. It is important to keep in mind how medication affects haemoglobin A1c’s dependability as a measure of glycaemic management. Anaemia and its causes are suggested to be crucial parts of treatment for patients with early diabetic kidney impairment.
Erythropoietin Production
Many investigations on humans and animals have been conducted to explain the genesis and mechanism of “EPO,” formerly known as “haemopoietin,” since hypoxia-induced erythropoiesis was proposed in 1893. Anaemia, tissue hypoxia, and decreased capillary flow (resulting from cardiac or vascular anomalies) all promote the synthesis of EPO. Current research indicates that hypoxia first triggers the manufacture of “hypoxia-inducible factor” (HIF), which then attaches to an oxygen-sensitive enhancer in the chromosome 7 transcription site of the EPO gene to initiate the synthesis of EPO. Interstitial cells in the renal cortex close to the proximal tubule, primarily fibroblasts, undergo this procedure [4].
It has been suggested that the generation of EPO serves as a functional marker for the tubulointerstitium. The splanchnic innervations of the kidneys are hypothesised to regulate EPO release. Interestingly, hypoglycaemia, insulin release, and a number of cytokines are among the stresses that, in addition to hypoxia, can cause the HIF pathway to become activated and enhance the expression of EPO and EPO-receptors. Peripheral endothelial cells, smooth muscle cells, the liver, the uterus, and the neurological system are among the extra- renal sources of EPO, as evidenced by their existence in a nephric patient [5].
![Figure 1: EPO as Functional Marker [5].](/fulltextimages/12371/fig_1.png)
Mechanism of Action of Erythropoietin
Erythroid cell proliferation and red blood cell mass are stimulated by EPO, which is recognised by EPO receptors found in bone marrow surface progenitor cells. Additionally, EPO has a variety of cellular effects in non-hematopoietic organs, such as the heart, brain, and blood vessels, which are frequently poorly defined. It contributes to the formation of brain progenitor cells and encourages angiogenesis. Preventing apoptosis through several intracellular pathways, which shields DNA from damage, is one of the main benefits of EPO. Furthermore, EPO directly inhibits several kinds of proinflammatory cytokines, including TNF-alpha and interleukin-6, to reduce cellular inflammation. EPO protects blood vessels by both encouraging angiogenesis and maintaining the integrity of endothelial cells. Additionally, experimental research has demonstrated that EPO has cardio protective benefits and increases left ventricular (LV) function. These sources account for 10% of serum EPO. The functions of EPO appear to be agonistic for cobalt, androgens, and insulin-derived growth factor, and antagonistic for inflammatory cytokines [6].
Anaemia in Diabetes Mellitus
Diabetes frequently results in anaemia, especially when diabetic renal disease is present. Anaemia has been found in roughly 25% of outpatient DM patients, both with and without renal impairment, according to cross-sectional research. Diabetes-related anaemia has a complex aetiology. While the occurrence of anaemia in type 1 DM provides a clearer understanding of the overall effect of DM on anaemia, anaemia in type 2 DM cannot be entirely attributable to diabetes by itself; coexisting conditions in the elderly can additionally play an important role. A synergistic effect exists between diabetes mellitus (DM), chronic kidney disease (CKD), and anaemia, all of which are potential risk factors for cardiovascular disease. The development of diabetic retinopathy and renal failure is independently correlated with anaemia. As a result, it not only has negative effects of its own but also accelerates Diabetes mellitus -related micro and macro vascular damage [7].
![Figure 2: Daibetes is related to Anaemia [7].](/fulltextimages/12371/fig_2.png)
Diabetes Mellitus Causes of Anaemia
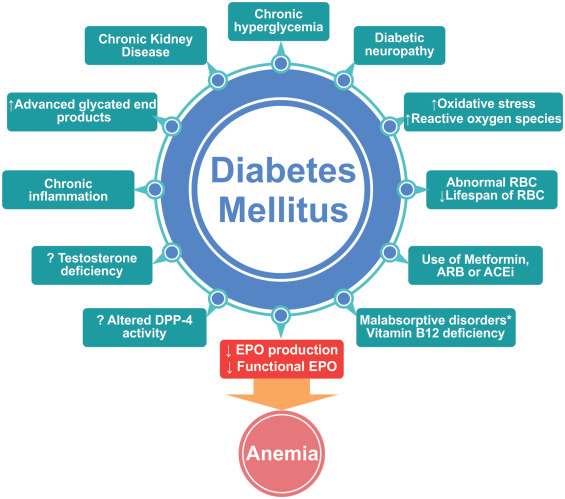
Anaemia in diabetic mellitus has a complex etiology and pathophysiology. Chronic hyperglycaemia may cause oxidative stress, aberrant red blood cells, and sympathetic denervation of the kidneys, which is linked to autonomic neuropathy. These elements encourage the renal interstitium to become hypoxic, which impairs the peritubular fibroblasts’ ability to produce erythropoietin. Early anaemia in people with diabetes mellitus is largely caused by an inappropriately low erythropoietin level. However, before there is a clear functional erythropoietin shortage, a number of additional factors may be involved in the establishment of a chronic hypoxic environment, which in turn promotes erythropoietin stress and intensifies the development of early anaemia. These include low testosterone levels, iron deficiency, elevated levels of advanced glycation end products, diabetic neuropathy, chronic inflammation, and elevated levels of glycation end products [8].
![Figure 3: Diabetes related to the complications [8].](/fulltextimages/12371/fig_3.png)
Anaemia is a condition characterized by a deficiency in red blood cells or haemoglobin, leading to reduced oxygen- carrying capacity in the blood. Diabetes mellitus, particularly type 2 diabetes, can contribute to anaemia through various mechanisms. Here are some factors that can contribute to anaemia in diabetes mellitus:
Diabetic Nephropathy
A chronic microvascular consequence of diabetes mellitus, diabetic nephropathy is characterised by a progressive capillary angiopathy within the renal glomeruli. Diabetic nephropathy is now the most common cause of end- stage renal disease and renal anaemia in developed nations due to the increased life expectancy of individuals with diabetes mellitus. Anaemia is also common in individuals with non-diabetic chronic kidney disease; however, the symptoms of anaemia in these patients develop later and are typically milder than in patients with diabetic nephropathy who have comparable levels of renal impairment due to a drop in erythropoietin levels [9].
Chronic Kidney Disease (CKD)
Diabetes mellitus is a leading cause of chronic kidney disease (CKD). CKD can lead to anaemia due to decreased production of erythropoietin by the kidneys and impaired red blood cell production. Additionally, CKD can lead to iron deficiency and vitamin B12 deficiency, further contributing to anaemia.
![Figure 5: CKD related to Anaemia [9].](/fulltextimages/12371/fig_5.png)
Iron Deficiency: Diabetes can lead to gastrointestinal issues such as gastroparesis (delayed stomach emptying) and malabsorption, which can result in iron deficiency anaemia. Additionally, some medications used to treat diabetes, such as metformin, can interfere with iron absorption. Vitamin B12 Deficiency: Metformin, a commonly prescribed medication for type 2 diabetes, can interfere with the absorption of vitamin B12, leading to a deficiency. Vitamin B12 is essential for red blood cell production, and its deficiency can result in anaemia [10]. Chronic Inflammation: Diabetes is associated with chronic low-grade inflammation, which can contribute to anaemia of chronic disease by affecting the production and lifespan of red blood cells. Increased levels of proinflammatory cytokines, which are visible prior to the onset of renal impairment, are a hallmark of diabetes mellitus, a chronic inflammatory disease. Anaemia in chronic disorders may be largely caused by proinflammatory cytokines including interleukin-1, TNF, and interferon-γ, according to studies on these molecules. This function involves erythroid progenitor cell apoptosis and repression. Patients with erythropoietin-deficiency anaemia may respond poorly to treatment with recombinant human erythropoietin due to chronic inflammation caused by hyperactivity of the cytokine network [11]. This hyperactivity may also influence other aspects of anaemia in chronic diseases, such as impairment of iron release. Renal Tubule Dysfunction: A higher risk of diabetic nephropathy is initially indicated by measurable clinical signs such as microalbuminuria. Before microalbuminuria develops, patients with diabetes mellitus have been found to have early malfunction in the renal tubules, which are the main locations of erythropoietin production. Both type 1 and type 2 diabetes mellitus have been linked to an increase in the urinary excretion of tubular damage indicators, such as retinol-binding protein and the tubular enzyme N-acetyl-β- glucosaminidase. The results of this study suggest that renal tubular failure occurs in diabetes mellitus much prior to the development of microalbuminuria [12]. Tubular Ischemia: Renal tubules absorb glucose without the assistance of insulin. Direct exposure to elevated glucose concentrations caused due to long-term hyperglycaemia may cause abnormal tubular cell development, improper collagen production, and early tubular cell apoptosis. Furthermore, this condition is linked to elevated synthesis of polyols and advanced glycation end products, as well as elevated release of angiotensin II and protein kinase C in the renal tubules [13]. Tubular ischemia and vasoconstriction may arise from these modifications. For tubular cells to survive and operate normally, peritubular capillaries are necessary. When the concentration of nitric oxide is insufficient, chronic hyperglycaemia combined with renal vasoconstriction and the cellular alterations previously stated may have a detrimental effect on the survival of cells in the peritubular capillaries.
Chronic hyperglycaemia can impair the microcirculation in the renal interstitium because insufficient nitric oxide availability may result in elevated vascular tone and improved oxygen absorption. Increased lactate concentration in the renal medulla as a result of this condition lowers pH levels and further impairs oxygen availability in the renal interstitial [13, 14].
Even in normal circumstances, the tubular and interstitial cells of the outer medulla and juxtamedullary region are in a condition of relative hypoxia. The s3 segments of the proximal tubules and the medullary thick ascending limb have a high oxygen consumption rate, which contributes to the hypoxia caused by the counter current oxygen exchange inside the vasa recta. Hypoxia-inducible factor 1 (HIF-1), one of the key mediators in cells’ adaptation to hypoxia, is produced in response to a hypoxic environment. HIF-1 increases the availability of oxygen, stimulates vasculogenesis, and modifies cellular metabolism. HIF-1 may also influence genes that induce fibrosis, potentially protecting against fibrotic processes within the kidney [14]. HIF-1 also affects pathways related to the metabolism of glucose, apoptosis and cell development, erythropoietin and vascular endothelial growth factor synthesis, iron and extracellular matrix metabolism, and erythropoietin production. The mechanisms that shield HIF-1 from protease degradation are affected by hyperglycaemia in a dose-dependent manner. As a result, there may be a potential for interstitial fibrosis due to the decreased activity of HIF-1 on profibrotic genes. By preventing oxygen from diffusing from the capillary to the tubule, this mechanism may make local ischemia worse. The hypoxic environment generated by all of these modifications could impair the ability of peritubular fibroblasts, which are primarily in responsible for producing erythropoietin, to function in the tubular interstitial [15].
Advanced End Products of Glycation
The broad class of compounds known as advanced glycation end products is created when glucose residues covalently attach to free amino groups in proteins, lipids, and nucleic acids without the aid of enzymes. Microangiopathy in diabetes mellitus has been linked to increased synthesis of advanced glycation end products. In diabetes mellitus, increased accumulation of these products might encourage nonenzymatic glycation of haemoglobin and red blood cell membrane glycoproteins, which impairs the deformability of red blood cells. These chemicals may also stimulate an increase in the generation of free oxygen radicals, which would increase the degree of oxidative stress in diabetes mellitus [16].
Advanced glycation end products play a significant part in the development of diabetic neuropathy and nephropathy.
Hematinic Absorption Abnormalities: Hematinics, which include iron, vitamin B12, and folic acid, are micronutrients that are essential for boosting haemoglobin levels in anaemic patients or for stimulating the production of red blood cells. Anaemia may also be caused by metabolic disturbances associated with diabetes. Chronic gastritis and Helicobacter pylori infection are more common in patients with diabetes mellitus, and they have an impact on the stomach’s ability to absorb minerals, particularly dietary iron. Antibodies against parietal cells are present in some type 1 diabetes mellitus patients, raising their risk of iron-deficiency anaemia and atrophic gastritis. A related malabsorptive illness, like celiac disease, affects some patients and impairs their ability to absorb iron and absorb nutrients in general. Normoblast development and proliferation during erythropoiesis depend on adequate iron reserves [17].
Reduced erythropoiesis responsiveness to erythropoietin may be the consequence of inadequate iron reserves. The most frequent reason for resistance to exogenous erythropoietin in clinical practice is iron insufficiency. According to reports, individuals with diabetes mellitus have a higher prevalence of iron deficiency than those without the disease. The difference may be explained by the possibility that long-term hyperglycaemia induces glycation-mediated regulation of transferrin receptors, potentially reducing the availability of iron by reducing the receptors’ ability to bind iron [18].
Oxidative Stress
Diabetes-related nephropathy may also be facilitated by an increase in the generation of oxidative stress-reducers like oxygen free radicals and other reactive oxygen species. The endothelium is a site of reactive oxygen species-nitric oxide pairing those results in reactive oxygen intermediates like peroxynitrite, which lower nitric oxide’s overall bioavailability. As previously indicated, this alteration may result in higher oxygen consumption and vascular tone. Decreased tubular interstitium damage from free radicals may be exacerbated by a drop in renal oxygen content and decreased nitric oxide bioavailability. As previously stated, these changes cause a hypoxic milieu to form in the tubular interstitium, which prevents erythropoietin from being produced [19].
Medications
Some medications used to treat diabetes, such as certain sulfonylureas, can cause haemolytic anaemia, a condition in which red blood cells are destroyed faster than they can be produced. Multiple drugs are frequently taken by patients with type 2 diabetes mellitus to manage their diabetes symptoms and other coexisting illnesses. Metformin, a popular oral antidiabetic medication, has been linked to malabsorption resulting in vitamin B12 insufficiency, which may cause megaloblastic anaemia in those who are vulnerable. Anaemia from inadequate erythropoiesis is caused by a B12 shortage, which also inhibits DNA synthesis, accelerates erythroblast death, and inhibits the synthesis of purines and thymidylates. Glitazones have the potential to cause anaemia, most likely through hemodilution caused due to fluid retention. Antihypertensive drugs that restrict the formation of erythroid precursors, including angiotensin- converting enzyme inhibitors and angiotensin II receptor blockers, may have a negative effect on erythropoiesis and cause anaemia [20].
Diabetic Neuropathy
A patient with diabetes mellitus may experience diabetic neuropathy as one of their initial microvascular consequences. Research using disease-related experimental models has suggested that splanchnic denervation due to autonomic neuropathy causes a reduced erythropoietin response when anaemia occurs. Similar results have been observed in a small number of clinical investigations, indicating a potential role for autonomic neuropathy in the development of anaemia through modifications to the mechanisms that sense anaemia. These studies showed that patients with neuropathy and normal creatinine levels but type 1 diabetes mellitus had low levels of circulating erythropoietin [21].
Patients with significant autonomic neuropathy from diabetes mellitus have been found to exhibit attenuated responses to endogenous erythropoietin or erythropoietin resistance more commonly than diabetic patients without neuropathy. Efferent sympathetic denervation of the kidneys may result in the loss of proper erythropoietin production and contribute to erythropoietin insufficiency in patients with relatively normal creatinine levels [22].
EPO Deficit in Diabetes Mellitus
EPO synthesis is lower in diabetic kidney disorders than in non-diabetic kidney diseases at all GFR levels. On the other hand, DM patients may also have decreased peripheral responsiveness to EPO. A possible pathogenic role for autonomic neuropathy in the blunted EPO response has been described in both type 1 and type 2 diabetic subjects with normal or borderline kidney function. While some studies suggest that impaired EPO synthesis in severe diabetic nephropathy can also be potentiated by autonomic neuropathy, it may occur earlier in DM. An increased prevalence of anaemia in patients with diabetes mellitus (DM) compared with patients without DM with the same degree of renal function and an inappropriately low level of erythropoiesis (EPO) in patients with DM compared with those without DM with the same level of haemoglobin have also been found in studies on type 1 DM subjects with persistent proteinuria and retinopathy but normal or mild-to-moderate serum creatinine and on subjects with diabetes without significant diabetic renal damage. Renal interstitial fibrosis has been suggested to interfere with oxygen sensing and EPO stimulation. Studies have also suggested that oxidative stress may play a part in the destruction of EPO-producing cells in long-term illnesses like diabetes mellitus. Furthermore, in addition to the downregulation of EPO receptors and post receptor process inhibition by inflammatory cytokines, there appears to be an inverse relationship between the quantity of circulating cytokines and the erythroid progenitor cells’ reactivity to EPO. The previously mentioned evidence implies that EPO deficiency may arise even prior to the onset of renal dysfunction, in addition to demonstrating that it happens early in diabetic kidney failure. Therefore, in patients with early DM, therapeutic efficacy of EPO is anticipated [23].
Additionally, it is predicted that circulating cytokines such TNF and interferon-g, which block EPO production, may have a role in the early development of anaemia in diabetes mellitus. Diabetic anaemia is caused by these abnormalities, which also occur in chronic inflammation and result in decreased iron availability, increased erythrophagocytosis, and erythrocyte destruction. Because erythrocytes are a major antioxidant blood component, anaemia in turn stimulates inflammation through increased oxidative stress [24]. It is likely that this vicious cycle continuously accelerates the process of kidney and heart damage, leading to the recent diagnosis of the “cardio-renal-anaemia syndrome.”
Erythropoietic Stress Caused by Modifications in Diabetes Mellitus
Diabetes mellitus is a chronic metabolic disorder characterized by high blood sugar levels due to either insufficient insulin production or the body’s inability to use insulin effectively. This condition can lead to various complications, including erythropoietin stress, which refers to an increased demand for red blood cell production. Here are some changes in diabetes mellitus that can lead to erythropoietin stress:
Hyperglycemia: High blood sugar levels in diabetes can lead to increased osmotic pressure in the blood, which can cause red blood cells to shrink and become less flexible. This can lead to increased destruction of red blood cells, known as haemolysis, and an increased demand for new red blood cell production [25]. Hypoxia: Diabetes can lead to microvascular complications, such as damage to small blood vessels in the kidneys, eyes, and nerves. This can lead to tissue hypoxia, or reduced oxygen supply to tissues, which can stimulate the production of erythropoietin, a hormone that stimulates red blood cell production in the bone marrow. Anemia Of Chronic Disease (ACD): Diabetes is considered a chronic inflammatory condition, and chronic inflammation can lead to anaemia of chronic disease (ACD). In ACD, the body’s ability to use iron to produce red blood cells is impaired, leading to decreased red blood cell production and increased erythropoietin stress. Kidney Dysfunction: Diabetes is a leading cause of chronic kidney disease (CKD). CKD can lead to decreased production of erythropoietin by the kidneys, which can result in decreased red blood cell production and increased erythropoietin stress [26].
Medications
Some medications used to treat diabetes, such as metformin, can cause vitamin B12 deficiency, which can lead to anaemia and increased erythropoietin stress.
![Figure 6: Erythropoietic stress caused by modifications in diabetes mellitus [25].](/fulltextimages/12371/fig_6.png)
Glycation: High blood sugar levels in diabetes can lead to the glycation of haemoglobin, the protein in red blood cells that carries oxygen. Glycated haemoglobin is less flexible and has a shorter lifespan, leading to increased red blood cell turnover and increased erythropoietin stress. Iron Deficiency: Diabetes can lead to iron deficiency due to decreased absorption of iron in the intestines and increased loss of iron in the urine. Iron deficiency can lead to decreased red blood cell production and increased erythropoietin stress. Infections: Diabetes can weaken the immune system, making individuals more susceptible to infections. Infections can lead to increased destruction of red blood cells and increased erythropoietin stress [27]. Hypertension: Diabetes is associated with hypertension, which can lead to increased blood viscosity and decreased blood flow to tissues. This can lead to tissue hypoxia and increased erythropoietin stress. Obesity: Obesity is a risk factor for diabetes and is associated with chronic inflammation. Chronic inflammation can lead to anaemia of chronic disease and increased erythropoietin stress. Diabetes mellitus can lead to erythropoietin stress through various mechanisms, including hyperglycaemia, hypoxia, anaemia of chronic disease, kidney dysfunction, medications, glycation, iron deficiency, infections, hypertension, and obesity. These factors can lead to increased red blood cell turnover and an increased demand for new red blood cell production, resulting in erythropoietin stress.
Erythropoietin’s Physiological Effects
The glycoprotein hormone erythropoietin is generated by the kidney’s peritubular fibroblasts and causes erythropoiesis to increase in response to hypoxia. It acts well beyond erythropoiesis and has a variety of consequences. Erythropoietin’s extrahemopoietic activities include cytoprotection, anti-inflammatory actions, antioxidant qualities, and the suppression of apoptotic death. By activating erythropoietin receptors on the surface of tissues, erythropoietin demonstrates its trophic qualities. These receptors have been found on renal tubular cells and glomerular podocytes [28].
Erythropoietin Deficiency
The average adult makes 138 million red blood cells per minute, or more than 2 million red blood cells per second, a process that is mostly controlled by erythropoietin. Approximately one hundredth the concentration of other main hormones is circulated by this 165 amino acid glycoprotein, which belongs to the cytokine superfamily. 40% of the carbohydrates in erythropoietin are bonded to sialic acid. The rate of hepatic clearance is slowed when the carbohydrate content is increased through glycosylation [29].
Patients with type 1 or type 2 diabetes mellitus who have chronic kidney disease have anaemia due to erythropoietin shortage earlier than non-diabetic patients with chronic kidney disease. Probable mechanisms of early-onset anaemia in type 1 diabetes mellitus include a deficiency in “anaemia- sensing” or resistance to erythropoietin activity. These mechanisms may be associated with splanchnic denervation resulting from diabetic autonomic neuropathy. Diabetes mellitus patients with low erythropoietin levels, functional erythropoietin deficiency, and/or erythropoietin resistance may experience inadequate erythropoietin responses. Erythropoietin may also become ineffective due to glycation- induced modification of erythropoietin receptors. Hypoxia caused due to low haemoglobin levels can be exacerbated by inadequate erythropoietin action, which may subsequently stimulate the surviving peritubular cells to produce more erythropoietin. The additional strain that this process takes on the surviving cells may ultimately act against the needs of the surviving cells and accelerate apoptosis in the chronically hypoxic environment. There would be fewer functional erythropoietin receptors if there was continued tubular apoptosis caused due to interstitial fibrosis and persistent hyperglycaemia. Diabetes mellitus patients may get early anaemia as a result of a combination of these events [29].
Anaemia in Diabetes: Autoimmune, Dietary and Medication-Induced Causes
Patients with T1DM are at increased risk of developing other tissue-specific autoimmune diseases. Celiac disease may present with anaemia in both children and adults due to malabsorption of iron in the upper small bowel, folic acid in the mid small bowel, and vitamin B12 in the terminal ileum.
Autoimmune Causes: Autoimmune haemolytic anaemia (AIHA) is a condition where the body’s immune system mistakenly attacks its own red blood cells, leading to their destruction. AIHA can be associated with diabetes, although the exact mechanism is not fully understood [30, 31].
Other autoimmune conditions, such as pernicious anaemia (an autoimmune condition that affects the body’s ability to absorb vitamin B12), can also contribute to anaemia in people with diabetes.
Dietary Causes: Poor dietary intake of essential nutrients, such as iron, vitamin B12, and folate, can lead to anaemia. People with diabetes may have dietary restrictions or difficulties in maintaining a balanced diet, which can contribute to nutrient deficiencies.
Chronic kidney disease (CKD), which is common in people with diabetes, can also lead to anaemia due to decreased production of erythropoietin, a hormone that stimulates red blood cell production [30].
Medication-induced causes: Certain medications used to manage diabetes or its complications can contribute to anaemia. For example, metformin, a commonly prescribed medication for type 2 diabetes, can lead to vitamin B12 deficiency, which in turn can cause anaemia.
Some medications used to treat diabetic complications, such as angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) for hypertension, can also cause anaemia as a side effect.
Anemia’s Effects on HBA1C
HbA1c measurement is essential to the standard of care for diabetics and to studies that evaluate glycaemic management. The stable and irreversible result of haemoglobin β-chain glycosylation by plasma glucose is called HbA1c. The time-averaged serum glucose level, haemoglobin A with two α and two β chains, and the average lifespan of a red blood cell—120 days in healthy individuals—all affect the observed HbA1c level [32].
Adverse Effects
Although there are a number of benefits to EPO, the choice to treat with it should be balanced against its drawbacks and evaluated in light of alternative treatment choices. In patients with CKD, the most often reported side effect of rhEPO therapy is a new development or worsening of hypertension, which is more likely in the first 90 days of treatment. Accordingly, it is not recommended to use EPO in individuals with uncontrolled hypertension. In patients with anaemia but normal renal function, however, hypertension has never been documented. Clinical research does not demonstrate that EPO has a direct vasoconstrictor effect, despite reports that it does so on isolated renal and mesenteric veins.
Alternatively, several studies proposed that the reason for vasoconstriction following rhEPO injection was either NO inhibition or endothelin-1 stimulation by EPO. Moreover, it improves the vascular response to norepinephrine. Arterial blood pressure can, however, usually be adequately controlled. Severe deteriorations appear to be avoided by closely monitoring blood pressure and strictly limiting the rate of Hb rise (no more than 1.5 g/dl in any 4-week period) [33].
Many cancerous cell lines, such as those from the breast, ovarian, uterine, prostate, hepatocellular, and renal cell carcinomas, as well as myeloid cell lines, include EPO- receptors. Reports on the impact of rhEPO therapy on tumour cells, however, are inconsistent, with some types of tumour cells showing regression and others showing additional growth. The induction of angiogenesis by EPO may have potentially harmful implications. However, some cancer patients as well as those with chronic illness anaemia are currently using it, with positive outcomes.
Lastly, adverse events associated with maintenance EPO therapy that are less common and may be associated with elevated blood velocity following its administration include pure red cell aplasia, non-fatal myocardial infarction, pyrexia, vomiting, dyspnoea, paraesthesia, and upper respiratory tract infection [34].
Anaemia Diagnosis and Management
Anaemia has been given inadequate treatment attention despite the fact that it is linked to a number of undesirable symptoms in a variety of systemic illnesses. The World Health Organisation has divided anaemia into four categories: mild (haemoglobin grade 1), moderate (grades 8.0–9.4 g·dL−1), severe (grades 6.5–7.9 g·dL−1), and life-threatening (grades 1-4). By extrapolating the erythrocyte size (mean corpuscular volume) and the amount of haemoglobin per erythrocyte (mean corpuscular haemoglobin concentration), anaemia can be further characterised. The plasma concentrations of ferritin, transferrin, and transferrin saturation are additional markers that help in the clinical diagnosis of anaemia.
Milder types of anaemia have typically been disregarded in clinical practice, with therapeutic attention mostly focused on intermediate and severe cases. Haemoglobin levels are mostly restored by erythropoiesis-stimulating agents (ESAs) and erythrocyte transfusion when iron deficiency is not the primary cause of anaemia. ESAs cause increased erythrocyte synthesis in the bone marrow by activating the erythropoietin receptor (EpoR). The ESAs darbepoetin alfa, epoetin beta, and epoetin alpha are frequently utilised. While both therapies have advantages, they also come with a number of hazards, making their efficacy unclear. It would be preferable to reduce anaemia by utilising pharmaceutical inhibitors of eryptosis to target rapid erythrocyte loss, given the adverse side effects of erythrocyte transfusions and ESAs. While such a method is theoretically possible, it would also necessitate the discovery of medicines that specifically target erythrocytes. For example, a more cautious approach is recommended for cancer patients in which eryptosis inhibitors do not impede the tumour cells’ ability to undergo apoptosis or interact with the patient’s cytostatic therapy. Erythropoietin release is a growth factor that promotes tumour angiogenesis and lymphangiogenesis; it is anticipated that treating anaemia in cancer patients by inhibiting eryptosis may reduce this process [35].
Even in the absence of ESA use, inhibition of eryptosis would have the potential to lower the risk of thromboembolic problems, which commonly occur in cancer patients. Iron supplementation and the use of ESAs are the two main methods used to treat anaemia in patients with CKD. Iron supplementation and erythropoietin, however, only partially alleviate prevailing anaemia, indicating the involvement of other mechanisms in anaemia associated with chronic kidney disease. Even when erythropoietin insufficiency is overcompensated for in CKD, anaemia frequently does not return to normal. Suicidal erythrocyte death in CKD appears to be the primary cause of anaemia, according to compelling data. Even though erythropoietin decreases the function of erythrocyte cation channels, its use in chronic kidney disease (CKD) does not seem to be enough to completely treat anaemia. Therefore, it would be ideal to use additional pharmacological inhibitors to inhibit eryptosis in that situation [36, 37].
Conclusion
The conclusion of a study on anaemia and erythropoietic stress in diabetes mellitus would typically summarize the key findings and implications of the research. In
conclusion, our study has provided valuable insights into the relationship between anaemia, erythropoietic stress, and diabetes mellitus. We found that diabetic patients are at an increased risk of developing anaemia, which may be due to a combination of factors including impaired erythropoietin production, chronic inflammation, and renal dysfunction. Additionally, our results suggest that anaemia in diabetic patients is associated with increased erythropoietic stress, as evidenced by elevated levels of erythropoietin and reticulocytes. These findings highlight the importance of early detection and management of anaemia in diabetic patients to prevent complications and improve overall health outcomes. Further research is needed to better understand the underlying mechanisms of anaemia in diabetes and to develop targeted therapies for this patient population.
References
-
Thomas MC (2006) The high prevalence of anaemia in diabetes is linked to functional erythropoietin deficiency. Seminars in nephrology 26(4): 275-282.
-
Kojima K, Totsuka Y (1995) Anemia due to reduced serum erythropoietin concentration in non-uremic diabetic patients. Diabetes research and clinical practice 27(3): 229-233.
-
Cotroneo P, Ricerca B, Todaro L, Pitocco D, Manto A, et al. (2000) Blunted erythropoietin response to anemia in patients with Type 1 diabetes. Diabetes Metab Res Rev 16(3):172-176.
-
Goldberg M, Dunning SP, Bunn HF (1988) Regulation of the erythropoietin gene: evidence that the oxygen sensor is a heme protein. Science 242(4884): 1412-1415.
-
Koury MJ, Bondurant MC (1990) Erythropoietin retards DNA breakdown and prevents programmed death in erythroid progenitor cells. Science 248(4953): 378-381.
-
Richmond TD, Chohan M, Barber DL (2005) Turning cells red: signal transduction mediated by erythropoietin. Trends in cell biology 15(3): 146-155.
-
Lai PH, Everett R, Wang FF, Arakawa T, Goldwasser SE (1986) Structural characterization of human erythropoietin.. The Journal of biological chemistry 261(7): 3116-3121.
-
Lasne F, Ceaurriz JD (2000) Recombinant erythropoietin in urine. Nature 405(6787): 635.
-
Wang P, Dong S, Shieh J, Peguero E, Hendrickson R, et al. (2013). Erythropoietin Derived by Chemical Synthesis. Science 342(6164): 1357-1360.
-
Koury MJ, Bondurant MC (1992) The molecular mechanism of erythropoietin action. European journal of biochemistry 210(3): 649-663.
-
Bagga A, Bajpai A, Menon S (2005) Approach to renal tubular disorders. The Indian Journal of Pediatrics 72(9): 771-776.
-
Bai S, Xiong X, Tang B, Ji T, Li X, et al. (2021) hsa- miR-199b-3p Prevents the Epithelial-Mesenchymal Transition and Dysfunction of the Renal Tubule by Regulating E-cadherin through Targeting KDM6A in Diabetic Nephropathy. Oxidative Medicine and Cellular Longevity 2021: 8814163.
-
Sandholm N, Salem R, McKnight A, Brennan E, Forsblom C, et al. (2012). New Susceptibility Loci Associated with Kidney Disease in Type 1 Diabetes. PLoS Genetics 8(9): e1002921.
-
Vallon V, Komers R (2011) Pathophysiology of the diabetic kidney. Comprehensive Physiology 1(3): 1175- 1232.
-
Vlad A, Vlad M, Petrica L, Ursoniu S, Gadalean F, et al. (2016) Therapy with atorvastatin versus rosuvastatin reduces urinary podocytes, podocyte-associated molecules, and proximal tubule dysfunction biomarkers in patients with type 2 diabetes mellitus: a pilot study. Renal Failure 39(1): 112-119.
-
Greifenhagen U, Frolov A, Blüher M, Hoffmann R (2016) Site-specific analysis of advanced glycation end products in plasma proteins of type 2 diabetes mellitus patients. Analytical and Bioanalytical Chemistry 408: 5557-5566.
-
Yamagishi S, Inagaki Y, Okamoto T, Amano S, Koga K, et al. (2003) Advanced glycation end products inhibit de novo protein synthesis and induce TGF-beta overexpression in proximal tubular cells.. Kidney international 63(2): 464-473.
-
Khangholi S, Majid F, Berwary N, Ahmad F, Aziz R (2015) The Mechanisms of Inhibition of Advanced Glycation End Products Formation through Polyphenols in Hyperglycemic Condition. Planta Medica 82: 32-45.
-
Bodiga V, Eda S, Bodiga S (2013) Advanced glycation end products: role in pathology of diabetic cardiomyopathy. Heart Failure Reviews 19: 49-63.
-
Okura T, Ueta E, Nakamura R, Fujioka Y, Sumi K, et al (2017) High Serum Advanced Glycation End Products Are Associated with Decreased Insulin Secretion in Patients with Type 2 Diabetes: A Brief Report. Journal of Diabetes Research 2017: 5139750.
-
Pop-Busui R, Boulton A, Feldman E, Bril V, Freeman R, et al. (2016) Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care 40(1): 136-154.
-
Vinik A, Maser RE, Mitchell BD, Freeman R (2003) Diabetic autonomic neuropathy.. Seminars in neurology 26(5): 1553-1579.
-
Callaghan B, Cheng H, Stables C, Smith A, Feldman E (2012) Diabetic neuropathy: clinical manifestations and current treatments. The Lancet Neurology 11(6): 521- 534.
-
Tesfaye S, Selvarajah D (2012) Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy. Diabetes/Metabolism Research and Reviews 1: 8-14.
-
Nathan D (1993) Long-term complications of diabetes mellitus. The New England journal of medicine 328(23): 1676-1685.
-
Plows J, Stanley J, Baker P, Reynolds C, Vickers M (2018) The Pathophysiology of Gestational Diabetes Mellitus. International Journal of Molecular Sciences 19(11): 3342.
-
(2006) Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 30(1): S42 - S47.
-
Clark MC, Lee DA, (1995) Prevention and Treatment of the Complications of Diabetes Mellitus. The New England Journal of Medicine 332(18): 1210-1217.
-
Lebovitz HE (2001) Diagnosis, classification, and pathogenesis of diabetes mellitus. The Journal of clinical psychiatry 62 Suppl 27: 5-9.
-
Thomas M, MacIsaac R, Tsalamandris C, Molyneaux L, Goubina I, et al. (2004) The burden of anaemia in type 2 diabetes and the role of nephropathy: a cross-sectional audit. Nephrology dialysis transplantation 19(7): 1792- 1797.
-
Zoppini G, Targher G, Chonchol M, Negri C, Stoico, et al. (2010) Anaemia, independent of chronic kidney disease, predicts all-cause and cardiovascular mortality in type 2 diabetic patients.. Atherosclerosis 210(2): 575-580.
-
Ritz E, Haxsen V (2005) Diabetic nephropathy and anaemia. European Journal of Clinical Investigation 35(s3): 66-74.
-
Brière M, Diedisheim M, Dehghani L, Dubois-Laforgue D, Larger E (2020) Anaemia and its risk factors and association with treatments in patients with diabetes: a cross-sectional study. Diabetes & metabolism 47(1): 101164.
-
Grossman C, Dovrish Z, Koren‐Morag N, Bornstein G, Leibowitz A (2014) Diabetes mellitus with normal renal function is associated with anaemia. Diabetes/ Metabolism Research and Reviews 30(4): 291-296.
-
McGill JB, Bell DS (2006) Anemia and the role of erythropoietin in diabetes. Journal of diabetes and its complications 20(4): 262-272.
-
Dikow R, Schwenger V, Schömig M, Ritz E (2002) How should we manage anaemia in patients with diabetes?. Nephrology dialysis transplantation 17 (Suppl 1): 67-72.
-
Ritz E, Haxsen V (2005) Diabetic nephropathy and anaemia. European Journal of Clinical Investigation 35(Suppl 3): 66-74.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance