Interplay Between Metabolic Syndrome and Gastrointestinal Disorders: Pathophysiology and Clinical Implications
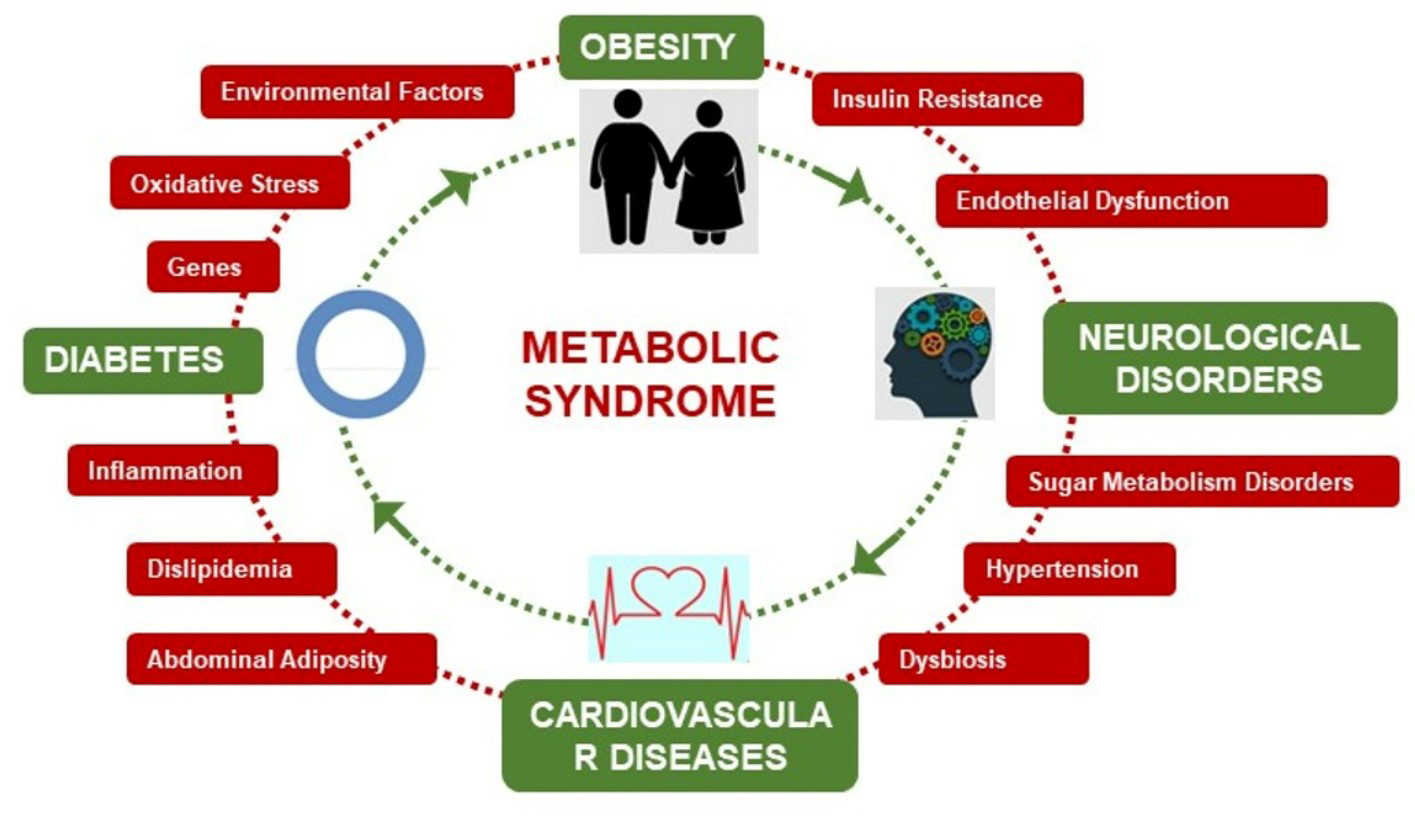
The term "metabolic syndrome" refers to a collection of metabolic disorders, the most common of which is obesity, particularly abdominal obesity. Many chronic diseases, including cardiovascular disease, have metabolic syndrome as a risk factor. Furthermore, the rise in obesity-related disorders linked to a poor lifestyle that include dyslipidaemia, hypertension, and irregularities in glucose metabolism—a condition known as metabolic syndrome (MS)—has been problematic. In addition to being linked to digestive system issues, such as upper gastrointestinal diseases, MS has also been found to be a risk factor for arteriosclerotic diseases and ischemic heart disease. Multiple gastrointestinal disorders, including colorectal cancer and gastroesophageal reflux disease, have been associated with obesity. Obesity as manifested by an elevated body mass index is not as significant as abdominal obesity as a contributing factor to the development of these diseases, according to recent research. Apart from the physiological consequences of obesity, such as elevated intra-abdominal pressure due to substantial adipose tissue, substances secreted by adipose tissue, including insulin-like growth factor-1, interleukin-6, leptin, and tumour necrosis factor-α, have been suggested as pathogenic mediators of these disorders. Unlike high body weight and high body mass index, visceral fat accumulation associated with abdominal obesity is linked to the onset of several diseases of the digestive system because it can raise intra-abdominal pressure, which triggers the release of several bioactive substances known as adipocytokines, such as tumour necrosis factor-a, interleukin-6, resistin, leptin, and adiponectin. This review article focuses on obesity, visceral fat build-up, and the main upper gastrointestinal ailments, as well as their correlation with multiple sclerosis. Within this review, we discuss the relationship between digestive disorders and metabolic syndrome or its component parts, with a particular emphasis on obesity and abdominal obesity.
Key Insights
- Abdominal obesity is a more significant risk factor for gastrointestinal diseases than general obesity, with adipose tissue secretions like tumor necrosis factor- alpha and interleukin-6 playing pathogenic roles.
- Gut dysbiosis contributes to the pathogenesis of both gastrointestinal disorders and metabolic syndrome, with bioactive dietary components such as fibers and polyphenols potentially serving as alternative treatments by restoring normal intestinal flora.
- The gastrointestinal tract is integral to metabolic syndrome, with bariatric surgery being an effective treatment for obesity-related type 2 diabetes due to changes in gut hormones and microbiota.
- Traditional Chinese medicine may treat metabolic syndrome-related diseases like diabetes and NAFLD by influencing the composition and metabolism of intestinal microorganisms.
- Metabolic syndrome components, particularly abdominal obesity and insulin resistance, are implicated in the development of colorectal cancer.
- NAFLD, the major hepatic disorder in metabolic syndrome patients, is influenced by insulin resistance, abnormal lipid metabolism, and dysregulation of cytokines/adipokines.
- The gut microbiome has a substantial influence on metabolic syndrome risk factors, with a defective gut barrier and microbially produced metabolites affecting host metabolism.
- Metabolic and bariatric surgeries address the metabolic syndrome by altering neurohormonal mechanisms, which can lead to the resolution of clinical and biochemical manifestations.
- Metabolic syndrome is associated with an increased risk of gastrointestinal cancers, with central obesity being a core driver of this risk.
- Metabolic syndrome and inflammatory bowel disease share pathophysiological features such as adipose tissue dysregulation and chronic inflammation, suggesting potential common therapeutic targets.
Abbreviations
MS: Metabolic Syndrome; HDL: High-Density Lipoprotein; ATP: Adult Treatment Panel; IDF: International Diabetes Federation; WHR: Waist-to-hip Ratio; NSAIDs: Non-Steroidal Anti-Inflammatory Drugs; GERD: Gastroesophageal Reflux Disease; BE: Barrett’s Oesophagus; LES: Lower Oesophageal Sphincter.
Introduction
The term metabolic syndrome (MS) refers to the build-up of visceral fat together with disorders linked to a certain lifestyle that include dyslipidaemia, hypertension, and irregularities in glucose metabolism [1]. A cluster of metabolic abnormalities, metabolic syndrome is defined as having three or more of the following characteristics: high blood pressure, low high-density lipoprotein (HDL) cholesterol, elevated triglycerides, elevated abdominal obesity (increased waist circumference [WC), and high fasting glucose.
Cardiovascular and other chronic disease are at risk due to metabolic syndrome. Worldwide use has been made of the MS diagnostic criteria that the Adult Treatment Panel (ATP) III and the International Diabetes Federation (IDF) accepted, although Japan frequently uses the MS criteria that a joint committee of eight Japanese medical societies established in 2005.The metabolic syndrome is receiving more and more attention, and the most clinically significant obesity pattern has been considered to be abdominal obesity, particularly visceral obesity (i.e., the build-up of intra-abdominal fat). Waist-to-hip ratio (WHR) and waist circumference (WC) are sensitive indicators of visceral obesity. While numerous research has examined the connection between obesity and various gastrointestinal disorders, there is a dearth of information regarding the potential risk factors for gastrointestinal disorders associated with metabolic syndrome or abdominal obesity [2]. We examine the relationship between gastrointestinal disorders and the metabolic syndrome, or its component parts, with a particular emphasis on obesity and abdominal obesity. Recent lifestyle changes, such as increased fat intake and decreased activity, have contributed to a rise in MS cases that has been problematic in both developed and developing nations. Insulin resistance is associated with a number of pathophysiological disorders, including altered adipocytokine production from visceral fat in MS patients. Multiple sclerosis (MS) has a significant influence on public health and medical costs since it can cause a variety of disorders, including ischemic heart disease and abnormalities of the digestive system, including upper gastrointestinal diseases. Aspirin, ibuprofen, and diclofenac are examples of non-steroidal anti-inflammatory drugs (NSAIDs); genetic predisposition to the disease; pharmaceutical therapies (i.e., antibiotics, not limited to those administered for human use but potentially including those used in farm animals and crops and ingested with the resultant foods); and unhealthy lifestyles (i.e., irregular eating, physical inactivity, smoking, and low fibre diets) are the main causes of gastrointestinal disorders [3, 4, 5]. Furthermore, Helicobacter pylori, a Gram- negative bacterial infection that may cause IBD and functional gastrointestinal diseases, affects roughly 50% of the world’s population. Abdominal pain, constipation, diarrhoea, abdominal distention, stomach acidity, gastrointestinal reflux disease (GERD), bleeding in the GI tract, malnourishment or malabsorption, and intestinal blockage are frequent symptoms of all GI illnesses [6, 7]. Currently, laxatives, anti-diarrheal, opioids, anti-emetics, motility enhancers, anti-acidity, anti-ulcer, and anti-inflammatory agents are some of the medications used to treat GI issues. Traditional treatments for inflammatory bowel disease (IBD) use corticosteroids, immunosuppressant’s, and anti-tumor necrosis factor (TNF)-α antibodies. These treatments are frequently associated with an increased risk of opportunistic infections and dysplasia’s, which can have costly effects on the management of the health system [8, 9]. Research points to the Western pattern diet (WPD) as the cause of the widespread occurrence of GERD. According to studies, GERD is more common in North America (18.1–27.8%), Europe
(8.8–25.9%), Australia (11.6%), South America (23%), East Asia (2.5–7.8%), and the Middle East (8.7–33.1%). Though the prevalence of dyspepsia varies from nation to nation, Ford et al. indicate a 21% pooled prevalence [10, 11]. Diarrhoea causes more than 128,000 hospital admissions and 3000 fatalities in the adult population in the United States. Likewise, extant research indicates that 12% of the global populace has experienced constipation.
The etiopathogenesis of GI illnesses remains unclear, and there is currently no marker that can definitively diagnose them, despite recent advancements in our understanding of the pathophysiological pathways involved [12, 13]. Several known etiological variables include infections, genetic and epigenetic modifications, stress, gut microbiota alterations that result in dysbiosis, and visceral hypersensitivity.
When discussing the function of insulin resistance in human disease, Reaven (1988) emphasised the clinical significance of multiple sclerosis [14, 15]. Numerous metabolic disorders, such as gout, hypertension, and hyperglycaemia, were already documented in the 1920s, according to Sadeghi. Later, in 1947, Vague identified metabolic problems, cardiovascular disease, and type 2 diabetic mellitus (T2DM) as factors influencing the obese phenotype. Insulin resistance and glucose intolerance are recognised as critical elements of multiple sclerosis (MS) in both the European Group for the Study of Insulin Resistance and the WHO classification. The past 20 years have seen a significant rise in the global MS population, which has been linked to an epidemic of obesity and type 2 diabetes [16, 17, 18]. Approximately 20–25% of adults worldwide have multiple sclerosis. According to WHO estimates, 422 million people have diabetes, 1.13 billion have hypertension, and 650 million have obesity. These days, it is understood that nutrition and lifestyle choices are essential to preventing diseases including MS, T2DM, cardiovascular disease, and gastrointestinal issues [19, 20]. Moreover, the most recent research indicates that the balance of gut microbiota is restored by modulating intestinal dysbiosis with dietary supplements. The goal of this review is to provide an overview of the current understanding of the protective roles of functional dietary components in both GI and MS, taking into account that dysbiosis may be a common link between GI disorders and MS and that the restoration of altered microbiota through diet is thought to be the first line of treatment for both conditions [21, 22].
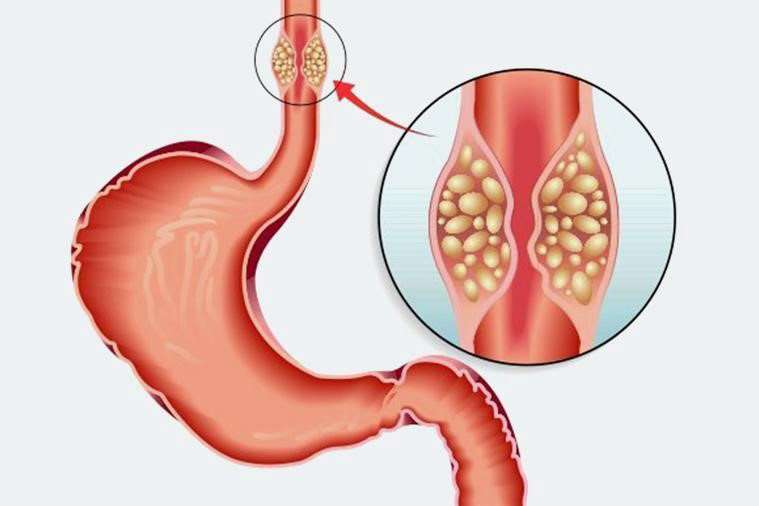
Hiatal Hernias
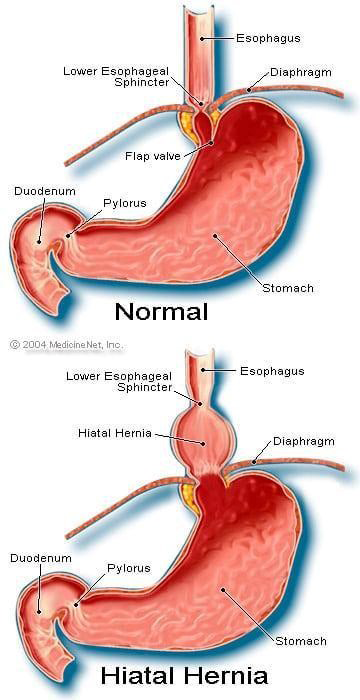
Hiatal hernias are a common condition that can mimic other diseases and have significant implications for upper gastrointestinal health. They are particularly relevant in the context of gastroesophageal reflux disease (GERD) and can be associated with other conditions such as metabolic syndrome [23]. Hiatal hernias can mimic symptoms of cardiovascular and gastrointestinal diseases, leading to substernal and upper abdominal complaints, and are often associated with conditions like angina pectoris and peptic ulcer. The size of a hiatal hernia is directly related to the severity of lower oesophageal sphincter (LES) dysfunction, oesophageal acid exposure, and mucosal injury in GERD patients [24]. Larger hernias result in weaker LES, increased acid reflux, and more severe esophagitis. Hiatal hernias can have clinical implications beyond GERD, such as in patients with right isomerism, where they are associated with symptoms like vomiting and recurrent airway infections, and may have a potential link to sudden death [25].
Cameron ulcers, which are linear gastric ulcers found in large hiatal hernias, can cause severe upper gastrointestinal haemorrhage. Treatment options for Cameron ulcers include high-dose proton pump inhibitors or surgery, depending on individual patient circumstances [26].
In conclusion, hiatal hernias play a significant role in upper gastrointestinal diseases, affecting LES function and contributing to conditions like GERD and Cameron ulcers. The size of the hernia is a critical factor in the severity of associated symptoms and mucosal damage [27]. Additionally, hiatal hernias can have broader clinical implications, particularly in patients with specific anatomical anomalies such as right isomerism. Treatment approaches vary and should be tailored to the individual patient’s needs [28].
Gastroesophageal Reflux Disease
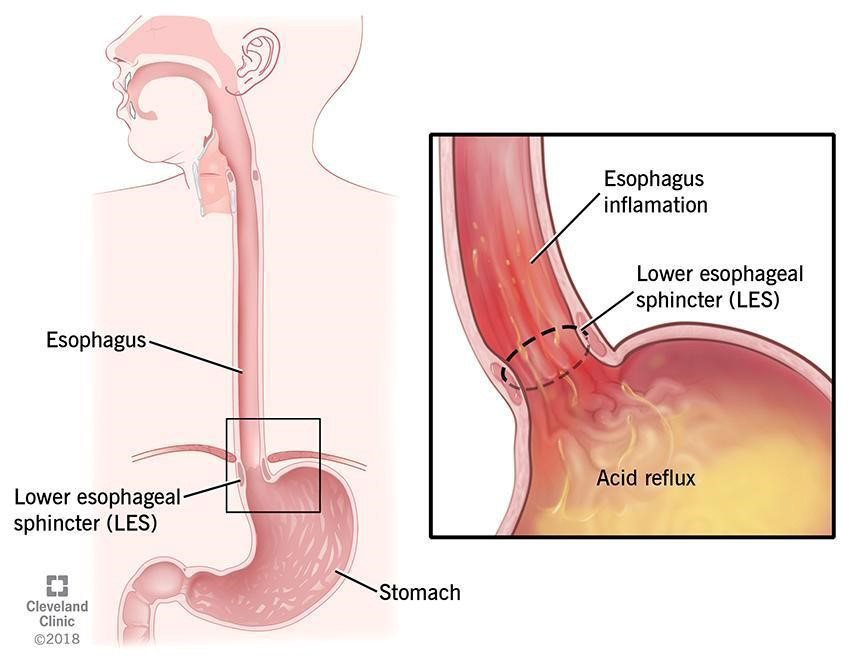
Gastroesophageal reflux disease (GERD) is a prevalent condition that negatively impacts the quality of life and has been increasingly associated with metabolic syndrome (MS). The relationship between MS and GERD, including its complications such as Barrett’s oesophagus (BE), has been the subject of various studies, revealing a complex interplay between these conditions [29].
Metabolic syndrome is significantly associated with a higher prevalence of GERD, as evidenced by systematic reviews and cross-sectional studies, suggesting MS as an independent risk factor for GERD [30]. The presence of MS components, particularly central obesity and abnormal fasting glucose levels, has been independently linked to GERD, indicating that central obesity may play a more critical role than BMI alone in this association [31]. Metabolic syndrome has been identified as a risk factor for the development of Barrett’s oesophagus, independent of reflux symptoms, suggesting a potential reflux-independent pathway in the pathogenesis of BE [32].
Studies have shown that metabolic syndrome is associated with both erosive esophagitis and Barrett’s oesophagus, with a greater risk of concurrent MS in patients with these conditions [33]. There is no significant difference in the prevalence of central obesity and metabolic syndrome between patients with Barrett’s oesophagus and those with GERD, indicating that these factors may not directly influence the development of BE in a reflux population [34]. Decreased levels of adiponectin in obese patients with GERD have been observed, which may indicate a relationship between GERD and metabolic syndrome.
The synthesis of the research indicates a strong association between metabolic syndrome and gastroesophageal reflux disease [35]. Metabolic syndrome, particularly factors like central obesity and abnormal glucose levels, appears to be an independent risk factor for GERD and its complications, including Barrett’s oesophagus [36]. This relationship suggests that the management of metabolic syndrome may play a role in the treatment and prevention of GERD and its progression [37].
Barrett’s Oesophagus
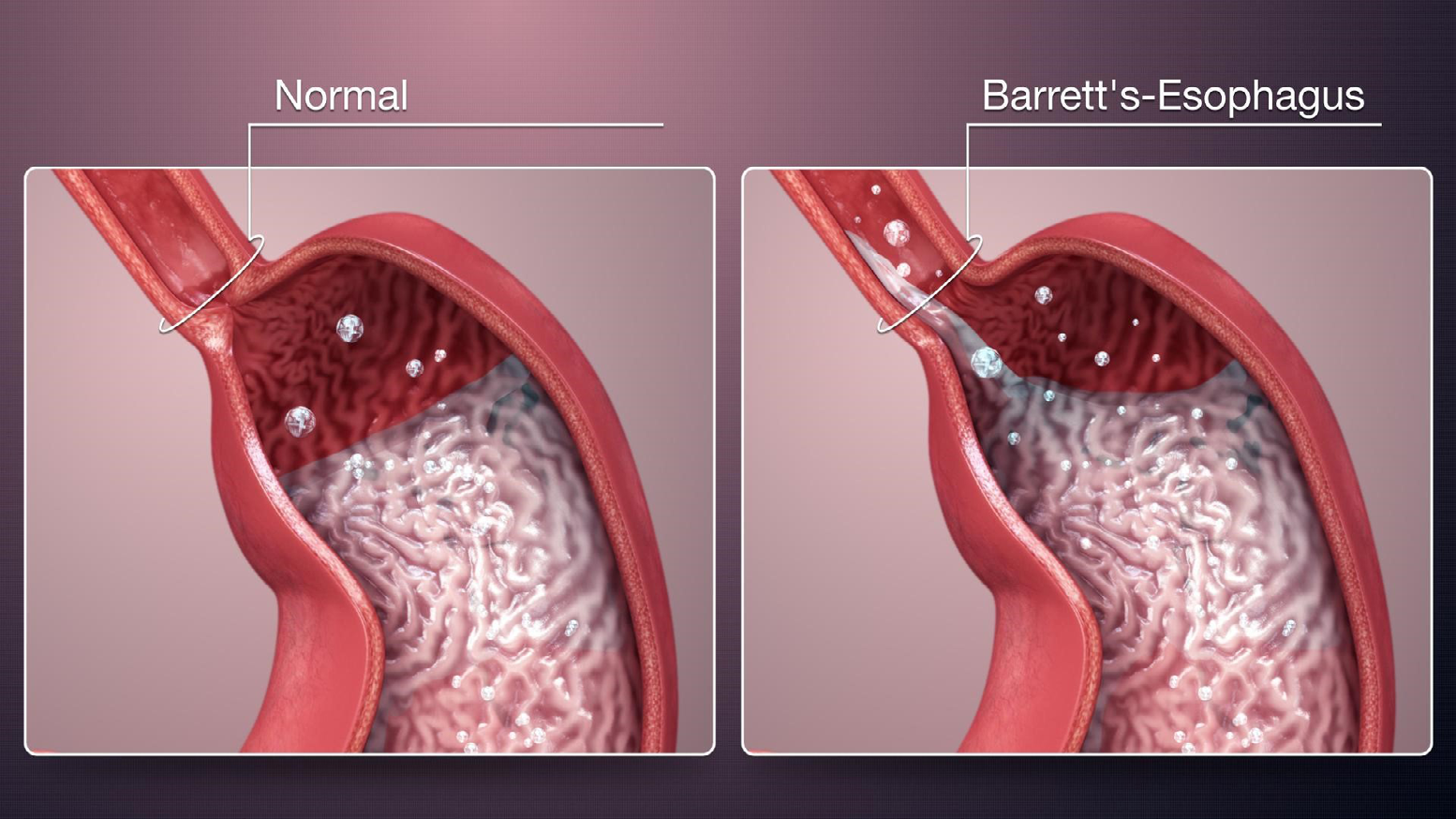
Barrett’s oesophagus (BE) is a condition that can arise as a complication of gastroesophageal reflux disease (GERD), and it is characterized by the replacement of the normal squamous epithelium of the oesophagus with columnar epithelium. Metabolic syndrome is associated with an increased risk of Barrett’s oesophagus, particularly in patients without symptomatic reflux, suggesting a potential GERD-independent inflammatory pathway for BE pathogenesis [38].
Central obesity and metabolic syndrome are prevalent in patients with Barrett’s oesophagus, with a significant association between the length of specialized intestinal metaplasia and the presence of metabolic syndrome. The prevalence of metabolic syndrome in patients with Barrett’s oesophagus exceeds population norms, and metabolic syndrome is associated with elevated levels of proinflammatory markers such as C-reactive protein and interleukin-6 [39]. There is no significant difference in the prevalence of central obesity and metabolic syndrome between Barrett’s oesophagus and gastroesophageal reflux disease patients, indicating that these factors may not impact the development of BE in a reflux population.
Metabolic syndrome is associated with Barrett’s oesophagus independent of other risk factors such as smoking, alcohol consumption, and body mass index, and this association remains robust in various analyses. The systemic inflammatory state induced by metabolic syndrome may represent a reflux-independent inflammatory pathway that increases the risk of Barrett’s oesophagus, but it does not appear to increase the risk of oesophageal adenocarcinoma in the studied population [40].
The research indicates a strong association between metabolic syndrome and the risk of developing Barrett’s oesophagus, especially in the absence of gastroesophageal reflux symptoms. Central obesity and metabolic syndrome are common in BE patients and are linked to a proinflammatory state [41]. However, the presence of metabolic syndrome does not significantly differ between BE and GERD patients, suggesting that while MS may contribute to the risk of BE, it does not necessarily differentiate between BE and GERD in terms of disease progression. The findings underscore the importance of considering metabolic syndrome as a potential independent risk factor for Barrett’s oesophagus, separate from the effects of gastroesophageal reflux [42].
Esophageal Adenocarcinoma
Oesophageal adenocarcinoma (EA) is a type of cancer that arises from the oesophagus, often associated with Barrett’s oesophagus and influenced by various risk factors, including metabolic syndrome (MS).
Adenocarcinomas of the oesophagus and stomach show differential activity in functional modules related to inflammation and lipid metabolism, with lipid metabolism being active in intestinal metaplasia and inactive in adenocarcinomas [43]. A significant proportion of patients with Barrett’s oesophagus exhibit metabolic syndrome and central adiposity, with a higher prevalence in those with longer segments of specialized intestinal metaplasia. Metabolic syndrome is associated with an increased risk of gastric adenocarcinoma, particularly in women, with high waist circumference also associated with an increased risk of oesophageal adenocarcinoma [44]. Metabolic syndrome may represent a GERD-independent inflammatory pathway that increases the risk of Barrett’s oesophagus but does not appear to increase the risk of oesophageal adenocarcinoma The incidence of oesophageal adenocarcinoma has been rising, with known risk factors including GERD, obesity, and tobacco smoking, but the role of metabolic syndrome requires further investigation [45]. There is no significant difference in the prevalence of central adiposity and metabolic syndrome between patients with Barrett’s oesophagus and those with GERD, suggesting that these factors may not independently affect the development of Barrett’s oesophagus in a reflux population.
The research indicates a complex relationship between metabolic syndrome, Barrett’s oesophagus, and oesophageal adenocarcinoma. Metabolic syndrome is linked to an increased risk of Barrett’s oesophagus, particularly in the absence of GERD, and may contribute to the progression of gastrointestinal diseases through inflammation and altered lipid metabolism [46]. While central adiposity and metabolic syndrome are common in both Barrett’s oesophagus and GERD, their direct impact on the development of oesophageal adenocarcinoma remains unclear, necessitating further research to understand the mechanisms and potential interventions [47].
Gastric Adenocarcinoma
Gastric adenocarcinoma, a prevalent form of stomach cancer, has been increasingly studied in relation to metabolic syndrome, a cluster of conditions including increased waist circumference, elevated triglycerides, reduced high-density lipoprotein cholesterol, hypertension, and high glucose levels. This interest stems from the potential influence of metabolic disorders on the development and progression of gastrointestinal diseases [48]. Metabolic syndrome is significantly associated with an increased risk of gastric adenocarcinoma, particularly in women, with high waist circumference, hypertension, and high non-fasting glucose levels being notable risk factors. The presence of metabolic syndrome prior to surgery predicts a higher mortality rate for gastric cancer patient’s post-gastrectomy, with hyperglycaemia being a critical factor, especially in the early stages of gastric cancer [49].
Gastric adenocarcinoma can manifest as part of a familial syndrome known as GAPPS, characterized by fundic gland polyps and a high risk of cancer confined to the proximal stomach, without association with colorectal or duodenal polyposis [50]. Metabolic syndrome components, such as higher triglyceride levels, lower HDL-C levels, and hypertension, are more prevalent in gastric cancer patients, suggesting a role in cancer development and progression, particularly in poorly differentiated and advanced-stage cancers. In contrast to gastric adenocarcinoma, metabolic syndrome does not show a significant association with oesophageal adenocarcinoma or oesophageal squamous-cell carcinoma. Abdominal obesity, rather than overall obesity, is emphasized as a more critical factor for the development of gastrointestinal diseases, including gastric adenocarcinoma.
The research indicates a strong link between metabolic syndrome and the risk of developing gastric adenocarcinoma, with specific components of the syndrome such as abdominal obesity, hypertension, and hyperglycaemia being particularly influential [51]. This association is more pronounced in women and can significantly affect mortality rates following surgical treatment for gastric cancer. Additionally, certain familial syndromes highlight the genetic predisposition to gastric adenocarcinoma, emphasizing the need for awareness and screening in affected families [52]. While metabolic syndrome is a clear risk factor for gastric adenocarcinoma, its role in other gastrointestinal cancers, such as oesophageal cancer, is less evident. Overall, these findings underscore the importance of managing metabolic disorders to potentially reduce the risk and improve outcomes for gastric adenocarcinoma patients [53].
Obesity and GI Disorders Insulin Resistance and GI Disorders Dyslipidaemia and GI Disorders Hypertension and GI Disorders Hyperglycaemia and GI Disorders Gastroesophageal Reflux Disease (GERD): Obesity increases the pressure in the abdominal cavity, which can lead to the development of GERD. Excess body fat, especially around the abdomen, can push the stomach upward and cause acid to reflux into the oesophagus.
Gallstones: High levels of triglycerides and low levels of high- density lipoprotein (HDL) cholesterol are associated with an increased risk of gallstones. Gallstones can block the bile ducts, causing pain, infection, and jaundice.
NAFLD: Insulin resistance is closely linked to the development of NAFLD. It promotes the accumulation of fat in the liver and contributes to inflammation and fibrosis.
Pancreatitis: Insulin resistance and hyperglycaemia can lead to pancreatitis, an inflammation of the pancreas. Chronic pancreatitis can result in exocrine pancreatic insufficiency, where the pancreas cannot produce enough digestive enzymes.
Non-alcoholic Fatty Liver Disease (NAFLD): Obesity is a major risk factor for NAFLD, a condition where fat accumulates in the liver in the absence of significant alcohol consumption. This can progress to non- alcoholic steatohepatitis (NASH), cirrhosis, and liver cancer.
Atherosclerosis: Dyslipidaemia contributes to atherosclerosis, which can affect blood vessels supplying the GI tract, potentially leading to ischemic bowel disease.
Gastroparesis: Chronic high blood sugar levels can damage the nerves that control the stomach muscles, leading to gastroparesis. This condition slows or stops the movement of food from the stomach to the small intestine.
Ischemic Colitis: Hypertension can contribute to ischemic colitis, where reduced blood flow to the colon causes inflammation and injury.
Portal Hypertension: High blood pressure can also lead to portal hypertension, which is high blood pressure in the portal vein that supplies the liver. This can result in complications such as varices (enlarged veins) in the oesophagus and stomach, which can bleed.
Diabetic Enteropathy: Hyperglycaemia can also affect the small and large intestines, leading to symptoms like diarrhoea, constipation, and abdominal pain.

Gastroesophageal Reflux Disease, Barrett’s Esophagus and Esophageal Adenocarcinom
In the United States and the Western world, obesity and gastroesophageal reflux disease (GERD) are two of the most prevalent conditions, and their rates have been rising sharply.
Recent research indicates that 20% of Americans may have GERD [54]. In the US population, the prevalence of obesity (body mass index (BMI) ≥ 30 kg/m2) is 30.5%. Increases in GERD symptoms are connected with higher BMIs, and a correlation has been documented between GERD symptoms and obesity [55, 56]. A BMI > 30 kg/m2 was found to be one risk factor [odds ratio (OR) 2.8; 95% confidence interval (CI), 1.7–4.5, compared with normal weight, which is defined as BMI ≤ 24 kg/m2] in a cross-sectional population-based study conducted in the United States by Lock et al. [57] to assess risk factors for the development of GERD symptoms. A cross-sectional population-based study conducted in the UK revealed an effective and positive correlation between BMI and the frequency of GERD symptoms.
In comparison to people of normal weight, the odds ratios (ORs) for the frequency of acid regurgitation and heartburn in obese individuals were 2.91 (95% CI, 2.07–4.08) and 2.23 (95% CI, 1.44–3.45), respectively. Additionally, a population- based study conducted in Germany found a substantial correlation between GERD symptoms and being overweight or obese [58]. However, a population-based study conducted in Sweden discovered that there was no correlation between reflux symptoms and BMI, and that the OR of recurrent GERD symptoms in adults who had ever been obese or overweight (BMI ≥ 25 kg/m2) compared to those who had never been obese or overweight was 0.99 (95% CI, 0.66–1.47) [59]. Exams with an esophagogastroduodenoscopy are not typically conducted in cross-sectional population-based investigations. Consequently, those suffering from Barrett’s oesophagus (BE), oesophageal adenocarcinoma (EAC), GERD (both nonerosive and erosive), or other medical conditions are all included.
The range of diagnosis could have an impact on the outcomes. The mean BMI is substantially greater in patients with erosive GERD than in those with nonerosive GERD in studies where endoscopic examinations were conducted in patients exhibiting symptoms of GERD [60, 61]. According to research by Van Oijen et al., [62] there is a tendency for obesity to be linked to both erosive GERD and GERD symptoms when examining the relationship between BMI and GERD symptoms in a group referred for upper gastrointestinal endoscopy [63]. El-Serag, et al. [64] investigated if the correlation between obesity and GERD symptoms remained after controlling for other established risk factors for GERD, such as age, sex, race, and smoking. Weekly heartburn or regurgitation was associated with to a BMI > 30 kg/m2 (adjusted OR, 2.44; 95% CI, 1.27–4.67) as in contrast to a BMI < 25 kg/m2. Obesity and overweight (body mass index, 25–30 kg/m2) were both significant independent risk factors for erosive GERD. However, Lundell, et al. [65] found no correlation between abnormal acid reflux or erosive GERD and being significantly overweight (BMI, 42.5 ± 5.2 kg/m2).
There is a sex difference in the relationship between GERD symptoms and obesity, according to [66] Nilsson et al. Higher BMI was positively associated with GERD symptoms in both sexes, but the correlation was larger in female patients. In addition, there was a difference in the strength of the connection between premenopausal and postmenopausal women. Both being overweight (BMI, 25–30 kg/m2) and obese (BMI > 30 kg/m2) were related to a statistically significant increase in the risk for GERD symptoms, with ORs of 1.43 (95% CI, 1.158–1.774) and 1.94 (95% CI, 1.468–2.566), respectively, in a recent meta-analysis [67] of published data on the association between obesity and GERD. Additionally, being overweight or obese was a risk factor for erosive GERD (OR, 1.76; 95% CI, 1.156–2.677). Both of these findings were associated to a statistically significant increase in the risk for GERD symptoms.
Empirical observations suggest that losing weight can help lessen GERD symptoms. The results of Nilsson et al. support the theory that if there is a direct correlation between obesity and GERD, weight change should affect GERD symptoms or the severity of erosive GERD. They demonstrated that, in comparison to people with stable BMI, the risk of reflux symptoms was higher (OR, 2.7; 95% CI, 2.3–3.2) in those who gained more than 3.5 BMI units, but the risk of GERD symptoms was lower (OR, 0.6; 95% CI, 0.4–0.9) in those who lost more than 3.5 BMI units. On the other hand, there is inconsistent data about the relationship between weight loss and improved GERD symptoms [68, 69]; certain reports indicate a reduction in GERD symptoms, while others do not.
The contradictory findings could be explained by either irreversible abnormality at the esophagogastric junction, like a hiatal hernia, or by the weight loss being insufficient to produce an improvement after the increase in BMI [70].
The evaluation of the correlation between GERD and BMI entails a number of confounding variables. Although several statistics point to an increased incidence of GERD in overweight or obese patients, the link between obesity and GERD is still unclear. It was recently revealed that WC and BMI were related to the same level of oesophageal acid exposure. A BMI ≥ 30 kg/m2 was no longer substantially correlated with any indicators of oesophageal acid exposure after controlling for WC. Consequently, obesity as indicated by an elevated BMI may not be the primary cause of GERD symptoms [71] than abdominal obesity. To test this theory, more research is required.
Over the past three decades, squamous cell carcinoma of the oesophagus has remained steady in the United States and other Western countries, whereas the incidence of oesophageal adenocarcinoma has been progressively rising. The incidence of EAC increased significantly in white men. Sex and race variations in occurrence still exist, despite the fact that rising incidences have been observed in white women and black men: the white: black ratio is approximately 5:1, while the male: female incidence ratio is 8:1 [72]. The causes of these variations are not well known [73]. Given that the incidence of EAC is rising in tandem with the fast rise in the number of obese people, and that obesity is known to raise the risk of numerous malignancies in Western nations [74], GERD is recognised as a risk factor for EAC. Obesity is also considered to be a risk factor.
Numerous case-control studies provide credence to this theory [77, 78]. According to a meta-analysis by Hampel et al., there is a statistically significant increase in the risk for EAC for both being overweight (BMI, 25–30 kg/m2) and obese (BMI > 30 kg/m2) (OR, 1.52; 95% CI, 1.147–2.009 vs. OR, 2.78; 95% CI, 1.850–4.164, respectively).
The oesophageal squamous epithelium is replaced by a metaplastic columnar cell-lined epithelium in BE, the condition from which most EACs arise. Histologically, the metastasis-dysplasia-carcinoma sequence correlates the progression of BE to adenocarcinoma.” 10% of people with GERD go on to develop BE, and GERD is a risk factor for BE. In patients with BE, the annual incidence of adenocarcinoma development is 0.3%–1% [79]. As a result, obesity may be tangentially linked to BE because, as was previously mentioned, it may be a risk factor for GERD. Furthermore, obesity may directly affect the susceptibility for advancement to oesophageal cancer, even if it is uncertain what causes the conversion of a benign oesophageal epithelium to a malignant epithelium.
High BMI may accelerate the development of BE into EAC [80], according to an epidemiological study. While 60% of people with EAC have reportedly experienced GERD symptoms in the past, 40% have never experienced reflux symptoms [81]. Adenocarcinoma after BE can occasionally be found in asymptomatic individuals [82], and some people do not exhibit GERD symptoms [59, 60]. Identification of risk factors for BE other than GERD would be very helpful in the identification of asymptomatic BE and EAC. However, these risk variables are not well recognised. There are few studies examining the relationship between obesity and BE risk.
While Chak et al. [83] demonstrated that obesity was linked to the length of obesity rather than the presence of BE, Stein et al.[84] observed that obese patients are more likely to develop BE. According to Smith et al. [85], BE was significantly more likely among individuals with GERD symptoms who were obese, although obesity by itself did not cause this increase. It is still debatable if obesity poses a separate risk for BE. There is evidence that the obesity pattern affects the risk of several diseases. Compared to those with peripheral obesity, those with visceral obesity are more likely to develop insulin resistance syndrome and cardiovascular disease. In their investigation of the relationship between the pattern of obesity and BE development, El-Serag et al. [86, 87, 88] found a strong correlation between a higher risk of BE and both BMI and the surface areas of visceral adipose tissue (VAT), as determined by computed tomography scanning. When BMI was taken into account, VAT continued to have an independent relationship with BE, but the substantial correlation between BMI and BE vanished. In contrast to a greater BMI, a higher [89] WHR was significantly associated with increased chances of aneuploidy, loss of heterozygosity Thus, it is possible that visceral fat deposition plays a significant role in the development of GERD. Oestrogen may be involved in the relationship between BMI and GERD symptoms since it is higher in premenopausal women than in postmenopausal women [102]. Furthermore, increased serum levels of adipokines, such as interleukin (IL)-6 and tumour necrosis factor (TNF)-α, [103] are strongly linked to adipose tissues, particularly visceral adipose tissues, which are metabolically active and may contribute to GERD or the ensuing carcinogenesis. Adipose tissues release leptin primarily, and blood levels rise in direct proportion to body fat [104] accumulation. It has been demonstrated that leptin promotes cell division and prevents apoptosis in EAC cells generated from Barrett’s [105]. As genetic defects accumulate and remain, the traits of reduced apoptosis and enhanced proliferation, which are frequently observed in BE, play a crucial role in the development of cancer.
at chromosome 17p (17pLOH), and 9pLOH, all of which have been shown or considered to be predictive of further cancer development from BE [90]. Visceral obesity may therefore have a significant role in raising the risk of BE and encouraging BE to develop to EAC. The gender difference in EAC (male predominance) can be partially explained by the higher prevalence of visceral obesity in males.
The primary causes of gastric reflux disease (GERD) are increased transient lower oesophageal sphincter (LES) [91, 92] relaxation, hypotensive LES tone, and hiatal hernia. Moreover, disorders in salivary production, aberrant motility [93, 94, 95] of the oesophagus and stomach, or compromised mucosal defence [96] mechanisms can alter the extent of acid reflux injury. Obesity is thought to contribute to GERD, BE, and EAC through a number of pathways. Increased intra- abdominal pressure from obesity may result in an increase in intragastric pressure, which in turn may cause an increase in the gastroesophageal pressure gradient that causes LES relaxation [97]. Furthermore, obesity can cause an increase in intra-abdominal pressure, which can lead to the formation of a hiatal hernia and the displacement of the LES [98].
Consequently, the size of the hernia influences LES pressure and is a substantial independent risk factor for hiatal hernia. It also predicts the severity of esophagitis. The gastroesophageal pressure gradient and intragastric pressure [99, 100] are related to both BMI and WC, however WC has recently been shown to have a larger correlation than BMI [101].
There has been a rise in the prevalence of cardiac adenocarcinomas. There have been contradictory findings from a number of researches looking at the relationship between obesity and the risk of cardiac adenocarcinoma [106].
While some discovered either no association or a negative one, others reported an association with an increased risk of cardiac adenocarcinoma [107]. A 2006 meta-analysis revealed that there was heterogeneity in the overall association between high BMI and cardiac adenocarcinoma, and that in certain populations from the United States or Europe, a high BMI was weakly associated with the risk of cardiac adenocarcinoma (OR 0.5; 95%CI, 1.3–1.8); Chinese studies, on the other hand, did not reveal this association [108]. A diverse overall connection was also revealed by a meta-analysis conducted in 2005.
As such, there is ongoing debate over the relationship between obesity and the risk of cardiac adenocarcinoma.
With around 52,000 [109] fatalities each year from cancer, colorectal cancer is the second most common cause of cancer-related mortality in the US. Although a number of dietary and lifestyle factors, as well as a family history, have been associated to an increased risk [110, 111] of colorectal cancer, the exact origins of the disease are still unknown. Numerous studies have demonstrated that there is a correlation between a higher BMI and a higher risk of colorectal cancer, particularly in men [111]. Furthermore, Giovannucci et al. [112] showed that elevated WC and WHR values were significant risk factors for colorectal malignancies. The relative risk of colorectal cancer for WHR ≥ 0.99 compared to WHR < 0.90 was 3.41 (95% CI, 1.52– 7.66) and for WC ≥ 43 inches (about 109 cm) compared to WC < 35 inches (approximately 89 cm) was 2.56 (95% CI, 1.33–4.96). The relative risk of colorectal cancer for WHR ≥ 0.99 compared to WHR < 0.90 was 3.41 (95% CI, 1.52–7.66) and for WC ≥ 43 inches (about 109 cm) compared to WC < 35 inches (approximately 89 cm) was 2.56 (95% CI, 1.33– 4.96). Additionally, Schoen et al. [113] showed a significant correlation between higher WC measures and colorectal cancer. Given the higher prevalence of visceral obesity in males compared to women, it is believed that visceral obesity acts as a mediating factor between BMI and the elevated risk of colorectal cancer. Given that a malignant illness frequently affects a host’s body weight, anthropometric measurements in individuals with confirmed colorectal cancer are unlikely to be significant. Due to this, research has been done on the relationship between obesity and colorectal adenomas, which are known to be precancerous lesions of the colon and rectum [114]
According to Giovannucci et al., [115] BMI was not significantly related to an elevated risk of distal colon adenoma, regardless of size, whereas WC and WHR were unrelated to small adenomas with diameter less than 1 cm but major risk factors for large distal colon adenomas with diameter > 1 cm. Distal colon cancer has been observed to have a somewhat greater correlation between WC and an elevated risk of cancer.
When obesity functions as a risk factor for colon cancer, the degree of involvement may vary depending on the colon’s specific sections [116].
A significant contributing factor to the carcinogenesis of colon cancer has also been proposed to be being overweight during adolescence and into adulthood. Because there are so many confounding variables, it is difficult to investigate the relationship between obesity and the risk of colorectal cancer [117, 118]. Therefore, additional sub analyses are required.
Research has examined the correlation between several components of the metabolic syndrome and the risk of colorectal cancer. With proximal colon cancer being more likely, type 2 diabetes raises the risk of colon cancer by 1.3 to 1.6 times. It is unknown how insulin plays a part in the correlation between diabetes mellitus and a higher risk of colorectal cancer [119]. The relationship between high serum insulin levels and an increased risk of colorectal cancer is still unclear, despite Yoshida et al. [120] reporting a direct correlation between the presence of adenoma and hyperplastic polyps in the proximal colon and insulin levels [120, 121]. Numerous researchers looked into the possible link between elevated HDL cholesterol and triglycerides and the risk of colorectal cancer, but the findings were inconsistent, requiring more investigation [121, 122, 123]. Ahmed et al. investigated the possibility of metabolic syndrome as a colorectal cancer risk factor [124]. Age- and sex-adjusted colorectal cancer development was positively correlated with metabolic syndrome that met diagnostic criteria, and there was a dose-response relationship observed between the number of metabolic syndrome components and colorectal cancer development. Metabolic syndrome has been demonstrated to be a risk factor for colon cancer development in males but not in women, according to sex distribution study. In contrast to patients without polyps, Wang et al. [125, 126, 127] found that the OR of developing colorectal adenoma increased gradually with the amount of metabolic syndrome components present. For colorectal cancer, obesity is a significant risk factor. Adipose tissue, particularly VAT, is not just a tissue that stores fat; it is also a metabolically active organ that secretes several adipokines, which are proteins that are produced and secreted by adipocytes [128]. Examples of these proteins include TNF-α, IL-6, and adiponectin. Growth factors like insulin-like growth factor-1 (IGF-1), which is made in the liver, are also found in adipose tissue [128, 129]. Insulin resistance syndrome has been related to several molecules released by adipose tissue, including TNFα, IL-6, and adiponectin. Consequently, there is a substantial correlation between obesity and insulin resistance [128], a condition characterised by high levels of both insulin and IGF1. In vitro, insulin plays a crucial role in the growth of colonic mucosal cells and colonic carcinoma cells [129].
IGF-1 [130, 131] also inhibits apoptosis and accelerates the advancement of the cell cycle, which ultimately results in the development of cancer.
The relationship between hyperinsulinemia and colorectal neoplasm is unknown, however it is known that insulin has anti-inflammatory properties, and anti- inflammatory drugs have been demonstrated to lower the risk of colorectal neoplasm. Furthermore, adipose tissue has been proposed as the mediating factor in the relationship between obesity and tissue inflammation. Since ulcerative colitis patients acquire colorectal cancer due to chronic inflammation, it is hypothesised that this subclinical inflammation plays a role in the development of colorectal cancer [132].
Conclusion
Numerous gastrointestinal disorders seem to be associated with obesity, particularly visceral obesity. Since visceral obesity is the main component of metabolic syndrome, gastrointestinal disorders may be linked to metabolic syndrome. The relationships between specific elements of the metabolic syndrome, other than obesity, and gastrointestinal disorders have not been thoroughly investigated. According to recent research, diseases of the digestive system, such as upper gastrointestinal disorders, are associated with MS and visceral obesity in addition to arteriosclerotic and ischemic heart disease. As a result, it is concerning that there are more people with MS. There are recognised differences in the prevalence of MS and obesity according to gender, ethnicity, and geography. A cluster of metabolic abnormalities that meet the diagnostic criteria of metabolic syndrome may raise the risk of gastrointestinal diseases more than an individual metabolic abnormality because each component of metabolic syndrome may interact to increase the risk of gastrointestinal diseases.
The complex interplay between metabolic syndrome and upper gastrointestinal (GI) diseases underscores the importance of understanding metabolic syndrome as a multifaceted risk factor.
Metabolic syndrome, characterized by a cluster of conditions including insulin resistance, central obesity, dyslipidaemia, and hypertension, has been increasingly associated with various upper GI diseases such as gastroesophageal reflux disease (GERD), Barrett’s oesophagus, and oesophageal adenocarcinoma.
Research indicates that the pro-inflammatory state induced by metabolic syndrome exacerbates mucosal damage and impairs the healing process in the upper GI tract. The presence of central obesity and insulin resistance, key components of metabolic syndrome, are particularly implicated in the pathogenesis of GERD due to increased intra-abdominal pressure and altered oesophageal motility. Furthermore, the chronic low-grade inflammation characteristic of metabolic syndrome can contribute to the progression from GERD to Barrett’s oesophagus and eventually oesophageal adenocarcinoma.
The bidirectional relationship between metabolic syndrome and upper GI diseases suggests that management strategies should address both conditions concurrently. Lifestyle interventions, including dietary modifications, increased physical activity, and weight loss, have shown promise in mitigating the effects of metabolic syndrome and, subsequently, reducing the incidence and severity of upper GI diseases. Pharmacological treatments targeting the individual components of metabolic syndrome, such as antihypertensive and lipid-lowering agents, may also play a role in reducing upper GI disease risk.
In conclusion, the influence of metabolic syndrome on upper gastrointestinal diseases is profound and multifactorial. Effective management of metabolic syndrome can potentially alleviate the burden of upper GI diseases, highlighting the need for an integrated approach in both prevention and treatment. Future research should continue to explore the underlying mechanisms linking these conditions and develop targeted interventions to improve patient outcomes.
References
-
Cleeman JI, Grundy SM, Becker D, Clark L (2001) Executive summary of the third report of the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP III). Expert panel on detection, evaluation and treatment of high blood cholesterol in adults. Jama 285(19): 2486-2497.
-
Grundy SM (2002) Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation 106(25): 3143-3421.
-
Hyun JJ, Bak YT (2011) Clinical significance of hiatal hernia. Gut and liver 5(3): 267.
-
Patti MG, Goldberg HI, Arcerito M, Bortolasi L, Tong J (1996) Hiatal hernia size affects lower esophageal sphincter function, esophageal acid exposure, and the degree of mucosal injury. The American journal of surgery 171(1): 182-186.
-
Holtmann G, Shah A, Morrison M (2017) Pathophysiology of functional gastrointestinal disorders: A holistic overview. Dig Dis 35: 5-13.
-
Philpott H, Nandurkar S, Lubel J, Gibson PR (2014) Republished: Drug-induced gastrointestinal disorders. Postgrad. Med J 90: 411-419.
-
Francino MP (2016) Antibiotics and the human gut microbiome: Dysbioses and accumulation of resistances. Front. Microbiol 6: 1543.
-
Scarborough P, Bhatnagar P, Wickramasinghe KK, Allender S, Foster C, et al. (2011) The economic burden of ill health due to diet, physical inactivity, smoking, alcohol and obesity in the UK: An update to 2006–07 NHS costs. J Public Health 33: 527-535.
-
Sachs G, Scott DR (2012) Helicobacter pylori: Eradication or preservation. F1000 Med Rep 4: 4.
-
Thomas HJ, Xavier RJ (2020) Gastrointestinal diseases. In Hunter’s Tropical Medicine and Emerging Infectious Diseases pp: 18-27.
-
McQuaid KR (2012) Drugs used in the treatment of gastrointestinal diseases. In: Katzung BG (Ed.), Basic and Clinical Pharmacology. (12th Edn), McGraw-Hill Education/Medical, New York, NY, USA, pp: 1081-1114.
-
Gangarosa LM, Seibert DG (2004) Drugs used in gastrointestinal disorders. In: Craig CR, Stitzel RE (Eds.), Modern Pharmacology with Clinical Applications. (5th Edn), Lippincott Williams & Wilkins, Philadelphia, PA, USA, pp: 470-483.
-
Hindryckx P, Novak G, Bonovas S, Peyrin-Biroulet L, Danese S (2017) Infection risk with biologic therapy in patients with inflammatory bowel disease. Clin Pharmacol Ther 102(4): 633-641.
-
Parfitt JR, Driman DK (2007) Pathological effects of drugs on the gastrointestinal tract: A review. Hum. Pathol 38(4): 527-536.
-
El-Serag HB, Sweet S, Winchester CC, Dent J (2014) Update on the epidemiology of gastro-oesophageal reflux disease: A systematic review. Gut 63(6): 871-880.
-
Ford AC, Marwaha A, Sood R, Moayyedi P (2015) Global prevalence of, and risk factors for, uninvestigated dyspepsia: A meta-analysis. Gut 64(7): 1049-1057.
-
Scallan E, Griffin PM, Angulo FJ, Tauxe RV, Hoekstra RM (2011) Foodborne illness acquired in the United States— Unspecified agents. Emerg. Infect. Dis 17(1): 16-22.
-
Scallan E, Hoekstra RM, Angulo FJ, Tauxe RV, Widdowson MA (2011) Foodborne illness acquired in the United States—Major pathogens. Emerg. Infect. Dis 17(1): 7-15.
-
Wald A, Scarpignato C, Mueller-Lissner S, Kamm M, Hinkel U (2008) Multinational survey of prevalence and patterns of laxative use among adults with self-defined constipation. Aliment. Pharmacol Ther 28: 917-930.
-
Nyrop K, Palsson O, Levy R, Korff MV, Feld A (2007) Whitehead, W. Costs of health care for irritable bowel syndrome, chronic constipation, functional diarrhoea and functional abdominal pain. Aliment. Pharmacol. Ther 26(2): 237-248.
-
Oświęcimska J, Szymlak A, Roczniak W, Girczys-Połedniok K, Kwiecien J (2017) New insights into the pathogenesis and treatment of irritable bowel syndrome. Adv Med Sci 62(1): 17-30.
-
Aguirre JE, Winston J, Sarna SK (2017) Neonatal immune challenge followed by adult immune challenge induces epigenetic-susceptibility to aggravated visceral hypersensitivity. Neurogastroenterol Motil 29(9): e13081.
-
Bockus HL (1959) The Role of Hiatal Hernia in the Differential Diagnosis of Gastrointestinal and Cardiac Disease. Postgraduate Medicine 26(2): 185-91.
-
Soricelli E, Iossa A, Casella G, Abbatini F, Calì B, Basso N (2013) Sleeve gastrectomy and crural repair in obese patients with gastroesophageal reflux disease and/or hiatal hernia. Surgery for Obesity and Related Diseases 9(3): 356-361.
-
Hutopila I, Copaescu C (2019) Hiatal hernia is more frequent than expected in bariatric patients. Intraoperative findings during laparoscopic sleeve gastrectomy. Chirurgia 114(6): 779-789.
-
Lamouliatte H, Bernard P, Lefebvre P, Boulard A, Arnal J, et al. (1992) Hiatal hernia with intrathoracic gastric volvulus as a rare cause of biliary obstruction. Gastroenterologie clinique et biologique 16(1): 89-91.
-
Fu S, Xu M, Zhou H, Wang Y, Tan Y, et al. (2021) Metabolic syndrome is associated with higher rate of gastroesophageal reflux disease: a meta‐analysis. Neurogastroenterology & Motility 34(5): e14234.
-
Watanabe S, Hojo M, Nagahara A (2007) Metabolic syndrome and gastrointestinal diseases. Journal of Gastroenterology 42(4): 267-274.
-
Kallel L, Bibani N, Fékih M, Matri S, Karoui S, et al. (2011) Metabolic syndrome is associated with gastroesophageal reflux disease based on a 24-hour ambulatory pH monitoring. Diseases of the Esophagus 24(3): 153-159.
-
Niigaki M, Adachi K, Hirakawa K, Furuta K, Kinoshita Y (2013) Association between metabolic syndrome and prevalence of gastroesophageal reflux disease in a health screening facility in Japan. Journal of Gastroenterology 48(4): 463-472.
-
Richter J, Rubenstein J (2017) Presentation and Epidemiology of Gastroesophageal Reflux Disease. Gastroenterology 154(2): 267-276.
-
Healy L, Ryan A, Pidgeon G, Ravi N, Reynolds J (2010) Lack of differential pattern in central adiposity and metabolic syndrome in Barrett’s esophagus and gastroesophageal reflux disease. Diseases of the Esophagus 23(5): 386- 391.
-
Mocanu M, Diculescu M, Dumitrescu M (2013) Gastroesophageal reflux and metabolic syndrome. Revista medico-chirurgicala a Societatii de Medici si Naturalisti din Iasi 117(3): 605-609.
-
Clark C, Horwitz B (1996) Complications of gastroesophageal reflux disease. Esophagitis, acid laryngitis, and beyond. Postgraduate medicine 100(5): 95-97.
-
Ierardi E, Rosania R, Zotti M, Principe S, Laonigro G, et al. (2010) Metabolic syndrome and gastro- esophageal reflux: A link towards a growing interest in developed countries. World journal of gastrointestinal pathophysiology 1(3): 91-96.
-
Ryan A, Healy L, Power D, Byrne M, Murphy S, et al. (2008) Barrett Esophagus: Prevalence of Central Adiposity, Metabolic Syndrome, and a Proinflammatory State. Annals of Surgery 247: 909-915.
-
Leggett C, Nelsen E, Tian J, Schleck C, Zinsmeister A, et al. (2013) Metabolic syndrome as a risk factor for Barrett esophagus: a population-based case-control study. Mayo Clinic proceedings 88(2): 157-165.
-
Drahos J, Li L, Jick S, Cook M (2016) Metabolic syndrome in relation to Barrett’s esophagus and esophageal adenocarcinoma: Results from a large population-based case-control study in the Clinical Practice Research Datalink. Cancer epidemiology 42: 9-14.
-
Caro S, Cheung W, Fini L, Keane M, Theis B, et al. (2016) Role of body composition and metabolic profile in Barrett’s oesophagus and progression to cancer. European Journal of Gastroenterology & Hepatology 28: 251-260.
-
Phelan J, MacCarthy F, Feighery R, O’Farrell N, Lynam‐ Lennon N, et al. (2014) Differential expression of mitochondrial energy metabolism profiles across the metaplasia-dysplasia-adenocarcinoma disease sequence in Barrett’s oesophagus. Cancer letters 354(1): 122-131.
-
Gomes L, Esteves G, Carvalho A, Cristo E, Hirata R, et al. (2005) Expression profile of malignant and nonmalignant lesions of esophagus and stomach: differential activity of functional modules related to inflammation and lipid metabolism. Cancer research 65(16): 7127-7136.
-
Lin Y, Ness-Jensen E, Hveem K, Lagergren J, Lu Y (2015) Metabolic syndrome and esophageal and gastric cancer. Cancer Causes & Control 26: 1825-1834.
-
Coleman H, Xie S, Lagergren J (2017) The Epidemiology of Esophageal Adenocarcinoma. Gastroenterology 154(2): 390-405.
-
Pera M, Manterola C, Vidal O, Grande L (2005) Epidemiology of esophageal adenocarcinoma. Journal of Surgical Oncology 92.
-
Coffey R, Knight C, Heerden J, Weiland L (1985) Gastric adenocarcinoma complicating Gardner’s syndrome in a North American woman. Gastroenterology 88(5pt1): 1263-1266.
-
Worthley DL, Phillips KD, Wayte N, Schrader KA, Healey S, et al. (2011) Gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS): a new autosomal dominant syndrome. Gut 61(5): 774 - 779.
-
Li J, Woods S, Healey S, Beesley J, Chen X, et al. (2016) Point Mutations in Exon 1B of APC Reveal Gastric Adenocarcinoma and Proximal Polyposis of the Stomach as a Familial Adenomatous Polyposis Variant. American journal of human genetics 98(5): 830-842.
-
Lee JWJ, Koh CJ, Ho KY (2019) Metabolic syndrome and gastrointestinal cancers. Indian Journal of Gastroenterology 38: 3-5.
-
Yoon SY, Kim SY, Cho YH, Chung HY, So Y, et al. (2009) Hepatic metastases of gastric adenocarcinoma showing metabolic remission on FDG-PET despite an increase in size on CT. Cancer research and treatment: official journal of Korean Cancer Association 41(2): 100-103.
-
Karamurzin YS, Kiyokawa T, Parkash V, Jotwani AR, Patel P, et al. (2015) Gastric-type Endocervical Adenocarcinoma: An Aggressive Tumor with Unusual Metastatic Patterns and Poor Prognosis. The American Journal of Surgical Pathology 39(11): 1449-1457.
-
Schneider HJ, Glaesmer H, Klotsche J, Bohler S, Lehnert H, et al. (2007) Accuracy of anthropometric indicators of obesity to predict cardiovascular risk. J Clin Endocrinol Metab 92(2): 589-594.
-
Locke GR, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ (1997) Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology 112(5): 1448-1456.
-
Flegal KM, Carroll MD, Ogden CL, Johnson CL (2002) Prevalence and trends in obesity among US adults, 1999–2000. JAMA 288(14): 1723-1727.
-
Murray L, Johnston B, Lane A, Harvey I, Donovan J, et al. (2003) Relationship between body mass and gastro- oesophageal re-flux symptoms: The Bristol Helicobacter Project. Int J Epidemiol 32(4): 645-650.
-
Locke GR , Talley NJ, Fett SL, Zinsmeister AR, Melton LJ (1999) Risk factors associated with symptoms of gastroesophageal reflux. Am J Med 106(6): 642-649.
-
Nandurkar S, Locke GR, Fett S, Zinsmeister AR, Cameron AJ, et al. (2004) Relationship between body mass index, diet, exercise and gastro-oesophageal reflux symptoms in a community. Aliment Pharmacol Ther 20(5): 497- 505.
-
Wajed SA, Streets CG, Bremner CG, DeMeester TR (2001) Elevated body mass disrupts the barrier to gastroesophageal reflux. Arch Surg 136(9): 1014-1018.
-
Clements RH, Gonzalez QH, Foster A, Richards WO, McDowell J, et al. (2003) Gastrointestinal symptoms are more intense in morbidly obese patients and are improved with laparoscopic Roux-en-Y gastric bypass. Obes Surg 13(4): 610-614.
-
Ruhl CE, Everhart JE (1999) Overweight, but not high dietary fat in-take, increases risk of gastroesophageal reflux disease hospitalization: the NHANES I Epidemiologic Followup Study. First National Health and Nutrition Examination Survey. Ann Epidemiol 9(7): 424- 435.
-
El-Serag HB, Graham DY, Satia JA, Rabeneck L (2005) Obesity is an independent risk factor for GERD symptoms and erosive esophagitis. Am J Gastroenterol 100(6): 1243-1250.
-
Nocon M, Labenz J, Willich SN (2006) Lifestyle factors and symptoms of gastrooesophageal reflux—a population- based study. Aliment Pharmacol Ther 23(1): 169-174.
-
Lagergren J, Bergstrom R, Nyren O (2000) No relation between body mass and gastrooesophageal reflux symptoms in a Swedish population based study. Gut 47(1): 26-29.
-
Fujiwara Y, Higuchi K, Shiba M, Yamamori K, Watanabe Y, et al. (2005) Differences in clinical characteristics between patients with endoscopy-negative reflux disease and erosive esophagitis in Japan. Am J Gastroenterol 100(4): 754-758.
-
Labenz J, Jaspersen D, Kulig M, Leodolter A, Lind T, et al. (2004) Risk factors for erosive esophagitis: a multivariate analysis based on the ProGERD study initiative. Am J Gastroenterol 99(9): 1652-1656.
-
Van Oijen MGH, Josemanders DFGM, Laheij RJF, Van Rossum LGM, Tan AC, et al. (2006) Gastrointestinal disorders and symptoms: does body mass index matter? Neth J Med 64(2): 45-49.
-
Lundell L, Ruth M, Sandberg N, Bove-Nielsen M (1995) Does massive obesity promote abnormal gastroesophageal reflux? Dig Dis Sci 40(8): 1632-1635.
-
Nilsson M, Johnsen R, Ye W, Hveem K, Lagergren J (2003) Obesity and estrogen as risk factors for gastroesophageal reflux symptoms. JAMA 290(1): 66-72.
-
Hampel H, Abraham NS, El-Serag HB (2005) Meta- analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med 143(3): 199-211.
-
Fraser-Moodie CA, Norton B, Gornall C, Magnago S, Weale AR, et al. (1999) Weight loss has an independent beneficial effect on symptoms of gastro-oesophageal reflux in patients who are over-weight. Scand J Gastroenterol 34(4): 337-340.
-
Wilson LJ, Ma W, Hirschowitz BI (1999) Association of obesity with hiatal hernia and esophagitis. Am J Gastroenterol 94: 2840-2844.
-
Kjellin A, Ramel S, Rossner S, Thor K (1996) Gastroesophageal reflux in obese patients is not reduced by weight reduction. Scand J Gastroenterol 31: 1047- 1051.
-
Cremonini F, Locke GR, Schleck CD, Zinsmeister AR, Talley NJ (2006) Relationship between upper gastrointestinal symptoms and changes in body weight in a population- based cohort. Neurogastroenterol Motil 18: 987-994.
-
El-Serag HB, Ergun GA, Pandolfino J, Fitzgerald S, Tran T, et al. (2006) Obesity increases esophageal acid exposure. Gut pp: 24.
-
Devesa SS, Blot WJ, Fraumeni JF (1998) Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 83: 2049-2053.
-
Blot WJ, McLaughlin JK (1999) The changing epidemiology of esopha-geal cancer. Semin Oncol 26: 2-8.
-
Botterweck AA, Schouten LJ, Volovics A, Dorant E, Van Den Brandt PA (2000) Trends in incidence of adenocarcinoma of the oesophagus and gastric cardia in ten European countries. Int J Epidemiol 29: 645-654.
-
Chow WH, Finkle WD, McLaughlin JK, Frankl H, Ziel HK, et al. (1995) The relation of gastroesophageal reflux disease and its treatment to adenocarcinomas of the esophagus and gas-tric cardia. JAMA 274: 474-477.
-
Lagergren J, Bergstrom R, Lindgren A, Nyren O (1999) Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocar-cinoma. N Engl J Med 340: 825- 831.
-
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003) Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 348: 1625-1638.
-
Brown LM, Swanson CA, Gridley G, Swanson GM, Schoen- berg JB, et al. (1995) Adenocarcinoma of the esophagus: role of obesity and diet. J Natl Cancer Inst 87: 1049.
-
Vaughan TL, Davis S, Kristal A, Thomas DB (1995) Obesity, alcohol, and tobacco as risk factors for cancers of the esophagus and gas-tric cardia: adenocarcinoma versus squamous cell carcinoma. Cancer Epidemiol Biomarkers Prev 4: 85-92.
-
Lagergren J, Bergstrom R, Nyren O (1999) Association between body mass and adenocarcinoma of the esophagus and gastric cardia. Ann Intern Med 130: 883- 890.
-
Veugelers PJ, Porter GA, Guernsey L, Casson AG (2006) Obesity and lifestyle risk factors for gastroesophageal reflux disease, Barrett esophagus and esophageal adenocarcinoma. Dis Esophagus 19: 321-328.
-
Jankowski JA, Wright NA, Meltzer SJ, Triadafilopoulos G, Geboes K, et al. (1999) Molecular evolution of the metaplasia–dysplasia–adenocarcinoma sequence in the esopha-gus. Am J Pathol 154: 965-973.
-
Eloubeidi MA, Provenzale D (2001) Clinical and demographic predic-tors of Barrett’s esophagus among patients with gastroesophageal reflux disease: a multivariable analysis in veterans. J Clin Gastro-enterol 33: 306-309.
-
Conio M, Filiberti R, Blanchi S, Ferraris R, Marchi S, et al. (2002) Risk factors for Barrett’s esophagus: a case– control study. Int J Cancer 97: 225-229.
-
Phillips RW, Wong RK (1991) Barrett’s esophagus. Natural history, incidence, etiology, and complications. Gastroenterol Clin North Am 20: 791-816.
-
Winters C, Spurling TJ, Chobanian SJ, Curtis DJ, Esposito RL, et al. (1987) Barrett’s esophagus. A prevalent, occult complication of gastroesophageal reflux disease. Gastroenterology 92: 118-124.
-
Drewitz DJ, Sampliner RE, Garewal HS (1997) The incidence of adenocarcinoma in Barrett’s esophagus: a prospective study of 170 pa-tients followed 4.8 years. Am J Gastroenterol 92(2): 212-215.
-
Miros M, Kerlin P, Walker N (1991) Only patients with dysplasia prog-ress to adenocarcinoma in Barrett’s oesophagus. Gut 32(12): 1441-1446.
-
O’Connor JB, Falk GW, Richter JE (1999) The incidence of adenocar-cinoma and dysplasia in Barrett’s esophagus: report on the Cleve-land Clinic Barrett’s Esophagus Registry. Am J Gastroenterol 94(8): 2037-2042.
-
Anderson LA, Murphy SJ, Johnston BT, Watson P, Comber H, et al. (2005) Obesity and smoking in patients with Barrett’s esophagus and esophageal adenocarcinoma: results from the Finbar study. Gastroenterology 128(Suppl 3): A49-50.
-
Gerson LB, Shetler K, Triadafilopoulos G (2002) Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology 123(2): 461-467.
-
Menke-Pluymers MB, Schoute NW, Mulder AH, Hop WC, van Blankenstein M, et al. (1992) Outcome of surgical treatment of adenocarcinoma in Barrett’s oesophagus. Gut 33(11): 1454-1458.
-
Wakelin DE, Al-Mutawa T, Wendel C, Green C, Garewal HS, et al. (2003) A predictive model for length of Barrett’s esophagus with hiatal hernia length and duration of esophageal acid exposure. Gastrointest Endosc 58(3): 350-355.
-
Stein DJ, El-Serag HB, Kuczynski J, Kramer JR, Sampliner RE (2005) The association of body mass index with Barrett’s oesophagus. Aliment Pharmacol Ther 22(10): 1005-1010.
-
Chak A, Lee T, Kinnard MF, Brock W, Faulx A, et al. (2002) Familial aggregation of Barrett’s oesophagus, oesophageal ade-nocarcinoma, and oesophagogastric junctional adenocarcinoma in Caucasian adults. Gut 51(3): 323-328.
-
Smith KJ, O’Brien SM, Smithers BM, Gotley DC, Webb PM, et al. (2005) Interactions among smoking, obesity, and symp-toms of acid reflux in Barrett’s esophagus. Cancer Epidemiol Biomarkers Prev 14(11): 2481-2486.
-
El-Serag HB, Kvapil P, Hacken-Bitar J, Kramer JR (2005) Abdominal obesity and the risk of Barrett’s esophagus. Am J Gastroenterol 100(10): 2151-2156.
-
Vaughan TL, Kristal AR, Blount PL, Levine DS, Galipeau PC, et al. (2002) Nonsteroidal anti-inflammatory drug use, body mass index, and anthropometry in relation to genetic and flow cytometric abnormalities in Barrett’s esophagus. Cancer Epidemiol Biomarkers Prev 11(8): 745-752.
-
Mittal RK, Balaban DH (1997) Mechanisms of Disease: The esophagogastric junction. N Engl J Med 336(13): 924-932.
-
Dent J, Dodds WJ, Friedman RH, Sekiguchi T, Hogan WJ, et al. (1980) Mechanism of gastroesophageal reflux in recumbent asymptomatic human subjects. J Clin Invest 65(2): 256-267.
-
Kawanishi M (2005) Development of reflux esophagitis following Heli-cobacter pylori eradication. J Gastroenterol 40(11): 1024-1028.
-
Patti MG, Goldberg HI, Arcerito M, Bortolasi L, Tong J, et al. (1996) Hiatal hernia size affects lower esophageal sphincter func-tion, esophageal acid exposure, and the degree of mucosal injury. Am J Surg 171(): 182-186.
-
Iwakiri K, Sugiura T, Hayashi Y, Kotoyori M, Kawakami A, et al. (2003) Esophageal motility in Japanese patients with Barrett’s esophagus. J Gastroenterol 38(11): 1036- 1041.
-
McCallum RW, Berkowitz DM, Lerner E (1981) Gastric emptying in patients with gastroesophageal reflux. Gastroenterology 80(2): 285-291.
-
Rourk RM, Namiot Z, Sarosiek J, Yu Z, McCallum RW (1994) Impairment of salivary epidermal growth factor secretory response to esophageal mechanical and chemical stimulation in patients with reflux esophagitis. Am J Gastroenterol 89(2): 237-244.
-
Asaoka D, Miwa H, Hirai S, Ohkawa A, Kurosawa A, et al. (2005) Altered localization and expression of tight- junction proteins in a rat model with chronic acid reflux esophagitis. J Gastroenterol 40(8): 781-790.
-
El-Serag HB, Tran T, Richardson P, Ergun G (2006) Anthropometric correlates of intragastric pressure. Scand J Gastroenterol 41(8): 887-891.
-
Barak N, Ehrenpreis ED, Harrison JR, Sitrin MD (2002) Gastro-oesophageal reflux disease in obesity: pathophysiological and therapeutic considerations. Obes Rev 3(1): 9-15.
-
Jones MP, Sloan SS, Jovanovic B, Kahrilas PJ (2002) Impaired egress rather than increased access: an important independent predictor of erosive oesophagitis. Neurogastroenterol Motil 14(6): 625-631.
-
Jones MP, Sloan SS, Rabine JC, Ebert CC, Huang CF, et al. (2001) Hiatal hernia size is the dominant determinant of esophagitis presence and severity in gastroesophageal reflux disease. Am J Gastroenterol 96(6): 1711-1717.
-
John BJ, Irukulla S, Abulafi AM, Kumar D, Mendall MA (2006) Systematic review: adipose tissue, obesity and gastrointestinal diseases. Aliment Pharmacol Ther 23(11): 1511-1523.
-
Considine RV, Sinha MK, Heiman ML, Kriauciunas A, Stephens TW, et al. (1996) Serum immunoreactive-leptin concentra-tions in normal-weight and obese humans. N Engl J Med 334(5): 292-295.
-
Ogunwobi O, Mutungi G, Beales IL (2006) Leptin stimulates proliferation and inhibits apoptosis in Barrett’s esophageal adenocarcinoma cells by cyclooxygenase-2- dependent, prostaglandin-E2-mediated transactivation of the epidermal growth factor receptor and c-Jun NH2- terminal kinase activation. Endocrinology 147(9): 4505- 4516.
-
Blot WJ, Devesa SS, Kneller RW, Fraumeni JF (1991) Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 265(10): 1287-1289.
-
Chow WH, Blot WJ, Vaughan TL, Risch HA, Gammon MD, et al. (1998) Body mass index and risk of adenocarcinomas of the esophagus and gastric cardia. J Natl Cancer Inst 90(2): 150–155.
-
Zhang J, Su XQ, Wu XJ, Liu YH, Wang H, et al. (2003) Effect of body mass index on adenocarcinoma of gastric cardia. World J Gastroenterol 9(12): 2658–2661.
-
Kubo A, Corley DA (2006) Body mass index and adenocarcinomas of the esophagus or gastric cardia: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev 15(5): 872-878.
-
American Cancer Society. Cancer facts and figures. NewYork: American Cancer Society; 2006.
-
Garland C, Shekelle RB, Barrett-Connor E, Criqui MH, Rossof AH, et al. (1985) Dietary vitamin D and calcium and risk of colorectal cancer: a 19-year prospective study in men. Lancet 1(8424): 307-309.
-
Giovannucci E (2002) Modifiable risk factors for colon cancer. Gastroenterol Clin North Am 31(4): 925- 943.
-
Chute CG, Willett WC, Colditz GA, Stampfer MJ, Baron JA, et al. (1991) A prospective study of body mass, height, and smoking on the risk of colorectal cancer in women. Cancer Causes Control 2(2): 117-124.
-
Bostick RM, Potter JD, Kushi LH, Sellers TA, Steinmetz KA, et al. (1994) Sugar, meat, and fat intake, and non-dietary risk factors for colon cancer incidence in Iowa women (United States). Cancer Causes Control 5(1): 38-52.
-
Graham S, Marshall J, Haughey B, Mittelman A, Swanson M, et al. (1988) Dietary epidemiology of cancer of the colon in western New York. Am J Epidemiol 128(3): 490-503.
-
Klatsky AL, Armstrong MA, Friedman GD, Hiatt RA (1988) The relations of alcoholic beverage use to colon and rectal cancer. Am J Epidemiol 128(5): 1007-1015.
-
Giovannucci E, Ascherio A, Rimm EB, Colditz GA, Stampfer MJ, et al. (1995) Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann Intern Med 122(5): 327-334.
-
Schoen RE, Tangen CM, Kuller LH, Burke GL, Cushman M, et al. (1999) Increased blood glucose and insulin, body size, and incident colorectal cancer. J Natl Cancer Inst 91(13): 1147-1154.
-
Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH (1992) Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med 327(19): 1350-1355.
-
Le Marchand L, Wilkens LR, Mi MP (1992) Obesity in youth and middle age and risk of colorectal cancer in men. Cancer Causes Control 3(4): 349-354.
-
Zhang Y, Bobe G, Revel JS, Rodrigues RR, Sharpton TJ, et al. (2020) Improvements in metabolic syndrome by xanthohumol derivatives are linked to altered gut microbiota and bile acid metabolism. Mol Nutr Food Res 64(1) :e1900789.
-
Szilagyi A (2019) Relationship (s) between obesity and inflammatory bowel diseases: Possible intertwined pathogenic mechanisms. Clin J Gastroenterol 13(2): 139- 152.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance