Computer-Aided Ergonomics: A Case Study for the Analysis of Resistance Training Exercises
This study features an analysis of the influences and effects of varying forms of execution while performing resistance training exercises from an ergonomic viewpoint using the University of Michigan’s 3D Statistic Strength Prediction Program (3DSSPP). The exemplary use case chosen is the performance of Deadlifts (DL), one of the main full body training exercises in resistance training. The purpose of this study is to show the potential ergonomic problem of lower back impact of the exercise when executed with inaccurate form using the 3DSSPP to exemplary assess the usability of this form of software analysis for the specific area of exercises in resistance training. Based on the findings from the analysis and the results, it can be concluded that according to the software a possible indicator for poor technique especially during phase 1 to 3 is the lower strength requirements on torso and hips in these postures when rounding the back, explaining why people tend to make these mistakes.
Introduction
Performing resistance training exercises is commonly known as a means not only to improve performance for professional sportsmen and sportswomen but is also widely used in areas of rehabilitation, injury prevention and health maintenance for the general public. Resistance training has been shown to be one of the great alternatives to improve muscular strength [1]. Deadlift is frequently performed primarily when the goal is the strengthening of thigh and posterior chain muscles; specifically gluteus, hamstrings, erector spinae and quadriceps [2]. Besides the positive effects provided by resistance training there is also a certain health risk to be considered, especially for inexperienced and young people. Studies on injuries caused by weightlifting in different age groups for example showed that the age group of 23‐30 year olds shows a lower amount of accidental caused injuries than younger groups but also that over 40% of that injuries are located in the trunk area [3]. In addition, studies on resistance training of young athletes for example suggest, that most of the injuries among younger athletes stem from insufficient supervision of the young and often less experienced athletes, which results in poor exercise techniques and wrong assessment of training loads [4]. Koderi, et al. [5] performed a study to determine the effect of three different stances which were narrow, shoulder, and wide stance on the number of repetitions completed and the level of muscle activation during Romanian deadlift (RDL).
These two pointers exemplary show the ergonomic risk of resistance training, especially if performed with poor technique for whatever reason (inexperience, wrong assessment of own performance, inadequate training loads). The deadlift, a full‐body exercise putting most effort on the lower body and the back, shows a significant risk for the trunk, or to be more exactly for the lower back, which will be shown later in the task description. The goal is to assess the use of modern means of analysis (3D analytical software) to show and reproduce the results form former research, in order to enable its usage to develop and evaluate solutions for prevention and handling of the identified problems.
The literature review contained different areas to be covered. Starting off the project with suitable descriptions for the exercise in focus (the deadlift) [6, 7] and additional sources to identify common mistakes and posture variations [4, 8] further review led to more insight into the dynamics of different exercise variations and the expectable outcomes [3, 9]. Also information regarding the analysis had to be reviewed regarding the biomechanical process of the exercise [10] and last but not least the information needed to operate and assess the usability of the 3DSSPP software used in the project [11]. Finally information on how to interpret the levels and limits of measurements used within in the software had to be gathered and interpreted in order to allow a proper assessment of the results later on National Institute for Occupational Safety and Health [12] and Center for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS) [13].
Methodology
Problem Statement/Task Description
The Deadlift (DL): While there are numerous descriptions in the literature, it can be summarized that there are different variations of the DL. The most known are: Conventional DL, Stiff-legged DL, Romanian DL, Sumo DL. Additional variation can be incorporated by adjusting stance width, standing on one leg, different grips and the use of different weight forms as there are barbells, dumbbells kettlebells, weight‐vests or simply body weight. Most of the variations are meant to be used for specific application areas or to reach certain training goals. But being a full body exercise the application area for the DL is wide and can be of diverse use. For this study, the focus lies on the conventional DL for a simple reason. To assess the usability of a tool to analyze a certain problem, a variation is selected that will expectably have a higher and therefore more significant impact on the lower back. As for example McGuigan and Wilson [10] state in their comparison of conventional and sumo style DL, the sumo DL has different mechanical advantages with a more upright trunk posture leading the way causing a lower L4/L5 torque [10]. The technique used to perform the conventional DL can be seen in different phases but should always be foregone by a proper setup.
Therefore, the execution is divided into the following phases:
- Setup / stance and posture adjustment
- Lift start
- Lift below the knee
- Lift above the knee
- Lift End The segmentation into an important preparation [7] and the
4 lifting phases chosen for this description and according to other sources [6] will later be beneficial to have different “static” postures to analyze via the 3DSSPP software.
Three Dimensional Statistic Strength Prediction Program (3DSSPP)
In this study, the 3DSSPP software was performed to assess in terms of usability for the analysis of movements in resistance training. It is meant to predict static strength requirements for different tasks using posture data, forces and anthropometry. Different outputs can be generated like percentages of populations who will be able to perform a simulated job in terms of strength, data comparisons to NIOSH guidelines and the spinal compression forces that will be of interest for this study. Features like the 3D graphic illustration and the automatic posture generator can help to set up the model properly to the DL. A special purpose mentioned in the description of the software on the University of Michigan’s homepage is the usability of the software for “the analysis of the “slow” movements used in heavy materials handling tasks since biomechanical computations assume that the effects of acceleration and momentum are negligible” [11]. Based on this assumption, it is aimed to assess the usability for the resistance training movement, which also shows comparable characteristics of the “slow movements in heavy material handling” mentioned above.
Results and Discussion
The first finding while using the software to generate the results is that in order to compare the lower back impact for the postures we need to adjust the angles of trunk flexion as well as the pelvic flexion independently. For the trunk flexion this is no problem since it is adjustable for every posture separately. A direct posture input for the pelvic flexion angle is missing in the software even though both joints are displayed in the 3D models. Nevertheless, the pelvic flexion can be accessed by a parameter called “additional pelvic forward rotation” in the support section of the task input menu [11]. This parameter is originally meant as a “seating parameter” to help simulating for example standing (0° additional pelvic forward flexion), sitting (‐15°) or wheelchair (‐25°). Using this feature it is able to align the simulation models to the postures needed for the DL. One software‐design induced problem still remains. The 3DSSPP software provides a “dynamic mode” that allows the analyst to capture postures as a sequence and combine static postures to a virtual dynamic model. Since the pelvic flexion angle is not modeled as an adjustable posture parameter but as support parameter it is not adjustable individually for every posture. Changing the parameter for one posture will change it for all postures in the dynamic model. Therefore it is not possible to make use of the dynamic model in order to compare different sequences of execution techniques and we will compare every single posture of the DL to it’s comparable posture when using poor technique or making mistakes.
The simulation was set up to model a male subject anthropometrically representing the 50th percentile of the population and a hand load of 60 lbs. resulting in a total weight to lift of 120lbs, which is about ⅔ of the subjects body weight and represents a reasonable training weight for a trained recreational sportsman. 3DSSPPs automatic posture prediction method called “inverse kinematics” uses algorithms to compute the position of body joints based on the relative position of hands to feet using behavioral data. The feature enhanced by manual editing was used to align body posture and joints naturally but also approximating the different desired body postures for the DL exercise.
| Posture Variation | Start | Optimized | Normal | Difference | Rounded Back | Difference | Rounded Back, Hanging Shoulder | Difference |
|---|---|---|---|---|---|---|---|---|
| 3D Low Back Compression | ||||||||
| L4/L5 | lb | 1241 | 1422 | -181 | 1501 | -260 | 1597 | -356 |
| Strength Percent Capable | ||||||||
| Wrist | % | 98 | 98 | 0 | 98 | 0 | 97 | 1 |
| Elbow | % | 100 | 100 | 0 | 100 | 0 | 100 | 0 |
| Shoulder | % | 99 | 98 | 1 | 98 | 1 | 99 | 0 |
| Torso | % | 70 | 80 | -10 | 83 | -13 | 80 | -10 |
| Hip | % | 70 | 74 | -4 | 77 | -7 | 74 | -4 |
| Knee | % | 98 | 96 | 2 | 95 | 3 | 95 | 3 |
| Ankle | % | 98 | 98 | 0 | 99 | -1 | 99 | -1 |
Table 1: Start posture analysis.
| Posture Variation | Below Knee | Optimized | Rounded Back, Shooted Hips | Difference | Straight back, weight coming out | Difference |
|---|---|---|---|---|---|---|
| 3D Low Back Compression | ||||||
| L4/L5 | lb | 1040 | 1449 | -409 | 1316 | -276 |
| Strength Percent Capable | ||||||
| Wrist | % | 95 | 95 | 0 | 94 | 1 |
| Elbow | % | 99 | 99 | 0 | 99 | 0 |
| Shoulder | % | 99 | 99 | 0 | 99 | 0 |
| Torso | % | 71 | 79 | -8 | 55 | 16 |
| Hip | % | 71 | 74 | -3 | 59 | 12 |
| Knee | % | 97 | 97 | 0 | 99 | -2 |
| Ankle | % | 98 | 98 | 0 | 89 | 9 |
Table 2: Below knee posture analysis.
For the start posture, four different variations were taken into account. All are characterized by a ‐20° vertical upper leg angle. The optimized posture is modeled with a +30° addition pelvic forward rotation which results in an approximately similar posture regarding a simulated lower back (disc compression) force on L4/L5 of 1241 pounds. The main strength limitation according to the data shown in Table 1 lays on the torso and the hip, where only 70% of the population will be capable of performing this posture regarding their strength. In comparison, the modeled “normal” posture variation, which has 0° addition pelvic forward rotation shows higher percentage capable levels, what explains why people might use this posture, but also puts 1422 pounds on the lower back, which is already very close to the NIOSH back compression upper limit (BCUL) of 1430 pounds.
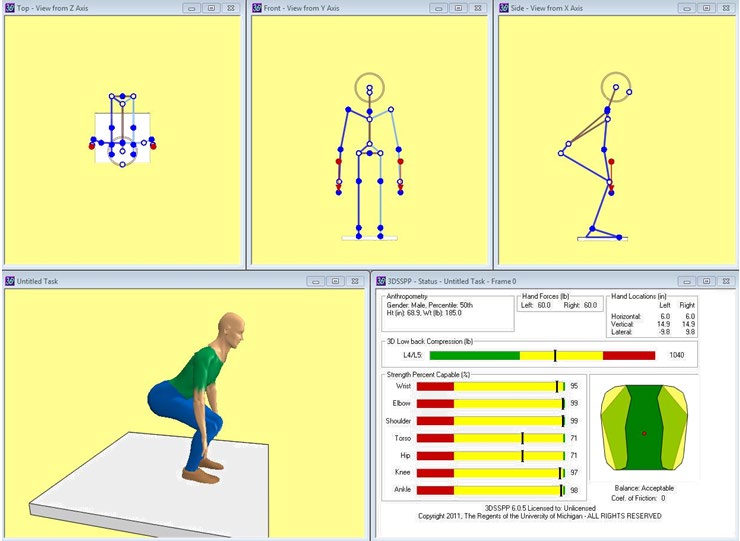
The second phase of the exercise, where the weight is moved below the knee, was modeled with a ‐30° vertical upper leg angle. Again the optimized posture shows a +30° additional pelvic forward rotation which results in 1040 pounds lower back compression (Figure 1) and is already lower than in the start posture (Table 2).
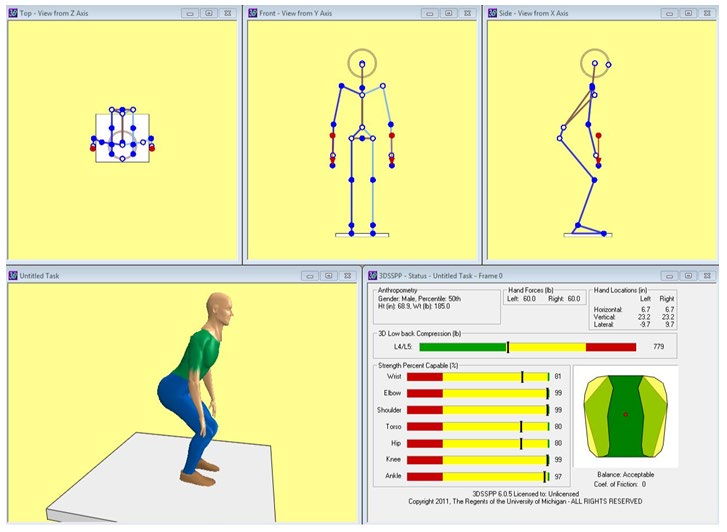
Moving the weight above the knee (phase 3) was modeled with ‐50° vertical upper leg angle and the optimized posture with a +15° addition pelvic forward rotation indicating the upbend of the upper body in this phase (Figure 2). As represented in Table 3, we note a L4/L5 compression of 779 pounds only slightly above the back compression design limit (BCDL) of 770 pounds according to NIOSH guidelines.
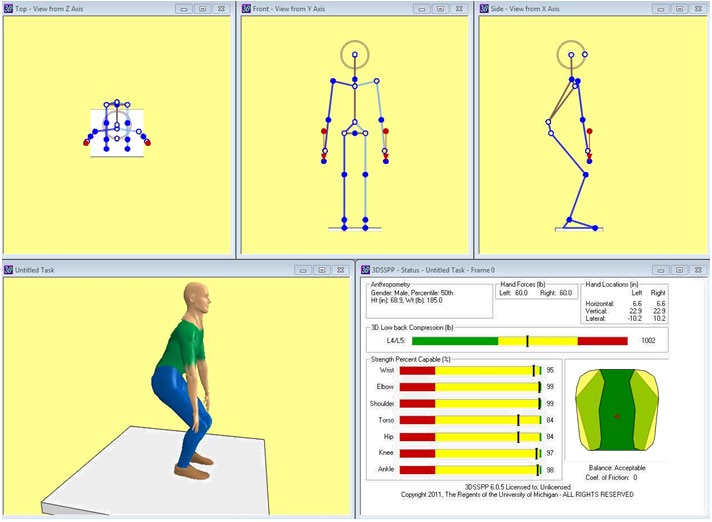
The limitations regarding strength of torso and hips are with 80% lower than in the phases before but with 81% the requirements regarding wrist strength rises. The poor technique with a rounded back and hanging shoulders (‐15° addition pelvic forward rotation and 0° clavicle horizontal angle) (Figure 3) again shows higher lower back compression but not the raised strength requirements on the wrists.
| Posture Variation | Above Knee | Optimized | Rounded Back, Hanging Shoulders | Difference |
|---|---|---|---|---|
| 3D Low Back Compression | ||||
| L4/L5 | lb | 779 | 1002 | -223 |
| Strength Percent Capable | ||||
| Wrist | % | 81 | 95 | -14 |
| Elbow | % | 99 | 99 | 0 |
| Shoulder | % | 99 | 99 | 0 |
| Torso | % | 80 | 84 | -4 |
| Hip | % | 80 | 84 | -4 |
| Knee | % | 99 | 97 | 2 |
| Ankle | % | 97 | 98 | -1 |
Table 3: Above knee posture analysis.
| End | Optimized | Hanging Shoulders | Difference | Hyperextended | Difference | |
|---|---|---|---|---|---|---|
| 3D Low Back Compression | ||||||
| L4/L5 | lb | 398 | 466 | -68 | 369 | 29 |
| Strength Percent Capable | ||||||
| Wrist | % | 99 | 99 | 0 | 62 | 37 |
| Elbow | % | 100 | 100 | 0 | 99 | 1 |
| Shoulder | % | 99 | 99 | 0 | 97 | 2 |
| Torso | % | 98 | 96 | 2 | 99 | -1 |
| Hip | % | 97 | 96 | 1 | 98 | -1 |
| Knee | % | 99 | 98 | 1 | 99 | 0 |
| Ankle | % | 98 | 97 | 1 | 99 | -1 |
Table 4: End posture (lock out) analysis.
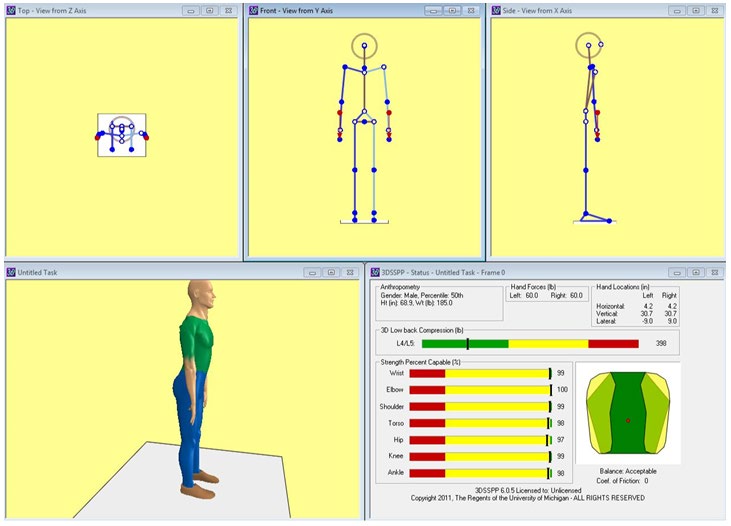
The final (lock out) posture shows ‐90° vertical upper leg angle (straight legs) and an additional pelvic forward rotation of 0° (Figure 4). The compression on the lower back is very low now (398 pounds) and well within the BCDL (Table 4). Also all strength requirement percentages are showing no problem regarding performing this posture. The hanging shoulders, modeled with 0° clavicle horizontal angle (instead of normal ‐20° when shoulders are back and tensed) result in 466 pounds on the back but also within the BCDL. The hyperextension of the back is modeled with a
100° trunk flexion (instead of 90°) and ‐5° clavicle horizontal angle instead of normal ‐20° to keep the weight on top of the thighs. Contrary to the expected values, this posture shows a lower compression of the back than the optimized posture but a significantly higher strength requirement on the wrists (only 62% capable instead of 99%).
Different conclusions can be drawn from the analysis of the DL exercise. As expected from the literature review, the lower back compression was highest in the beginning and lower at the end of the exercise, supporting the literature. Also as expected the performance using an optimized posture, mostly characterized by additional forward pelvic flexion supporting the lower back, resulted in lower compression force on the lower back discs. While there are multiple references and sources for common mistakes and their impact especially on the lower back, less information is present on why people are making these mistakes. Based on the findings from this analysis and the results we can conclude that according to the software a possible indicator for poor technique especially during phase 1 to 3 is the lower strength requirements on torso and hips in these postures when rounding the back, explaining why people tend to make these mistakes. The hanging shoulders, often accompanying the rounded back in these phases intensify the effect. Also, an increased wrist strength requirement towards the end of the exercise (phase 3 and 4) was noticed, but it is not assessable at this point if this is only task related or influenced by improper modeling of wrist postures (which was beyond the scope of the report) or the lack of a possibility to model the weight as a bar in the software which will be discussed later on. Other aspects like an explanation for the hanging shoulders in phase 4 could not be assessed by the software since according to the measurements there were no advantages to this posture regarding for example lower strength requirement on certain joints. So it is not reproducible why people tend to make this mistake while there seems to be no need to do so. It was also not possible to show the expected negative impact on the lower back during hyperextension of the back at the end of the exercise movement (phase 4) with the software.
Some of the findings have to be seen in close relationship with the assessment of the usability of the software as stated in the projects purpose. Especially the findings regarding the wrist strength requirements could be caused by an inaccurate modeling of the weight as two independent forces on the two hands. An additional feature in the software to model the weight as a bar gripped with both hands, which in case of the DL would be pressed against or lie on the thighs during some postures, could solve the problem, deliver more reliable data and improve the usability for this specific and similar kinds of analysis. Also beyond the scope of this study is the further assessment of the “inverse kinematics” feature and if the algorithms in particular support the desired postures or have to be adjusted. Especially the implementation of the pelvic flexion in relation to the trunk flexion should be designed as an adjustable value for the body posture to be used for dynamic sequences of postures and to be properly considered in the algorithms.
The software showed its potential the be used in this analytic environment by supporting finding from foregoing research (lower back pressure development over the phases, improvement by using optimized postures) and by revealing areas or aspects of interest to be further inspected (reasons for poor technique like lowered strength requirements on the mainly claimed joints when rounding the back, wrist strength requirements). Other aspects could not be supported or questioned (hyper‐extension impact on lower back, hanging shoulders at lock‐out) what again shows that this kind of tool should not be used as single determinant for an analysis but can very well be used to support and enrich it.
Conclusion
The first aspect to note, before drawing further conclusions from the results, is that the data gathered using the 3DSSPP software, especially regarding the lower back compression limits should be interpreted with care [11]. The data should be used to support findings and enable further research by revealing or carving out aspects and relationships within data sets but it should not be used as single source for determining strength performance or even workplace, job or task designs. Other assessment tools like REBA (rapid entire body assessment) and RULA (rapid upper limb assessment) are available and the appropriate mix of tools should be chosen according to the task to be analyzed. But using the data to support for example task design and assessment of, in this case training exercises, shows the importance of foregoing assessment of a tool like this to be used. Therefore, the findings can be divided into two categories: task related findings regarding the DL and findings regarding the usability of the software tool for the purpose of this analysis.
As already stated, further research should be done in different areas. Regarding the software, further addition of features to support the already mentioned aspects like improvement of usability of the dynamic model through independent pelvic flexion adjustment and modeling of additional weight types like for example bars could improve the overall usability and widen the area of application. Further assessment of algorithms regarding the wrist posture modeling in relation to certain grips could support the application in even more areas. The assessment method presented in this study will profit from further analysis of the postures to determine more exact joint angles (wrist posture, pelvic flexion, leg and shoulder angles etc.) on a larger test group to enhance validity of the results and the model itself. For the deadlift exercise itself further research could be done not only on the effect of poor technique and on the prevention of it, which both is well researched but in fact on the biomechanical aspect of why mistakes are made. This could lead to more and better recommendation of training weights for different groups of people in recreational and professional sports as well as in rehabilitation.
References
-
Suchomel TJ, Nimphius S, Bellon CR, Stone MH (2018) The importance of muscular strength: training considerations. Sports medicine 48(4): 765-785.
-
Krajewski KT, LeFavi RG, Riemann BL (2019) A biomechanical analysis of the effects of bouncing the barbell in the conventional deadlift. The Journal of Strength & Conditioning Research 33(S1): S70-S77.
-
Myer G, Quatman C, Khoury J, Eric J Wall, Timothy E Hewett (2009) Youth vs. adult “weightlifting” injuries presented to United States emergency rooms: accidental vs. Non-accidental injury mechanisms. The Journal of Strength & Conditioning Research 23(7): 2054‐2060.
-
Feigenbaum AD, Myer GD (2009) Resistance training among young athletes: safety, efficacy and injury prevention effects. British Journal of Sports Medicine 44(1): 56‐63.
-
Koderi KL, Tan K, Azzfar MS, Abd Malek NF, Mohamad NI, et al. (2020) The effects of stance width on muscle activation and performance during Romanian deadlift exercise. Journal of Physics: Conference Series, IOP Publishing 1529(2): 022026.
-
McDonald L (2008) Clean Style Deadlift Technique. Body Recomposition.
-
Robson D (2005) Deadlifts: The King of Mass‐ Builders? Bodybuilding.
-
Bird S, Barrington‐Higgs B (2010) Exploring the Deadlift. Strength and Conditioning Journal 32(2): 46‐51.
-
Escamilla RF, Francisco AC, Fleisig GS, Barrentine S, Welch CM, et al. (2000) A three dimensional biomechanical analysis of sumo and conventional style deadlifts. Medicine & Science in Sports & Exercise 32(7): 1265‐1275.
-
McGuigan MR, Wilson BD (1996) Biomechanical analysis of the deadlift. The Journal of Strength & Conditioning Research 10(4): 250‐255.
-
Center for Ergonomics (2020) 3D Static Strength Prediction Program Version 7.1.3 ‐ User’s Manual. Ann Arbor, University of Michigan, MI, USA.
-
NIOSH (1981) Work Practices Guide for Manual Lifting. Department of Health and Human Services, National Institute for Occupational Safety and Health, Cincinnat, Ohio, USA.
-
Centers for Disease Control and Prevention (2020) National Health and Nutrition Examination Survey Data. National Center for Health Statistics (NCHS), Department of Health and Human Services, Hyattsville, USA.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30