Susceptive, Supplemented, Stockpiled-Reactive Follicular Hyperplasia Lymph Node
Mini Review
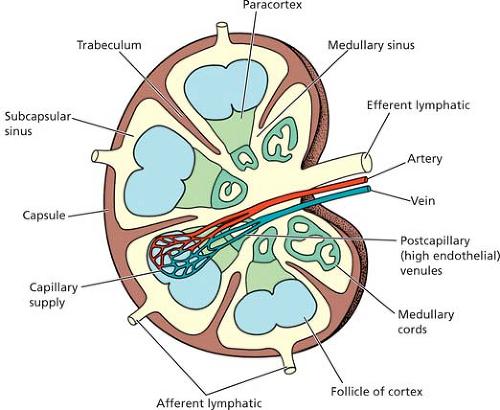
An oval tissue of nodular configuration, miniature dimensions and resemblance to a bean, composed of lymphoid tissue which is requisite for the filtration of the circulating lymph, essential for mounting an immune response and a constituent of the immune distribution is designated as the lymph node [1]. The lymph node is comprised of a coordinated architecture, composed of 4 principal anatomic subdivisions: the CORTEX, PARACORTEX, the MEDULLA and SINUSES [1]. The CORTEX is enclosed within the encapsulated perimeter of the lymph node. It is densely inhabited by the lymphocytic B cells which are configured into nodular aggregates and referred to as FOLLICLES. Contingent to the antigenic incitement, follicles may be denominated as either PRIMARY or SECONDARY [1]. Primary follicles are comprised of antigen naïve small, mature B cells. Secondary follicles articulate where primary follicles respond to antigenic stimulation and initiate a peripheral accumulation of small, mature B cells thereby configuring a mantle zone. The mantle zone encloses a central germinal centre formulated by antigen primed centroblasts and centrocytes which can differentiate into light and dark spheres when examined beneath polarized light. The antigen primed immature lymphoid cells may commingle with tingible body macrophages and follicular dendritic cells [1]. The PARACORTEX abounds with the lymphocytic T cells, a zone which interpolates with the B cell follicles and extensively intercalates into the cortex [1].
The paracortex is preponderantly constituted of small, mature T cells as well as a varying proportion of huge, transformed immunoblasts (originating from T cells and B cells), interdigitating dendritic reticulum cells, plasmacytoid dendritic cells and venules lined by a high endothelium. The MEDULLA is the centroidal domain in the lymph node abutting the hilum of the lymph node. It is fashioned with cords that are circumscribed by the medullary sinuses with an amalgamation of small B and T lymphocytes, plasmacytoid lymphocytes, plasmablasts and mature plasma cells [1]. Ultimately, the SINUSES incorporate endothelium lined vessels that intersect through the lymph node and transfer the lymph about the nodal parenchyma [1]. Lymph transported in the afferent lymphatic vessel infiltrates the node through the sub- capsular sinus, perambulates the node between the intermediary and medullary sinuses and eventually evacuates into the efferent lymphatic vessel, thus subsequently traverses beyond the lymph node [1] (Figures 1 & 2). Specific cellular constituents of the lymphatic sinuses comprise of histiocytes, lymphocytes, plasma cells and granulocytes [1]. Reactive alterations in lymph nodes are conventionally categorized by the histological arrangements established on the aforementioned anatomic subdivisions. FOLLICULAR/ NODULAR template which influence the cortex, INTERFOLLICULAR/ PARACORTICAL pattern – which impinges upon the paracortex, the SINUSOIDAL specification –which involves the lymphatic sinusoids in their entirety and the DIFFUSE prototype with the inclusion of two or more anatomic territories [1].
Reactive Follicular Hyperplasia (RFH)
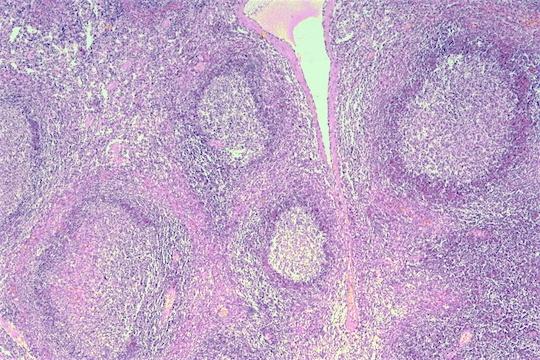
Concurs frequently in the Iymphnodes. Lymphoid follicles are the operative system of the B cell immune retroaction. It is an ambiguous peculiarity of an obscure aetiology [2]. Consequent to the inflammation and immune response are factors that provoke a humoral feedback, augment the stimulation of B cells and are usually accompanied with Reactive Follicular Hyperplasia (RFH) [2]. Disorders of precise aetiologies, innumerable Bacterial and Viral infections in conjunction with Autoimmune disease may also be accompanied by reactive follicular hyperplasia, besides displaying a specific histopathology which may comprise of aspects of infections (Human Immune-deficiency Virus, Epstein Barr virus, Toxoplasmosis, Syphilis), autoimmune disease (Rheumatoid Arthritis, Systemic Lupus Erythematosus), Castleman’s disease or Immunoglobulin 4 (IgG4) related disorders [3, 4, 5]. Follicular hyperplasia is distinguished by an enlargement of the cortex on account of a bilateral amplification in the count and diameter of the secondary lymphoid follicles which may sporadically extend into the paracortex and medulla. Follicular hyperplasia does not influence the normal lymph node configuration. The subdivisions of the lymph node, though attenuated, are discernible or the follicular hyperplasia may be accompanied by hyperplasia of the adjunct subsidiaries of the lymph node [2]. Manifests are the inconstant appearance and magnitude of the reactive follicles, which may characteristically elucidate polarized germinal centres. The secondary follicles are comprised of centroblasts and centrocytes with a mingling of tingible body (phagocytic) macrophages and small, mature B lymphocytes with a peripheral cuffing of a well structured and well delineated mantle zone [2] (Figures 3 & 4).
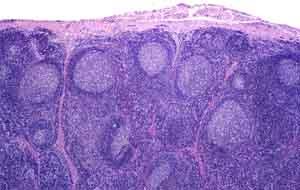
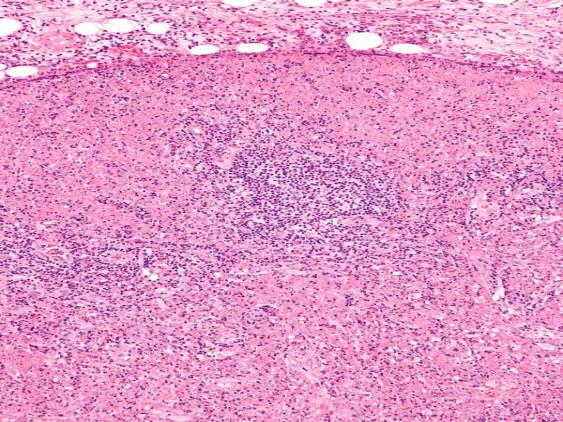
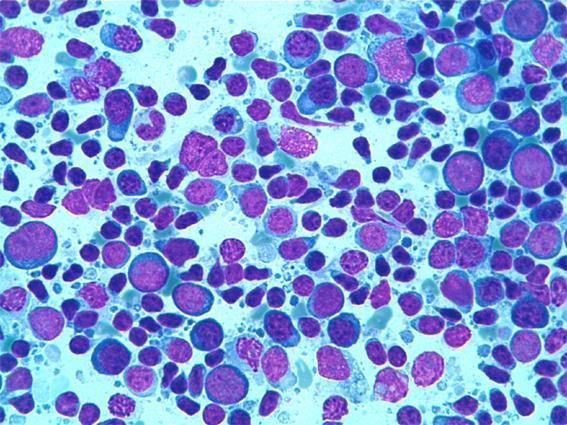
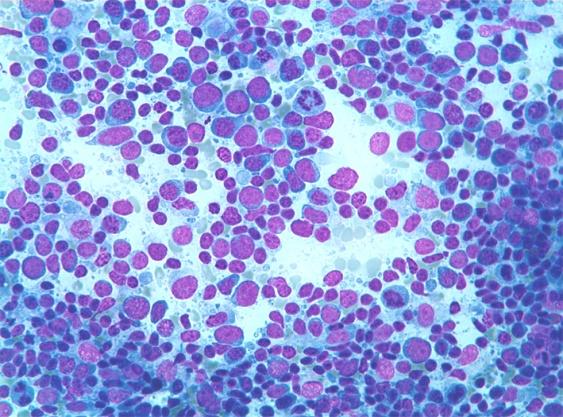
Reactive follicles elucidate a significant variation in the cellular metamorphosis. The perimeter is tapered, suitably etched and circumscribed by a mantle of small lymphocytes which frequently display an onion skin pattern, occasionally with an eccentric amalgamation of the circumferentially organized lymphocytes at one pole (concurrent with the edge of the antigenic stimulation) [2, 4]. The follicles are compounded of a commixture of small and large lymphoid cells with variable (elongated and cleaved) nuclei, prominent mitosis, intense phagocytosis of the nuclear debris by histiocytes and an emerging starry sky disposition. The inter-follicular lymphoid tissue, incorporated betwixt the lymphoid follicles is specifically diverse from the cellular components of the follicles (the feature validates in follicular lymphomas) [2]. It is constituted of an amalgamation of small lymphocytes, large lymphoid cells, protuberant post capillary venules and occasionally, a conspicuous fraction of mature plasma cells. Numerous inflammatory and non infectious disorders may predispose to follicular hyperplasia. With massive (giant) reactive follicles, a concurrent infection with Epstein Barr Virus may be implicated. Follicular Hyperplasia may integrate with Follicular Lymphoma in the synonymous lymph node besides auxiliary subdivisions of Malignant Lymphoma [2, 3, 4, 5]. MORPHOLOGICALLY Reactive Follicular Hyperplasia is typified by an augmentation in the enumeration and amplitude of the lymphoid follicles [4]. Numerous expansive lymphoid follicles may also adapt or consolidate to formulate random, erratic outlines. Despite these alterations, follicles with the hyperplasia maintain distinct mantle or marginal zones. The germinal centre is usually extended with the preservation of the light and dark regions. Disseminated within the reactive germinal centres are numerous tingible body macrophages, an appearance which imparts a starry sky pattern to the lymphoid tissue. In pure Reactive Follicular Hyperplasia, the paracortical zone is attenuated. Sinuses are usually evident and prominent, though an intensified component of the sinus cells (or littoral cells) may be visualized. Reactive lymphocytes generally infiltrate the lymph node capsule. However, the reactive follicles may occasionally extend into the abutting peri-nodal soft tissue [6, 7, 8]. Reactive Follicular Hyperplasia requires a distinction from a malignant lymphoid proliferation which may elucidate anodular growth architecture, preponderantly a Follicular Lymphoma (FL). Follicular Lymphoma commonly exhibits follicles that are extensive, numerous, proportionately dispersed (back to back) with identical dimensions on morphology, in contrast to the reactive follicles (Table 1). Tingible body macrophages are usually insufficient in follicular lymphomas and the mantle zone is inadequately depicted [9, 10, 11, 12] (Figures 5 & 6).
| Follicular Lymphoma | Reactive Follicular Hyperplasia |
| ARCHITECTURE: Complete effacement of architecture | Preservation of nodal architecture |
| Even distribution of follicles throughout cortex and medulla | Follicles more prominent in cortical portion of lymph node |
| Slight or moderate variation in size and shape of follicles | Marked variation in size and shape of follicles with presence of elongated, angulated and dumbbell shaped forms. |
| Fading of follicles | Sharply demarcated reaction centres |
| Massive infiltration of capsule and peri-capsular fat with or without formation of malignant follicles outside capsule | Nil or moderate infiltration of the capsule or peri-capsular fat with inflammatory cells that may be arranged as focal or peri-vascular aggregates(when accompanied with lymphadenitis) |
| Condensation of reticulin fibres at the periphery of the follicles | Little or no alteration of the reticular framework |
| CYTOLOGY: Follicles composed of malignant cells exhibiting cellular pleomorphism with nuclear aberrations. | Centres of follicles (reaction centres) composed of lymphoid cells, histiocytes and reticulum cells, with few or no cellular / nuclear aberrations. |
| Lack of phagocytosis | Active phagocytosis in reactive germinal centres |
| Relative paucity of mitotic figures usually without significant differences inside and outside the follicles, presence of atypical mitosis | Moderate to pronounced mitotic activity in reaction centres, rare or no mitosis outside reaction centres, no atypical mitosis |
| Analogy of cell type inside and outside the follicles | Infiltration of tissue between the reaction centres with inflammatory cells(accompanied with lymphadenitis) |
Table 1: Allegory of Reactive/ Lymphoid Neoplasm Follicles [10].
Immunohistochemistry
Immunohistochemical stains that are elucidated in the predominant lymphocytes of the reactive follicles, besides the centroblasts, centrocytes and the mantle zone lymphocytes are primarily the CD20 positive cells. Germinal centre B cells are reactive for CD10 and BCL 6 and non reactive for anti-apoptosis protein BCL2 [1]. Mantle zone B cells are reactive for IgD and BCL2, though lack the expression of CD10 and BCL6. Reactive germinal centres also comprise of dispersed small CD3+ follicular helper T cells that co-articulate CD4 and CD57, PD-1 and BCL2 [1, 2]. These T cells are prominent in the luminous region of the germinal centres. CD21 highlights a competently manufactured network of follicular dendritic cells delineated in the entirety of the follicles. Two lymphomas that elucidate identical traits on histology with follicular hyperplasia and may be misrepresented are Follicular Lymphoma and Mantle cell lymphoma. Along with the morphologic interpretation, immunophenotyping by immunohistochemistry and flow cytometry procures adequate information which assists in the differentiation of the reactive from the malignant propagation [1, 2]. The most appropriate immunologic stain to discriminate Reactive Follicular Hyperplasia from Follicular Lymphoma is the B cell lymphoma 2( BCL-2) stain which typically lacks enunciation by the reactive germinal centre B cells and is frequently propounded in the follicular lymphomas [1, 2]. Flow cytometry is beneficial for demonstrating the polytypic B cells in Reactive Follicular Hyperplasia. Occasionally, Immunoglobulin G heavy chain gene rearrangement analysis may be required in cases where the morphology and immune-phenotype are ineffective in producing irrefutable evidence of demarcation amidst the Reactive Follicular Hyperplasia and the B cell neoplasm. Lymph node diseases that elucidate a FOLLICULAR prototype [10]:
- Non specific reactive follicular hyperplasia.
- Secondary Syphilis.
- Rheumatoid arthritis.
- Castleman’s Disease (Hyaline Vascular and Plasma Cell type).
Hyperplastic Follicles
Histopathology and extensive immune mediated investigations facilitate in the determination of the Hyperplastic follicles which habitually comprise of a germinal centre circumscribed by an integrated, competent and a well delineated mantle zone [11]. CD3 may discern the limited number of T cells existing in the germinal centre. BCL-2 staining remains distinct and prominent within the mantle zone. B cells and T cells prevail within the para-cortical regions but the volume of BCL 2 reactive cells specified in the germinal centre may be equivalent to the perceived CD 3 reactive cells [13, 14, 15, 16, 17, 18]. Thus the quantification of mantle B cells (defined as BCL2+/CD3-) accessing the follicular germinal centre may be comparatively moderate within the hyper plastic follicles.
References
-
Slack GW (2016) The pathology and reactive lymphadenopathies: A Discussion of Common Reactive Patterns and Their Malignant Mimics. Arch Pathol Lab Med 140(9): 881-892.
-
Miranda RN (2013) Atlas of Lymph Node Pathology. Atlas of Anatomic Pathology” XIX pp: 530.
-
Weiss LM, O Malley D (2009) Benign Lymphadenopathy. Mod Pathol 26(1): S88-S96.
-
Ioachim HL “Reactive Follicular Hyperplasia” Ioachim’s Lymph Node Pathology”. 4th (Edn.), Phildelphia PA: Lippincott William and Wikins, pp: 172-180.
-
Jaffe ES (2011) “Hematopathology”. 1st (Edn.), St Louis MO Elseiver Saunders.
-
Kusick SJ Kalnoski M, Braziel RM, Wood BL (2004) Prominent Clonal B cell population identified by flow cytometry in histologically reactive lymphoid proliferations. Am J Clin Pathol 121(4): 464-472.
-
Loddenkemper C, Anagnostopoulos I, Hummel M, Jöhrens Leder K, Foss HD, et al. (2004) Differential Emu enhancer activity and expression of BOB.1 OBF.1 Oct-2.PU.1 & immunoglobulin in reactive B cell populations, B cell Non Hodgkin’s Lymphoma & Hodgkin’s Lymphomas. J Pathol 202(1): 60-69.
-
Segal GH, Perkins SL, Kjeldsberg CR (1995) Benign Lymphadenopathies in children and adolescents. Semin Diagn Pathol 12(4): 288-302.
-
De wolf Peters C (1993) Anatomy and Histopathology of lymphoid tissue. Semin Oncol 20: 555-569.
-
Rosai and Ackerman”s “Surgical Pathology”. 10th (Edn.), pp: 1782.
-
Chang CC, Osipov V, Wheaton S, Tripp S, Perkins SL (2003) Follicular Hyperplasia, Follicular Lysis and Progressive Transformation of Germinal Centre” ‘A sequential spectrum of Morphologic Evaluation in Lymphoid Hyperplasia. Ame J Clin Path 120(3): 322- 326.
-
Van der Vauk P, Meijer CJ (1987) The histology of reactive lymph node. Am J Surg Pathol 11(11): 866- 882.
-
Lennert K, Müller Hermelink HK (1975) Lymphocytes and their functional forms: morphology, organization and immunologic significance. Verth Anat Ges 69: 19- 62.
-
Image 1 Courtesy: Pinterest.
-
Image 2 Courtesy: Med. Utah.edu.
-
Image 3 Courtesy: Pleiad.umdnj.edu
-
Image 4 Courtesy: Wikipedia.
-
Image 5 & 6 Courtesy: Euro-cytology.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient