Determining the Role of Serum Hyluronic Acid Levels to Degree of Fibrosis in Patients with Chronic Viral Hepatitis
Objective: In this study we aimed to investigate the value of hyaluronic acid levels, a non-invasive biochemical marker for the evaluation of liver fibrosis in patients with chronic hepatitis. Material and Methods: The study comprised 80 patients in Ataturk University Infectious Disease Clinic (48 with chronic hepatitis B and 32 with chronic hepatitis C) between 2008-2009. Patients were grouped into two for statistical analysis according to their liver fibrosis stage. Mild for no fibrosis (Stage 0,1,2) was accepted as group 1, severe fibrosis (stage3,4) was evaluated as group 2 For determining serum hyaluronic asit levels concomitantly to liver biopsy blood was taken, centrifuged, serums were separated. These serums were kept in suitable conditions until they were studied with ELISA method. Serum hyaluronic acid was compared between two groups. For evaluating results, comparing binary numerical variables student-t test, for multiple comparisons one way anova test were used.Results: In our study serum hyaluronic acid levels were significantly increasing in patients with increasıng fıbrosıs (p=0,003). When comparing HA between chronic hepatitis B and chronic hepatitis C; there is no statistical significance. However HA level were directly proportional to liver fibrosis. Conclusions: There is significant correlation between serums HA levels and severity of liver fibrosis. For thıs reason in determination of severe fibrosis which is a transition time to cirrhosis and cirrhosis itself, HA levels seem to be a useful marker.
Neslihan Ç*1, Ayten Kadanali2, Ibrahim Kaplan3
training hospital, Turkey, Tel: 905333585549; Email: drneslihancelik@yahoo.com.tr for the evaluation of liver fibrosis in patients with chronic hepatitis.
variables student-t test, for multiple comparisons one way anova test were used.
However HA level were directly proportional to liver fibrosis.
marker.
Keywords: Fibrosıs; Hyaluronic; Hepatitis B Virus; Pneumothorax; Necroinflammatory; Biopsy
Introduction
Chronic inflammation in liver tissue always leads to fibrosis. While several factors can result in chronic inflammation in the liver, viral hepatitis are prominent due to their prevalence and contagiousness. Most frequent agents that cause chronic hepatitis are hepatitis B virus (HBV) and hepatitis C virus (HCV). Chronic inflammation and subsequent fibrosis in liver tissue causes severe disorders. Cirrhosis is the last stage of liver fibrosis and many complications of cirrhosis are due to liver fibrosis [1]. Currently, gold standard in the identification and measurement of fibrosis is histological evaluation tissue samples obtained by liver biopsy. The identification of presence and extent of liver fibrosis is of paramount importance in terms of directing the treatment and predicting the prognosis in patients with chronic liver injury [2]. The fact that liver biopsy is an invasive procedure, which can lead to severe complications (bleeding, pneumothorax, colon or gallbladder perforation) even in the hands of experienced physicians, is a significant drawback of this procedure [3]. Due to the challenges of histological evaluation, non- invasive biochemical markers are believed to help in the detection of histological injury and monitoring of fibrosis in chronic hepatitis [4]. Hepatic fibrosis is a complex and dynamic process that includes the increased accumulation of extracellular matrix (ECM) content, activation of ECM producing cells and cytokine secretion and tissue remodeling. Due to identification of increased ECM content in fibrotic liver tissue, ECM related materials became potential candidates as biomarkers of liver fibrosis. Among these, the following are most emphasized: hyaluronic acid (HA), type III collagen, and amino- terminal propeptid of type III precollege. It is thought that fibrosis markers such as these may help in the early detection of liver fibrosis and evaluation of its progression and extent [5, 6]. In our study, we sought to examine the place of HA, one of the non-invasive biochemical markers of liver fibrosis, in the evaluation of liver fibrosis in patients with chronic viral hepatitis B and C.
Materials and Methods
This study included patients who were hospitalized at the department of clinical microbiology and infectious diseases, Ataturk University Faculty of Medicine, between 2007 and 2008 with the diagnosis of viral hepatitis and were planned for liver biopsy. These patients had 6 months of follow-up with serological, biochemical and serological evaluation and all patients had chronic viral hepatitis. Eighty patients with chronic hepatitis B and C were included in the study. There were 48 patients with hepatitis B (37 males, 11 females) and 32 patients with hepatitis C (18 males, 14 females). All patients were informed before liver biopsy and consent was obtained. Biopsies were performed at radiology department and infectious diseases clinic percutaneously with 16-G or 18G needles under local anesthesia with the assistance of ultrasonography (USG). Tissue samples were sent to pathology department in 10% formalin solution. Masson’s trachoma and Sweet’s reticulum stains were used to evaluate fibrosis in tissue samples. A pathologist performed histological evaluation. Fibrosis and necroinflammatory activity was evaluated according to Knoodell’s classification. Severity of liver fibrosis was classified as Stage 0, 1, 2, 3, and 4. In order to make statistical comparisons, the patients were assigned into two groups according to the severity of fibrosis. Group 1 comprised of patients with Stage 0,1,2 liver fibrosis (no fibrosis ormild fibrosis) and Group 2 comprised of patients with Stage 3 and 4 liver fibrosis (severe fibrosis). Venous blood samples (5 cc) were collected from the patients, who underwent liver biopsy, with sterile plastic syringe for HA measurement. Blood samples were centrifuged at 3000 RPM. Serum samples were aliquoted into eppendorf tubes and stored at -80ºC until the measurements. Serum samples were transferred to +4ºC refrigerator 1 day before the measurement in the biochemistry laboratory. On the day of measurement, samples were kept at room temperature for thawing. After thawing, serum HA level was measured with ELISA method by using Hyaluronic Acid Test Kit (96-well) (Corgenix, Inc.). Data were analyzed with Statistical Package for Social Sciences (SPSS) for Windows 13, 0. Descriptive statistics were employed for all patients (mean, maximum, minimum, median, standard deviation). HA level between two groups were compared with t test. Within group and between groups comparisons of chronic hepatitis B (Group 1 and 2) and chronic hepatitis C (Group 1 and 2) patients in terms of HA level was performed with one- way ANOVA test. A p <0.05 was accepted as statistically significant.
Findings
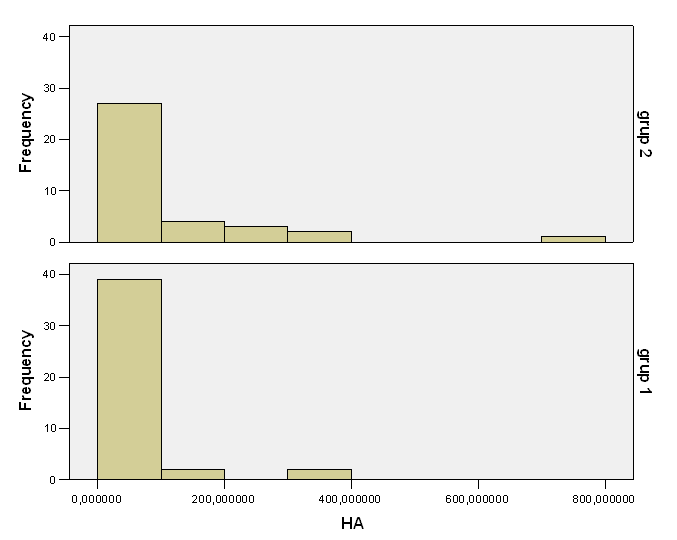
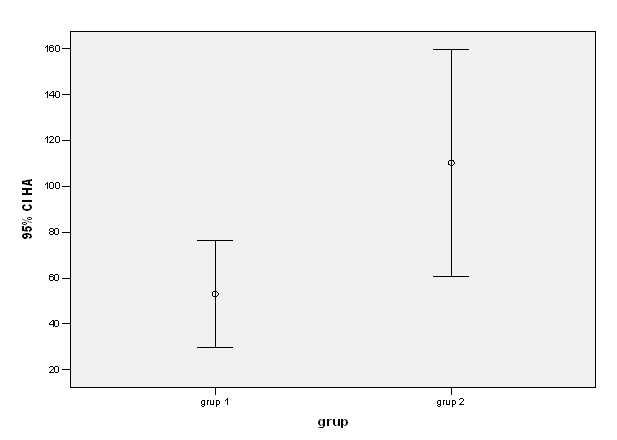
HA level in the Group 2 (severe fibrosis) was significantly higher than Group 1 (no fibrosis or mild fibrosis) (p=0,003).
| HA level (ng/ml) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | Min. | Max. | Median | ||||||||
| 1 | 0.96618 | 3,669,230 | 239,130 | ||||||||
| 2 | 7,971,010 | 800 | 55,706,520 |
HA levels in chronic hepatitis B (Group 1 and 2) patients and chronic hepatitis C (Group 1 and 2) patients were analyzed in terms of fibrosis severity.
| HBV Group 2 | HCV Group 1 | H | CVGrup | 2 | |||||
|---|---|---|---|---|---|---|---|---|---|
| HBV Group 1 | P= 0.014 | P= 0.571 | |||||||
| HBV Group 2 | P=0.769 | ||||||||
| HCV Group 1 | P=0.050 |
HA levels of patients with chronic hepatitis B in Group 1 and 2 were compared. In patients with chronic hepatitis B, HA level was significantly higher in Group 2 compared to Group 1 (p=0.014). Similarly, HA level was significantly higher in Group 2 compared to Group 1 in patients with chronic hepatitis C, as well (p=0.050). In Group 1, HA levels of patients with chronic hepatitis B and C were compared. The difference was not statistically significant (p=0.571). In Group 2, HA levels of patients with chronic hepatitis B and C were not significantly different also (p=0.769).
Discussion
Liver fibrosis is an important clinical condition because of its serious complications. The evaluation of liver fibrosis secondary to chronic liver injury is important in terms of treatment and follow-up. Chronic viral hepatitis is the most common cause for liver injury. As seen in other chronic liver disorders, the prognosis of chronic hepatitis is largely connected to liver fibrosis [7, 8, 9]. If liver injury is very large, this scar tissue transforms in nodule forming liver structures. This severe form of fibrosis is called as cirrhosis. It is very difficult to predict the level of fibrosis in a liver with clinical parameters [10]. Currently, the gold standard method for detection and staging of fibrosis is histological evaluation of liver biopsy materials. The identification of presence and extent of liver fibrosis is of paramount importance in terms of directing the treatment and predicting the prognosis in patients with chronic liver injury [2]. The fact that liver biopsy is an invasive procedure, which can lead to severe complications (bleeding, pneumothorax, and colon or gallbladder perforation) even in the hands of experienced physicians, is a significant drawback of this procedure [3]. These negative features lay the ground for the development of noninvasive methods to predict the amount of hepatic scar tissue and progression of fibrosis. Huge effort is being exerted to identify new serum biomarkers that can be used for non-invasive evaluation of hepatic fibrosis [2].
Liver fibrosis is a complex, dynamic process. This process includes increased ECM content production, activation of ECM producing cells, cytokine secretion and tissue remodeling. ECM is composed of collage nous proteins, non-collage nous proteins and hyaluronic acid. The synthesis and accumulation of these components increase during fibro genesis. Some of these products and their metabolites enter the systemic circulation and consequently serum levels of these metabolites increase [5]. In our study, we investigated the correlation between the severities of liver fibrosis in 80 patients, who underwent liver biopsy as part of the treatment planning, and HA, a noninvasive serum marker. The increase in HA level in patients with chronic hepatitis may reflect induction of HA production by active satellite cells or reduction of HA uptake and degradation by endothelial cells or both [11]. Its high levels in liver diseases especially in cirrhosis is thought to be related to endothelial sinusoidal cell dysfunction and considered as a marker of increased fibrogenesis [2]. Its concentration is low in normal liver and high in fibrotic liver [12]. Patel et al., in a study on 76 patients with hepatitis C, reported that HA level in patients with severe fibrosis was higher than that in patients with mild fibrosis. Furthermore, they also compared fibrosis and HA levels after treatment. While fibrosis score had not changed after the treatment, HA levels had decreased. They proposed that this result might be due to reduced collagen degradation, which could not be detected with histological evaluation [13]. With these results, it was suggested that HA can be used for direct follow-up of liver fibrosis and evaluation of response to antiviral treatment, moreover, it was recommended that serum HA monitoring can be used to follow-up the course of the disease in advanced liver fibrosis [14]. In our study, HA levels in Group 2 (patients with severe fibrosis) were higher than Groups 1 (patients with no fibrosis or mild fibrosis) (p=0,003). In patients with HBV, HA levels in Group 2 (patients with severe fibrosis) were higher than Groups 1 (patients with no fibrosis or mild fibrosis) (p=0.014). In patients with HCV, HA levels in patients in Group 2 were higher than those in Groups 1 (p=0.005). In comparison of HA levels in patients with HBV and HCV in Group1, there was not a statistically significant difference (p=0.571). Similarly, HA levels in Group 2 patients with HBV were not statistically different from those in Group 2 patients with HCV (p=0,769). Our findings confirm the results of previous studies and we found that serum HA levels increased proportionally with the severity of fibrosis. On the other hand, we did not find a difference between patients with chronic hepatitis B and chronic hepatitis C in terms serum HA levels. In another study, Arhan et al. investigated 43 patients with chronic hepatitis, and found that patients with severe fibrosis had significantly higher serum HA levels compared to those with mild fibrosis. The correlation between severities of fibrosis and HA levels were investigated in patients with HBV and HCV. Although HA level increased proportionally with the severity of fibrosis in patients with HB. On the other hand, HA level in patients with severe fibrosis was higher than that in patients with mild fibrosis in patients with HCV [15]. Chen YP et al. found that it is more sensitive than ultrasonography in the diagnosis of decompensate cirrhosis in patients with chronic hepatitis B. its use together with ultrasonography was not superior to its use alone. It was reported that it was correlated with serious inflammation and severe fibrosis [16]. In another study, Guechot et al. documented that serum HA level had a direct correlation with the severity of fibrosis in patients with liver fibrosis and HA gave reliable results in the evaluation of liver fibrosis in patients with chronic hepatitis [17]. Rosenberg et al. proposed that progressive liver injury in patients with chronic liver could be shown at the earliest by serum HA level [18]. Likewise, Murawaki et al. reached same conclusion in a similar study [19]. Li F et al. documented that serum HA and laminin levels are correlated with fibrosis level in patients with chronic hepatitis B [20]. Olga Hilda Orasan et al. found that HA level increased in parallel with fibrosis level in patients with hepatitis B and C. In hepatitis C, HA level was lower in patients with Stage 0, 1 fibrosis compared to those with Stage 2-4 fibrosis [21]. In another study, Olga Hilda Orasan et al. concluded that HA is a non-invasive parameter, which shows fibrosis level in chronic hepatitis B and C [22]. In the previous studies, it was showed that serum HA is correlated with severity of liver fibrosis in patients with chronic hepatitis. They concluded that HA could be a non- invasive index that shows the extent of liver fibrosis [23]. In our study also, we found that serum HA level increases proportionally with the severity of liver fibrosis in patients with chronic hepatitis B and C. Currently liver biopsy is accepted as the gold standard; but we concluded that HA could be an important non-invasive serum marker for the detection of the extent of liver fibrosis and evaluation of treatment response in patients, who will undergo biopsy repeat or in whom liver biopsy could not be performed.
References
-
Mohammed NA, El-Aleem SA, El-Hafiz HA, McMahon RFT (2004) Distribution of constitutive (COX-1) and inducible (COX-2) cyclooxygenase in postviral human liver cirrhosis: a possible role for COX-2 in the pathogenesis of liver cirrhosis. J Clin Pathol 57: 350- 354.
-
Bağcı S (2005) Karaciğer Fibrozisinde Tanı Metodları. Türkiye Klinikleri J Int Med Sci 1(16): 29-43
-
Rockey DC, Bissell DM (2006) Noninvasive Measures of liver fibrosis Hepatology 43: S113-S120
-
Trinchet JC (1995) Clinical use of serum markers of fibrosis in chronic hepatitis. J Hepatol 22(2): 89-95.
-
Wong VS, Hughes V, Trull A, Wight DG, Petrik J, et al. (1998) Serum hyaluronic acid is a useful marker of liver fibrosis in chronic hepatitis C virus infection. J Viral Hepat 5: 187-192.
-
Jeffers LJ, Coelho-Little ME, Cheinquer H, Vargas C, Civantos F, et al. (1995) Procollagen-III peptide and chronic viral Chepatitis. Am J Gastroenterol 90: 1437- 1440.
-
Piccinino P, Sangelli E, Guisti G (1986) Complications following percutaneous Liver biopsy. A multicentere retrospektive study on 68,276 biopsies. J Hepatol 2(2): 165-173.
-
McGill DB, Rakela J, Zinsmeister AR, Ott BJ (1990) A21 year experience with major hemorrage after percutaneous liver biopsy. Gastroenterology 99: 1396-1400.
-
Maharaj B, Maharaj RJ, Leary WP, Cooppan RM, Naran AD, et al. (1986) Sampling variability and itsİnfluence on the diagnostic yield of percutaneous needle biopsy of the liver. Lancet 1(8480): 523-525.
-
Yılmaz F (2005) Karaciğer fibrozisi patolojisi. Türkiye Klinikleri J Int Med Sci 1(16): 21-28.
-
Fraser JR, Engstrom-Laurent A, Nyberg A, Laurent TC (1986) Removal of hyaluronic acid from the circulation in rheumatoid disease and primary biliary cirrhosis. J Lab Clin Med 107(1): 79-85.
-
Murata K, Ochiai Y, Akashio K (1985) Polydispersity of acidic glycosaminoglycan components in human liver and the changes at different stages in liver cirrhosis. Gastroenterology 89: 1248-1257.
-
Patel K, Lajoie A, Heaton S, Pianko S, Behling CA, et al. (2003) Clinical use of hyaluronic acid as a predictor of fibrosis change in hepatitis C. J Gastroenterol Hepatol 18: 253-257.
-
Nyberg A, Engstrom-Laurent A, Loof L (1988) Serum hyaluronate in primer Biliary cirrhosis-abiochemical marker for progressive liver damage Hepatology 8: 142-146.
-
Arhan M, Köksal AŞ, Yüksel O, Akdoğan M (2007) Karaciğer fibrozisinin değerlendirilmesinde Serum hyaluronik asit düzeyinin yeri. Türkiye klinikleri J Med Sci 27(1): 21-26.
-
Chen YP, Freng XR, Dai L, Zhang L, Hou JL (2004) Noninvazive diagnostic sceening of hepatic fibrosis in patients with chronic hepatitis B. Chin Med J 117(7): 1109-1012.
-
Guechot J, Laudat A, Loria A, Serfaty L, Poupon R, et al. (1996) Accuracy of hyaluronan and type III procollagen aminoterminal peptideserum assays as markers of liver fibrosis chronic viral hepatitis C evaluatedby ROC curve analysis. Clin Chem 42: 558- 563.
-
Rosenberg WM, Voelker M, Thiel R, Becka M, Burt M, et al. (2004) Serum markers detect the presence of liver fibrosis: A cohort study. Gastroenterology 127: 1704-1713.
-
Murawaki Y, Ikuta Y, Okamoto K, Koda M, Kawasaki H (2001) Diagnostic value of serum markers of connective tissue turnover for predicting histologialstaging and grading in patients with chronic hepatitis C. J Gastroenterol 36: 399-406.
-
Li F, Zhu CL, Zhang H, Huang H, Wei Q, et al. (2012) Role of hyaluronic acid and laminin as serum markers for predicting significant fibrosis in patients with chronic hepatitis B. Braz J Infect Dis 16(1): 9-14.
-
Olga Hılda Orasan, George Cıulei, Angela Cozma, Madalına Sava, Dan Lucian Dumitrascu (2016) Hyaluronic acid as a biomarker of fibrosis in chronic liver diseases of different Etiologies Clujul Med 89(1): 24-31.
-
Orasan OH, Iancu M, Sava M, Saplontai Pop A, Cozma A, et al. (2015) Non-invasive assessment of liver fibrosis in chronic viral hepatitis. Eur J Clin Invest Dec 45(12): 1243-1251.
-
Guechot J, Loria A, Serfaty L, Giral P, Giboudeau J, et al. (1995) Serum hyaluronan as a marker of liver fibrosis in chronic viral hepatitis C: Effect of-interferon therapy. J Hepatol 22(1): 22-26.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient