A Rare Case of Esophagitis Dissecans Superficialis “Sloughing Esophagitis”
Esophagitis dissecans superficialis (EDS) or sloughing esophagitis is a rare idiopathic condition and is often under-reported and under-recognized entity. It is characterized by strips of denuded esophageal mucosa with minimal or no bleeding. EDS was first described in 1892, since then, there have been only very few case reports. Herein, we illustrate a case report of this rare entity that may serve to remind us of this often forgotten condition.
Introduction
Esophagitis dissecans superficialis (EDS) or sloughing esophagitis is a rare, benign cryptogenic condition of the esophagus, characterized by exfoliated superficial esophageal mucosa. Histologically, it is characterized by desquamated superficial epithelium of the esophageal lining. EDS tend to be associated with polypharmacy in elderly debilitated patients [1]. Clinically, majority of patients are asymptomatic. Most EDS are detected in the distal or mid-esophagus, however up to 23% EDS affect the entire esophagus [1]. The etiology of this condition remains unclear, although several exogenous agents such as chemical or corrosive irritants have been implicated to explain the denuded esophageal mucosa suggestive of possible contact injury rather than ischemia. This case report illustrates a debilitating patient who was diagnosed with EDS.
Case
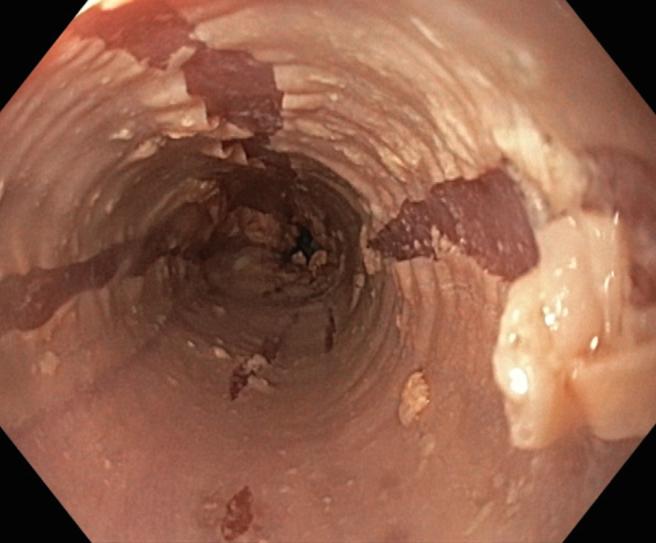
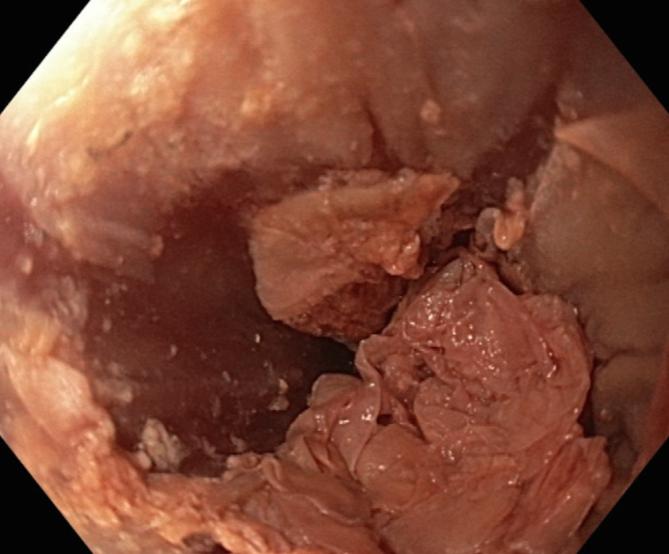
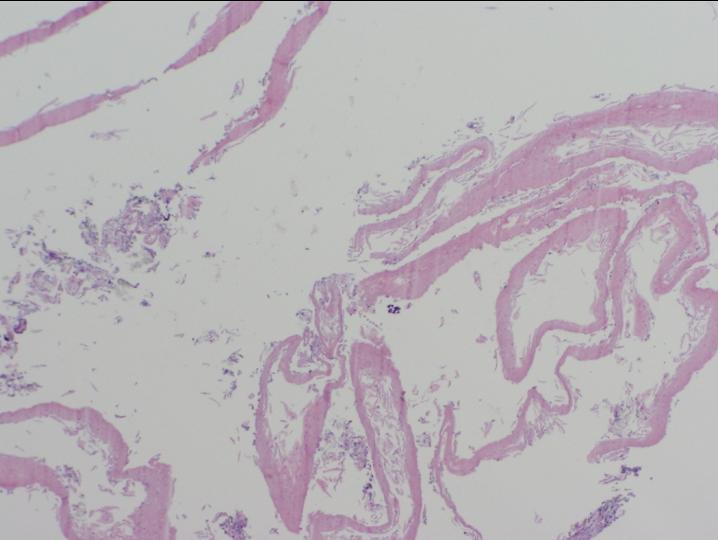
A 68 year-old man with a history of neurodegenerative disease, major depression and malnutrition was admitted with weight loss. He had no prior symptoms of dysphagia, nausea and vomiting. The patient also had no reported skin-related symptoms or associated autoimmune conditions. His regular medications included benzodiazepine, aspirin and multivitamins. Clinically, he appeared frail with no other significant findings. Esophagogastroduodenoscopy (EGD) was performed, which revealed streaks of peeled desquamated esophageal mucosa with circumferential cracks and long linear mucosa break (Figure 1). The lower third of the esophagus revealed clumps of exfoliated esophageal mucosa (Figure 2). Biopsies were taken from the proximal esophagus, histopathology of which was reported as superficial disaggregated epithelium that is entirely separated from the underlying squamous mucosa (Figure 3). These endoscopic appearances were consistent with esophagitis dissecans superficialis (EDS), also known as sloughing esophagitis. The patient was treated with oral proton pump inhibitor (pantoprazole 40 mg daily) for a week. A follow-up EGD showed complete normalization of the esophageal mucosa.
Discussion
Esophagus Dissecans Superficialis (EDS) was first reported in 1892 [2]. It is a rare and benign condition, also known as sloughing esophagitis and is an under- recognized entity whereby its prevalence or incidence rate is largely unknown [3]. EDS is characterized by strips of detached superficial mucosa but can present as vertical fissures, circumferential or long linear mucosal breaks in the esophagus and tends to be associated with minimal or no bleeding [4]. Patients are mostly asymptomatic, but some may report symptom of dysphagia and very rarely, vomit out casts of esophageal mucosa [5][6]. Histologically, there is superficial eosinophilic, necrotic squamous epithelium that is either partially or completely detached from the underlying epithelium. This endoscopic finding is most often seen in debilitated or malnourished elderly patients such as in our patient and who are typically on multiple (at least 5) medications including central nervous system depressants [1]. The pathogenesis is virtually unknown and is most often idiopathic. However, EDS has been linked to various forms of esophageal mucosal injury that includes iatrogenic, chemical, thermal, immunological or allergic reaction. Based on the reported cases linking EDS to nonsteroidal anti-inflammatory, bisphosphonate, consumption of hot beverages, heavy smoking, mediastinal radiation, endoscopic therapy (sclerotherapy, esophageal dilatation and band ligation), autoimmune bullous dermatoses, lichen planus, celiac disease and cardiac disease (valvular or congestive heart failure) [7, 8, 9, 10]. Diseases such as monilial esophagitis, eosinophilic esophagitis (EoE) and corrosive esophagitis may mimic EDS, hence emphasizing the need for esophageal biopsy [2]. Despite the dramatic endoscopic appearance, sloughing esophagitis, complete resolution of mucosal injury is usually achieved without any long-lasting clinical consequences through combination of acid suppression and discontinuation of the precipitating factors and medications. In the setting of bullous dermatoses, steroid therapy may be required for mucosal healing [9].
Conclusion
In summary, EDS remains an enigma to many health professionals where the etiology is largely unknown and is characterize by its dramatic endoscopic appearance and complete resolution with no long-term sequelae.
Conflict of Interest declaration
Author has no conflict or financial interest related to this article.
References
-
Purdy JK, Appelman HD, McKenna BJ (2012) Sloughing esophagitis is associated with chronic debilitation and medications that injure the esophageal mucosa. Mod Pathol 25(5): 767-775.
-
Rosenberg B (1892) Oesophagitis dissecans superficialis. Centralbl Allg Pathol Path Anat 3: 753- 759.
-
Carmack SW, Vemulapalli R, Spechler SJ, Genta RM (2009) Esophagitis dissecans superficialis (sloughing esophagitis): a clinicopathologic study of 12 cases. Am J Surg Pathol 33(12): 1789-1794.
-
De S, Williams GS (2013) Esophagitis dissecans superficialis: a case report and literature review. Can J Gastroenterol 27(10): 563-564.
-
Cesar WG, Barrios MM, Maruta CW, Aoki V, Santi GG (2009) Oesophagitis dissecans superficialis: An acute, benign phenomenon associated with pemphigus vulgaris. Clin Exp Dermatol 34(8): e614-616.
-
Ponsot P, Molas G, Scoazec JY, Ruszniewski P, Hénin D (1997) Chronic esophagitis dissecans: an unrecognized clinicopathologic entity. Gastrointest Endosc 45(1): 38-45.
-
Lin DE, Vanagunas A (2000) Esophagitis dissecans superficialis: a case series. Am J Gastroenterol 95: 24- 26.
-
Longman RS, Remotti H, Green PH (2011) Esophagitis dissecans superfialis. Gastrointest Endosc 74: 403- 404.
-
Hokama A, Yamamoto Y, Taira K, Nakamura M, Kobashigawa C, et al. (2010) Esophagitis dissecans superficialis and autoimmune bullous dermatoses: A review. World J Gastrointest Endosc 2(7): 252-256.
-
Cardoso Figueiredo P, Pinto-Marques P, Neta J, João Freitas (2014) Esophagitis dissecans superficialis. GE J Port Gastrenterol 21: 123-124.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient