Progression of AA Amyloidosis (Sequence of Amyloid A Deposition) in the Pancreas - A Postmortem Clinicopathologic Study of 161 Patients
The aim of our study was to determine the prevalence and severity of systemic AA amyloidosis (sAAa) in rheumatoid arthritis (RA), to specify amyloid A deposits in different tissue structures of the pancreas, to outline the development of pancreatic AA amyloidosis (pAAa), and to estimate the role of sAAa and pAAa in mortality. Patients and Methods: At the National Institute of Rheumatology 9475 patients died between 1969 and 1992; among them 161 with RA and all of them were autopsied. RA was confirmed clinically according to the criteria of the American College of Rheumatology (ACR). sAAa was specified histologically, based on evaluation of 5 organs (heart, lung, liver, kidney and pancreas). Tissue samples of pancreas were available for histologic evaluation in 118 of 161 patients. Amyloid A deposition was diagnosed according to Romhányi. The correlations between different patient cohorts were determined by the Student (Welch) t-probe. Results: sAAa complicated RA in 29 (24.58 %) of 118 patients. sAAa was histologically excluded in 89 (75.42 %) of 118 RA patients. The pancreas was involved in 26 (89.66 %) of 29 patients. Amyloid A deposits were not present in the pancreas in 3 (10.34 %) of 29 RA patients with sAAa. sAAa or pAAa complicated RA in both sexes, and at any time in the course of the disease. Discussion and Conclusion: Systemic AAa is one of the main and most insidious complications of rheumatoid arthritis affecting the pancreas with high prevalence and severity. sAAa is related to the cardiovascular system, and pAAa is connected with it. In sAAa the amyloid A deposition in the pancreas starts after a latent stage. Systemic and pancreatic amyloid a deposition is a progressive and cumulative process, involving in its early stage only a few structures in the pancreas, and increasingly more in later stages of the disease. Amyloid a deposition starts in the most frequently involved structures of the pancreas with more massive deposits. The chronology of amyloid A deposition allows an indirect assessment of the stage of pancreatic amyloidosis, which may have a prognostic value in everyday surgical pathology as well.
Introduction
Amyloidosis is a systemic or localized disorder characterized by the extracellular deposition of chemically heterogeneous fibrillar protein [1]. Several diseases or disorders may be complicated by systemic or localized deposition of amyloid proteins [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12]. Different systemic types of amyloidosis (secondary AA, primary myeloma-associated or B-cell dyscrasia related, senile, etc.) or organ (tissue)-limited localized form of amyloidosis (cerebral, dystrophic, endocrine related such as islet amyloid polypeptide localized to the islets of Langerhans, etc..) may exist simultaneously in patients with rheumatoid arthritis (RA). Only systemic AA amyloidosis (sAAa) may be considered as a true complication of RA, any other types of amyloidosis may be present in RA as an associated phenomenon or complication of associated diseases [13].
The aim of our study was to determine the prevalence and severity of sAAa in RA, to specify amyloid A deposits in different tissue structures of the pancreas, to outline the development of pancreatic AA amyloidosis (pAAa), and to estimate the role of sAAa and pAAa in mortality.
Patients (Autopsy Population) and Methods
At the National Institute of Rheumatology 9475 patients died between 1969 and 1992; among them 161 with RA (females 116, average age: 64.95 years, range 87- 16, onset of RA: 50.19, average disease duration: 14.79 years; males 45, average age: 66.29 years, range 88-19, onset of RA: 52.57, average disease duration: 13.46 years at death); all of them were autopsied [13].
RA was confirmed clinically according to the criteria of the American College of Rheumatology (ARA) [14]. sAAa was specified histologically, based on evaluation of 5 organs (heart, lung, liver, kidney and pancreas). Tissue samples of pancreas were available for histologic evaluation in 118 of 161 patients.
Amyloid A deposition was diagnosed according to Romhányi by a modified (more sensitive) Congo red staining [15, 16]. Amyloid A deposits were identified in serial sections by immunohistochemistry and histochemistry methods [17, 18]. The prevalence (existence) and severity (extent) of amyloid A deposition were evaluated microscopically with an Olympus BX51 polarizing microscope [13].
Glossary of Definitions
"Prevalence" concerns the presence of amyloid A in blood vessels of different calibers or in different tissue structures of the pancreas. Size of blood vessels in tissue samples [branches of splenic artery, upper and lower gastroduodenal arteries] [19]. a. Arteriole (a) – no internal or external elastic membrane, 500 micrometers in diameter b. Small artery (A) – only internal elastic membrane present, vessels 500-1000 micrometers in diameter c. Medium size artery (AA) – internal and external elastic $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ membrane are present – vessel diameter d. Venule (v), small vein (V), medium size vein (VV) – accompanying (a), (A) or (AA) e. Interstitial collagen fiber (I) – in peripancreatic or pancreatic localization f. reticulin fiber (collagen IV) (ret) – in peripancreatic or pancreatic fat tissue g. basement membrane of pancreatic ducts (BM) h. nerve (n) in the pancreas "Severity" indicates varying amounts of amyloid A deposition in different tissue structures. Severity of amyloidosis was evaluated by semi-quantitative visual estimation on a 0 to 3 plus scale (based on the number of involved vessels and tissue structures/light microscopic field x40 lens of Olympus BX51).
Semi-Objective Score System of “Severity”
The correlations were determined by the Student (Welch) t-probe comparing the age, sex of patients, onset of RA, and duration of disease at the time of death with and without sAAa or pAAa, and with “mild” (amyloid A deposits / patient < 1.0) and “severe” (amyloid A deposits / patient 1.0 ≤) pAAa [20].
Results
- tissue structures c. “2” – less than five involved tissue structures d. “3” – five or more involved tissue structures
- Remark
- In case of AA or VV this corresponds to the absolute number of involved medium size vessels of a tissue sample, e.g. “0” none, “1” only one,“2” less than five, “3” 5 or more than five medium size vessels/tissue sample with a x20 objective lens.
- Sex
- Number of
- Mean age in years at
- Range (in years)
- Mean age at onset
- Disease duration
- (in years) mean ±SD
- RA patients
- 118
- 64.97±12.84
- 16– 88
- 51.44±16.80
- 13.84±10.40
- Female
- 80
- 64.41±11.95
- 16 – 87
- 50.75±15.03
- 13.84±10.43
- Male
- 38
- 66.13±14.48
- 19 – 88
- 53.03±20.20
- 13.29±10.31
- With sAAa
- 29
- 62.14±15.30
- 19 – 88
- 47.59±16.66
- 15.59±9.35
- Female
- 24
- 64.42±9.34
- 44 – 82
- 48.70±12.66
- 15.74±9.96
- Male
- 5
- 51.20±28.18
- 19 – 88
- 41.25±30.07
- 14.75±4.44
- Without sAAa
- 89
- 65.90±11.79
- 16 – 87
- 52.83±16.64
- 13.21±10.68
- Female
- 56
- 64.41±12.90
- 16 – 87
- 51.73±15.95
- 13.29±10.55
- Male
- 33
- 68.39±9.07
- 52 – 87
- 54.78±17.63
- 13.07±10.89
- With pAAa
- 26
- 61.96±15.47
- 19 – 88
- 47.88±16.86
- 15.25±9.07
- Female
- 21
- 64.52±8.55
- 44 – 82
- 49.20±12.24
- 15.35±9.74
- Male
- 5
- 51.20±28.18
- 19 – 88
- 41.25±30.07
- 14.75±4.44
- Without pAAa
- 3
- 63.33±13.60
- 50 – 82
- 44.67±14.29
- 18.67±10.66
- Female
- 3
- 63.33±13.60
- 50 – 82
- 44.67±14.29
- 18.67±10.66
- Male
- 0
- -
- -
- -
- -
- Severe pAAa (1.0£)
- 12
- 58.33±16.22
- 19 – 82
- 39.36±15.33
- 18.45±8.28
- Female
- 9
- 62.67±6.11
- 54 – 73
- 43.38±7.05
- 19.13±9.40
- Male
- 3
- 45.33±26.74
- 19 – 82
- 28.67±23.92
- 16.67±3.40
- Mild pAAa (>1.0)
- 14
- 65.14±14.07
- 32 – 88
- 55.23±14.59
- 12.46±8.86
- Female
- 12
- 66.00±9.75
- 44 – 82
- 53.25±13.40
- 12.75±9.17
- Male
- 2
- 60.00±28.00
- 32 – 88
- 79.00±00.00
- 9.00±00.00 autopsies death ± SD of disease ± SD
Table 1: Sex, mean age with SD, range, onset and disease duration of RA patients with (n=29) or without sAAa (n=89),
Comparing the age, sex, onset of RA, and duration of disease at the time of death there was no significant difference between female (p< 0.99, p< 0.38, p< 0.35) and male (p< 0.29, p< 0.50, p< 0.63) RA patients with sAAa (p< 0.24, p< 0.17, p< 0.28) and without sAAa.
The age, sex of RA patients and onset of disease did not influence the amyloid A deposition in the pancreas; there was no significant difference between female (p< 0.82, p< 0.23, p< 0.43) and male (p< 0.82, p< 0.63, p< 0.61) RA patients with sAAa (p< 0.51, p< 0.20, p< 0.37) and pAAa.
The mean age of RA patients, complicated by severe pAAa was lower at onset of RA compared to those with mild pAAa (39.4 years versus 55.2); this difference was significant (p< 0.02).
sAAa or pAAa complicated RA in both sexes, and at any time in the course of the disease. The risk of severe pAAa was higher at early onset of RA.
The quantitative differences of amyloid A deposits in 5 organs of 29 of 118 RA patients are summarized in Table 2, Figures 1 & 2.
| f/m | Pr n0/y | Heart | Kidney | Pancr | Liver | Lung | Avg | CoD | Cl+/- | |
| 1 | f | 155/87 | 0,000 | 0,000 | 0,000 | 0,000 | 0,083 | 0,017 | ||
| 2 | f | 240/88 | 0,000 | 0,000 | 0,100 | 0,000 | 0,000 | 0,020 | ||
| 3 | f | 243/87 | 0,400 | 0,000 | 0,100 | 0,000 | 0,000 | 0,100 | cAAa | |
| 4 | f | 287/91 | 0,500 | 0,083 | 0,400 | 0,000 | 0,000 | 0,197 | cAAa | |
| 5 | f | 183/92 | 0,000 | 0,667 | 0,500 | 0,111 | 0,000 | 0,256 | ||
| 6 | f | 226/85 | 0,600 | 0,417 | 0,200 | 0,111 | 0,167 | 0,299 | ||
| 7 | f | 430/80 | 0,400 | 0,417 | 0,400 | 0,111 | 0,167 | 0,299 | cAAa | |
| 8 | f | 395/76 | 1,200 | 0,250 | 0,000 | 0,111 | 0,167 | 0,346 | cAAa | |
| 9 | f | 162/78 | 1,100 | 0,083 | 0,550 | 0,111 | 0,000 | 0,369 | ||
| 10 | f | 306/90 | 0,800 | 0,750 | 0,400 | 0,000 | 0,488 | rAAa-U | Cl+ | |
| 11 | f | 45/74 | 1,400 | 0,000 | 0,800 | 0,444 | 0,000 | 0,529 | cAAa | |
| 12 | m | 342/86 | 1,100 | 0,750 | 0,300 | 0,333 | 0,250 | 0,547 | rAAa-U | |
| 13 | f | 52/92 | 1,000 | 0,667 | 0,650 | 0,000 | 0,750 | 0,613 | ||
| 14 | f | 322/81 | 0,700 | 0,833 | 1,000 | 0,556 | 0,167 | 0,651 | cAAa | |
| 15 | f | 203/88 | 1,000 | 0,667 | 0,700 | 0,167 | 0,750 | 0,657 | rAAa-U | |
| 16 | f | 39/76 | 0,400 | 1,500 | 1,200 | 0,667 | 0,333 | 0,820 | rAAa-U | |
| 17 | f | 90/85 | 1,400 | 0,917 | 0,100 | 1,778 | 0,000 | 0,839 | ||
| 18 | f | 265/80 | 1,400 | 1,500 | 0,000 | 0,889 | 0,417 | 0,841 | rAAa-U | Cl+ |
| 19 | f | 245/88 | 1,500 | 1,000 | 1,100 | 0,556 | 0,250 | 0,881 | cAAa | |
| 20 | m | 232/74 | 1,300 | 1,833 | 0,600 | 1,000 | 0,333 | 1,013 | rAAa-U | Cl+ |
| 21 | f | 367/75 | 0,900 | 2,167 | 1,400 | 0,778 | 0,333 | 1,116 | cAAa | |
| 22 | m | 43/85 | 1,000 | 1,083 | 1,350 | 1,222 | 1,167 | 1,164 | rAAa-U | |
| 23 | f | 137/76 | 1,400 | 1,583 | 1,000 | $\cdot$ | 0,917 | 1,225 | rAAa-U | Cl+ |
| 24 | f | 73/87 | 1,600 | 1,417 | 1,300 | 1,111 | 0,833 | 1,252 | rAAa-U | Cl+ |
| Count | 29 | 29 | 29 | 27 | 29 | 34 | 22 | 8 | |
| Sum | 29,90 | 29,09 | 24,40 | 16,17 | 12,67 | 26 | |||
| Avg | 1,031 | 1,003 | 0,841 | 0,599 | 0,437 | 0,786 | |||
| 0 values n | 3 | 4 | 3 | 5 | 8 | 1 | |||
| + values n | 26 | 25 | 26 | 22 | 21 | 33 | |||
| SD | 0,605 | 0,778 | 0,724 | 0,579 | 0,464 | 0,537 | |||
| Prevalence % | 89,655 | 86,207 | 89,655 | 81,481 | 72,414 | 97,060 | |||
| Severity% | 34,368 | 33,431 | 28,046 | 19,960 | 14,561 | 25,650 | |||
| Heart | Kidney | Pancr | Liver | Lung | Avg | CoD | Cl+/- |
Table 3: Average amount of amyloid A deposits in different organs of 29/118 RA patients with sAAa arranged according Table 2: Ave
Table 2: Average amount of amyloid A deposits in different organs of 29/118 RA patients with sAAa arranged according Table 2: Average amount of amyloid A deposits in different organs of 29/118 RA patients with sAAa arranged according to the increasing values of average amounts of amyloid A deposits/patient (horizontal lines) and amyloid A deposits/organ (vertical columns). Remarks to Table 2 Pr n /year –number of autopsy protocol / year CoD: Cause of death: rAAa-U – Uremia due to massive amyloid A deposition in the kidneys with consecutive renal insufficiency (n=14), cAAa – lethal outcome exclusively caused by cardiac amyloidosis (n=3); cAAa – contribution of cardiac amyloidosis to the death (n=5) Cl+: Clinically recognized – Cl- : Clinically not recognized f: female, m: male Avg – Average SD – Standard Deviation * – tissue blocks were not available Amyloid a deposition in the pancreas compared to other organs of RA patients is demonstrated on Figure 1.
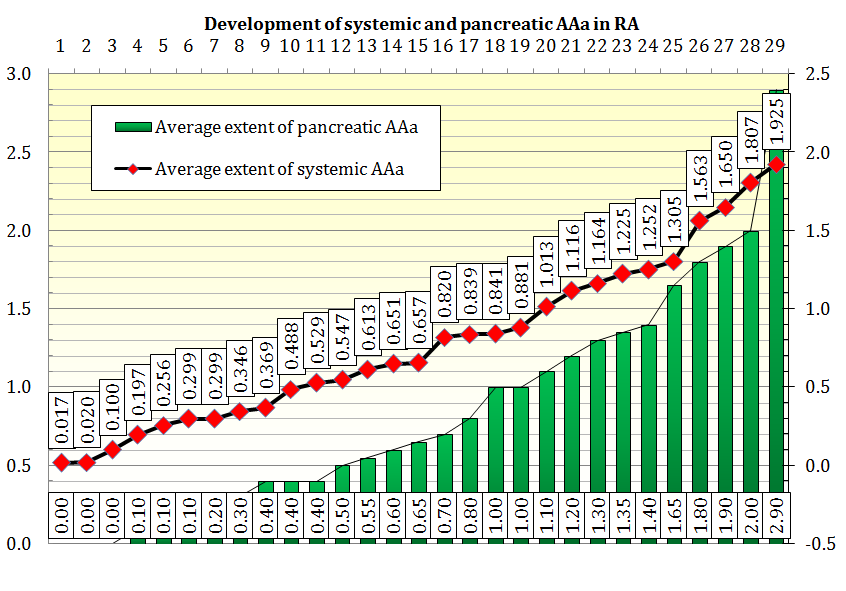
Cohort of 29 RA patients with systemic and pancreatic AAa at death, according to increasing values of amyloid A deposits ("average amount of amyloid A deposits/patient").
The systemic amyloid A deposition showed a basically a linear growth curve.
The amount of amyloid a deposits in pancreas increased gradually and showed basically a lineal growth curve like the systemic amyloid A deposition. The advanced stage of pAAa was characterized by an intensive amyloid A deposition, and the late (terminal) stage by an abrupt increment of amyloid A in the pancreas.
The quantitative differences of amyloid A deposits in the pancreas (n=26) of 29 RA patients are summarized in Table 3 and Figures 2 & 4.
| Sex | a | A | ret | VV | AA | V | I | v | BM | n | Avg | CoD | Cl+/- | ||
| 1 | 395/76 | f | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,00 | cAAa | |
| 2 | 265/80 | f | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,00 | rAAa-U | Cl+ |
| 3 | 155/87 | f | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,00 | ||
| 4 | 90/85 | f | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0,10 | ||
| 5 | 243/87 | f | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,10 | cAAa | |
| 6 | 240/88 | f | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,10 | ||
| 7 | 226/85 | f | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,20 | ||
| 8 | 342/86 | m | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,30 | rAAa-U | |
| 9 | 430/80 | f | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0,40 | cAAa | |
| 10 | 306/90 | f | 2 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0,40 | rAAa-U | Cl+ |
| 11 | 287/91 | f | 2 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0,40 | cAAa | |
| 12 | 183/92 | f | 2 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0,50 | ||
| 13 | 162/78 | f | 2 | 1,5 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,55 | ||
| 14 | 232/74 | m | 3 | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0,60 | rAAa-U | Cl+ |
| 15 | 52/92 | f | 2 | 1 | 1 | 1 | 0 | 0,5 | 1 | 0 | 0 | 0 | 0,65 | ||
| 16 | 203/88 | f | 2 | 1 | 0 | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0,70 | rAAa-U | |
| 17 | 45/74 | f | 3 | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0,80 | cAAa | |
| 18 | 137/76 | f | 3 | 3 | 2 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1,00 | rAAa-U | Cl+ |
| 19 | 322/81 | f | 3 | 2,5 | 0 | 2 | 2,5 | 0 | 0 | 0 | 0 | 0 | 1,00 | cAAa | |
| 20 | 245/88 | f | 3 | 3 | 0 | 1 | 1 | 2 | 0 | 1 | 0 | 0 | 1,10 | cAAa |
| + values n | 23 | 20 | 17 | 15 | 13 | 13 | 13 | 7 | 3 | 2 | 26 | ||
| Prevalence in % | 79,3 | 69 | 58,6 | 51,7 | 44,8 | 44,8 | 44,8 | 24,1 | 10,3 | 6,9 | 89,7 | ||
| Extent in % | 66,1 | 52,3 | 32,2 | 30,5 | 29,3 | 25,3 | 21,8 | 12,6 | 5,7 | 4,6 | 28,0 | ||
| Sex | a | A | ret | VV | AA | V | I | v | BM | n | Avg | Cl+/- |
Table 5: Prevalence and extent of amyloid A deposits in different tissue structures of the pancreas according to increasing Table
Table 3: Prevalence and extent of amyloid A deposits in different tissue structures of the pancreas according to increasing Table 3: Prevalence and extent of amyloid A deposits in different tissue structures of the pancreas according to increasing values of average amounts of amyloid A deposits/patient (horizontal lines) and A deposits/structure (vertical columns). Remarks to Table 3 Pr n /year –number of autopsy protocol / year CoD: Cause of death: rAAa-U – Uremia due to massive amyloid A deposition in the kidneys with renal insufficiency (n=14), cAAa – lethal outcome exclusively caused by cardiac amyloidosis (n=3), cAAa – contribution of cardiac amyloidosis to the death (n=5), the patients died due to circulatory failure, myocardial necrosis caused by coronary vasculitis of autoimmune origin or atherosclerosis Assoc dis – Associated diseases: aRecLnP – acute relapsing liponecrotic pancreatitis (n=2), or chrLnP – chronic liponecrotic pancreatitis (n=2) associated with pancreatic amyloidosis contributed to the death only; the patients died of uremia due to massive renal amyloidosis Cl+: Clinically recognized – Cl- : Clinically not recognized f: female, m: male SD – Standard Deviation Abbreviations (a): Arteriole; (A): Small Artery; (AA): Medium Size Artery; (v): Venule; (V): Small Vein; (VV): Medium Size Vein; (I): Interstitial Collagen Fiber; (Collagen IV): Reticulin Fiber (ret); (BM): Ductal Basement Membrane; (n): Nerve The distribution of amyloid A in the pancreas (according to increasing values of amyloid A deposits) is demonstrated in Figures 1 & 2.
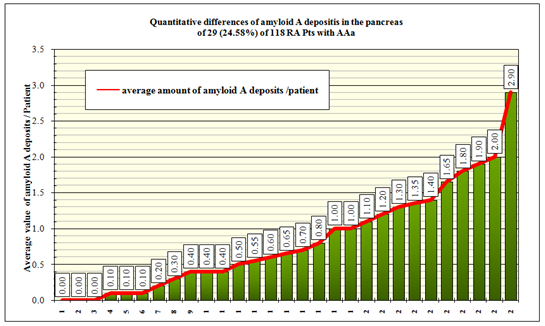
Cohort of 29 RA patients with or without amyloid A deposition in the pancreas at death, according to increasing values of amyloid A deposits ("average amount of amyloid A deposits/patient") In the pancreas amyloid A deposition started later than general (systemic) amyloid deposition, and increased gradually. The accumulation of amyloid A deposits in the pancreas with mild and severe amyloidosis showed basically a lineal growth curve, except at the end stages of amyloid deposition. At the terminal stage a rapid progression was characteristic, and the growth curve of amyloid A deposition displayed an exponential increment Figure 3.
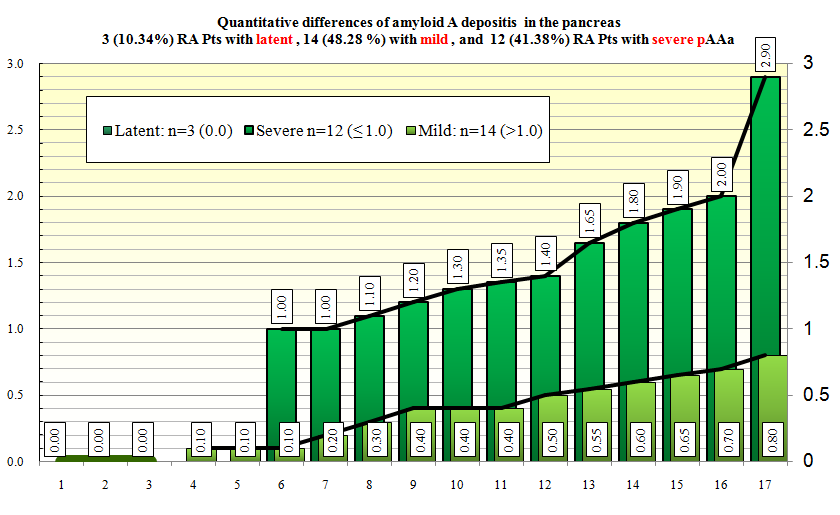
In 3 (10.34 %) of 29 RA patients with sAAa there was no amyloid A deposition in the pancreas, these represent a latent stage of pancreatic amyloidosis (the amount of amyloid A deposits was: 0.00); in 14 (48.28 %) of 29 patients the amount of amyloid A deposits was “mild” (>1.0), and in 12 (41.38 %) it was “severe” (≤ 1.0). The increment showed a basically a linear growth curve. The late stage of AAa was characterized by abrupt (intensified) deposition, and the increment was exponential in this terminal stage of pAAa.
The frequently involved tissue structures showed marked deposits of amyloid. Deposits were less striking in less frequently involved tissue structures Table 3 & Figure 4.
Regarding the regional distribution of amyloid A
deposits in the pancreas, besides the constant involvement of blood vessels Figures 6-7ac & 8ab, the relatively massive involvement of reticulin and collagen fibers was characteristic Figures 9-12ab. Amyloid A deposition was minimal in the periductal basement membranes Figures 6-7ac or peripheral nerves Figures 8ab.
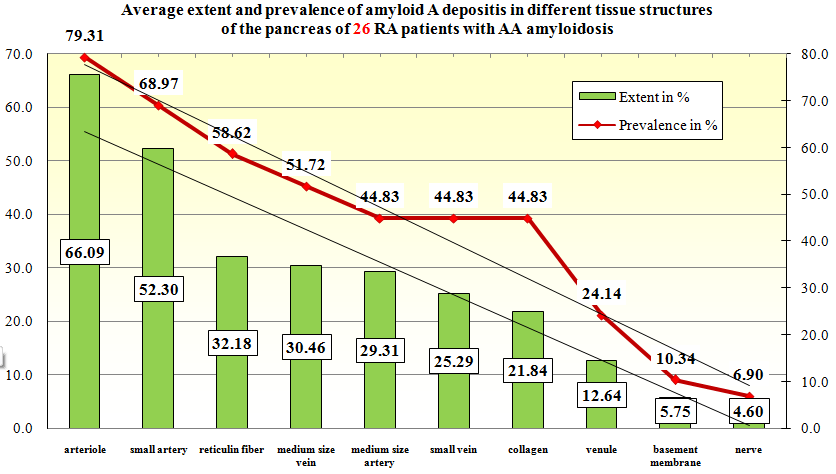
The prevalence and extent of amyloid A deposits in different tissue structures of the pancreas were running basically parallel Detectable amounts of amyloid A deposits on different tissue structures of the pancreas did not appear simultaneously. In the early stage of systemic amyloidosis there were histologically detectable amyloid deposits only in a few structures (arterioles, small arteries, reticulin fibers). In other structures of the pancreas (medium size veins and arteries, small veins, interstitial collagen fibers The amount of deposited amyloid A was different in various tissue structures and increased simultaneously, but the proportion of deposited amyloid A was nearly constant and independent of the stage of amyloidosis. The amounts of amyloid A deposits in various structures of the pancreas are demonstrated in Figure 5.
venules) in advanced stage, and in periductal basement membranes or nerves deposits were seen only in late stages of amyloidosis (with massive involvement of the former) (Figure 5).
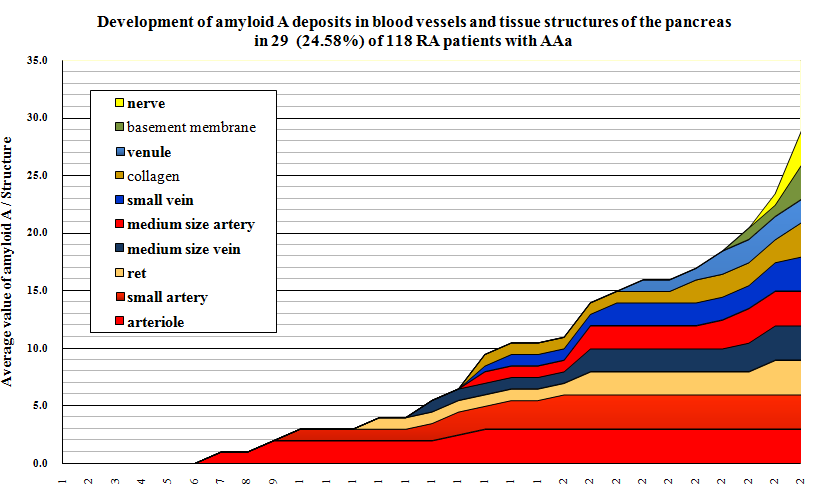
The amount of amyloid A deposits in blood vessels and in different tissue structures of the pancreas are arranged according to their decreasing severity.
Amyloid A deposition did not start at the same time in different tissue structures of the pancreas. The amount of amyloid deposits in different tissues increased simultaneously, the rate was constant and independent of the stage of amyloidosis.
The basic disease, complication(s) and cause of death of 29 (24.57 %) of 118 RA patients with sAAa is summarized in Table 4.
Pancreatic amyloidosis was associated with acute relapsing lipionecrotic pancreatitis (aRecLnP) in 2 (6.89 %), and with chronic lipionecrotic pancreatitis (chrLnP) in further 2 (6.89 %) of 29 RA patients. Pancreatic amyloidosis or aRecLnP and chrLnP had no direct role in mortality; the patients died of uremia due to massive amyloid A deposition in the kidneys (aRecLnP and chrLnP due to pAAa contributed to the death only) (Table 4).
| Associated | Pr n0/ | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Basic disease | Complication 1 | Complication 2 | Cause of death | Cl+/Cl- | |||||||||||||||||
| disease(s) | year | ||||||||||||||||||||
| 1 | RA-sAAa | Coronary arteritis- arteriolitis | A-SV | Myocardiocytolysis- cAAa | TbFc-mTb | Cl- | 395/76 | ||||||||||||||
| 2 | RA-sAAa | rAAa-U | Ca of pancreas | Cl+ | 265/80 | ||||||||||||||||
| 3 | RA-sAAa | Ependymoma | Vertebral fracture | Pulmonary embolism | RA-Ath-Hy | Cl- | 155/87 | ||||||||||||||
| 4 | RA-sAAa | A-SV | Myocardial necrosis | Ath-DM | Cl- | 90/85 |
| 5 | RA-sAAa | Coronary arteritis- arteriolitis | A-SV | Circulatory failure-cAAa | Cl- | 243/87 | |
|---|---|---|---|---|---|---|---|
| 6 | RA-sAAa | Coronary arteriolitis | A-SV | Myocardiocytolysis | Tb-F-mTb | Cl- | 240/88 |
| 7 | RA-sAAa | Sporadic mTu Vasculitis* | Pneumonia | Ca Bralveolare- Ath | Cl- | 226/85 | |
| 8 | RA-sAAa | rAAa-U | Ac Neurinom-Ath | Cl- | 342/86 | ||
| 9 | RA-sAAa | Circulatory failure-cAAa | Ca of gallbladder | Cl- | 430/80 | ||
| 10 | RA-sAAa | rAAa-U | Cl+ | 306/90 | |||
| 11 | RA-sAAa | Nodular epicarditis | Myocardial necrosis- cAAa | Operated breast Ca | Cl- | 287/91 | |
| 12 | RA-sAAa | Colitis-Colonic ulcers | Peritonitis | Lethal SI | Cl- | 183/92 | |
| 13 | RA-sAAa | Gastric ulcer-Bleeding- Opus | Perforation- Peritonitis | Lethal SI | Cl- | 162/78 | |
| 14 | RA-sAAa | ChrLnP | rAAa-U | Cl+ | 232/74 | ||
| 15 | RA-sAAa | Hypertension | Myocardial fibrosis | Bronchopneumonia | RA | Cl- | 52/92 |
| 16 | RA-sAAa | Femoral vein thrombosis | rAAa-U | Cl- | 203/88 | ||
| 17 | RA-sAAa | Heart failure-cAAa | Cl- | 45/74 | |||
| 18 | RA-sAAa | ChrLnP | rAAa-U | Cl+ | 137/76 | ||
| 19 | bTu-sAAa | Circulatory failure-cAAa | Cl- | 322/81 | |||
| 20 | RA-sAAa | Bronchiolitis obliterans | Multifocal pneumonia | Heart failure- cAAa | DM | Cl- | 245/88 |
| 21 | RA-sAAa | rAAa-U | Ath | Cl- | 39/76 | ||
| 22 | RA-sAAa | rAAa-U | Cl+ | 73/87 | |||
| 23 | RA-sAAa | aRecLnP | A-SV | rAAa-U | DM- Hy | Cl- | 43/85 |
| 24 | RA-sAAa | Myocardial necrosis- cAAa | Ath-DM | Cl- | 367/75 | ||
| 25 | RA-sAAa | aRecLnP | rAAa-U | DM | Cl+ | 255/83 | |
| 26 | RA-sAAa | rAAa-U | Cl- | 174/88 | |||
| 27 | RA-sAAa | rAAa-U | Cl+ | 53/87 | |||
| 28 | RA-sAAa | rAAa-U | Hy | Cl- | 101/90 | ||
| 29 | RA-sAAa | rAAa-U | Neurinom | Cl+ | 181/80 |
Table 7: Mortality of sAAa in 29 of 118 RA patients according to increasing average amounts of amyloid A deposits in Table 4: Mor
Table 4: Mortality of sAAa in 29 of 118 RA patients according to increasing average amounts of amyloid A deposits in Table 4: Mortality of sAAa in 29 of 118 RA patients according to increasing average amounts of amyloid A deposits in pancreas/patient (horizontal lines). Remarks to Table 4 Basic disease: underlying disease related to death. Complication: consequence of basic disease leading directly to death. Associated (Accompanying) disease: important disorder without direct causal role in death. Pr n /year –number of autopsy protocol / year sAAa – systemic AAa CoD: Cause of death: rAAa-U – Uremia due to massive amyloid A deposition in the kidneys with renal insufficiency (n=17), cAAa – lethal outcome exclusively caused by cardiac amyloidosis (n=3); cAAa – contribution of cardiac amyloidosis to the death (n=5). aRecLnP – acute recidieve liponecrotic pancreatitis (n=2), or chrLnP – chronic liponecrotic pancreatitis (n=2) associated with pancreatic amyloidosis contributed to the death only; the patients died by uremia due to massive renal amyloidosis. Cl+: – Clinically recognized AAa in 8 (27.59 %) of 29 patients Cl- : – Clinically not recognized 21 (72.41 %) of 29 patients *sporadic vasculitis associated with carcinoma (Ca) bTu: – benign tumor (ependymom) SI – lethal septic infection A-SV: – systemic vasculitis of autoimmune origin SI: – lethal septic infection Ath: – Atherosclerosis Hy: – Hypertension Tb – Post-primary (Fc – fibrocaseous, F – fibrous) tuberculosis mTb –miliary disseminated Tb DM – adult type II diabetes mellitus Ca – carcinoma; Ca of pancreas associated with RA without direct role in mortality Myocardiocytolysis – Multiple (multifocal) microinfarction of myocardium Figures 6-12 represent different (early and advanced) stages of pAA.
transparency slide the correct height: width ratio is 2:3. The printed size may be different; therefore it is necessary to indicate the original magnifications corresponding to a fixed size.
Original magnifications correspond to the 24x36 mm
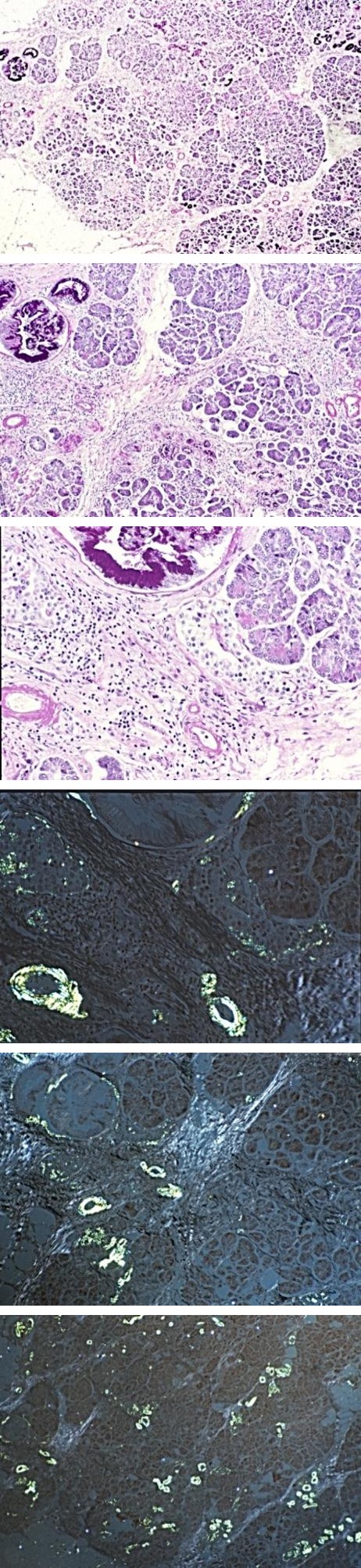
a b c Figure 6a-c: RA, AAa, Pancreas, early stage of pAAa amyloid A deposits in the wall of arterioles and small arteries with incipient amyloid A deposition in periductal basement membrane (in association with islet amyloid polypeptide deposits localized to the islets of Langerhans – see arrows of Figures 1c and 4c).
(4a) PAS, x20 (b) Same as (4a) PAS, x50 (c) Same as (4a), PAS, x125
a b c Figure 7a-c (same as Figure 4a-c): Congo red staining without alcoholic differentiation, covered with Canada balsam, viewed under polarized light. (5a) same as (4a), x20 (5b) same as (4b and 2a), x50 Apple green birefringence corresponds to amyloid A deposits, “white” birefringence is caused by the collagen fibers, covered with a polar hydrophobic mounting medium (Canada balsam) (5c) same as (4c and 5b), x125 Amyloid A deposits in arterioles and periductal basement membrane in association with islet amyloid polypeptide deposits localized to the islets of Langerhans (arrows)
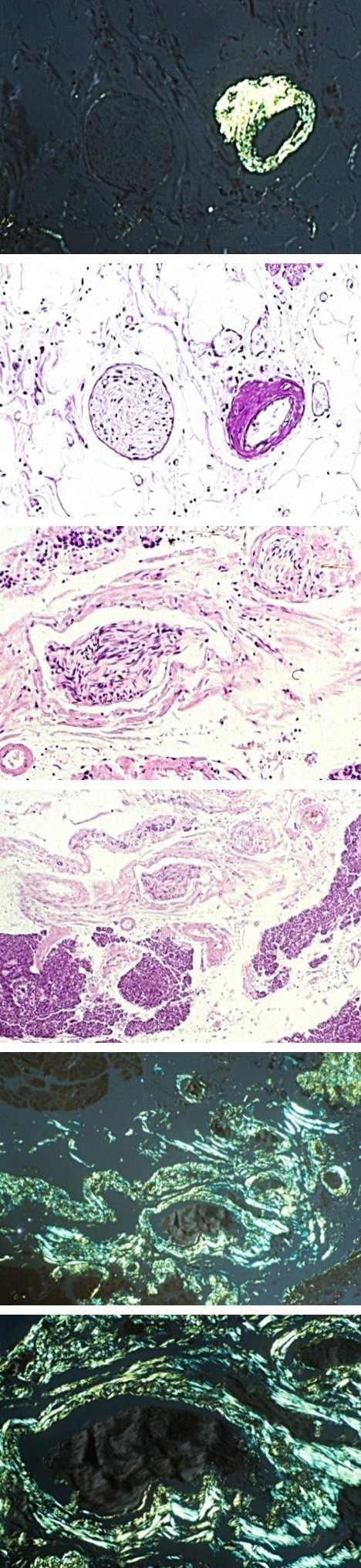
a b Figures 8a-b: RA, AAa, Pancreas, early stage of pAAa amyloid A deposits in the wall of arteriole with minimal perineural and reticular amyloid A deposits (a) PAS, x125 (b) Same as (a) Congo red staining according to Romhányi without alcoholic differentiation, covered with polar hydrophilic mounting medium (gum Arabic), x125.
a b Figures 9a-b: RA, AAa, Pancreas, late stage of pAAa massive amyloid A deposits in the wall of arterioles, small arteries, interstitial collagen fibers with marked neural involvement. (9a) H-E, x50 (9b) Same as (9a), H-E, x125
Figure 10a-b (same as Figure 9a-b): Congo red staining according to Romhányi without alcoholic differentiation, covered with gum Arabic, viewed under polarized light. (10a) same as (9a), x50 (10b) same as (9b and 10a), x125
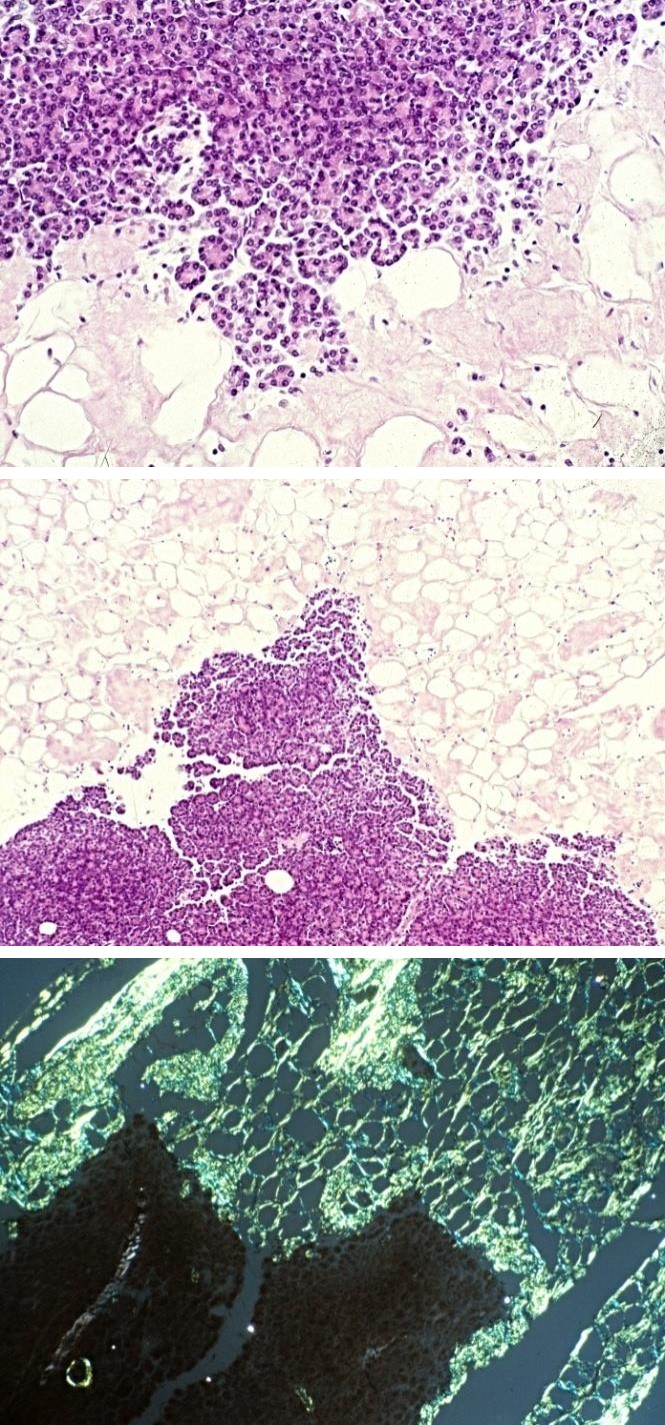
a b Figures 11a-b: RA, AAa, Pancreas, late stage of pAAa massive amyloid A deposits in the periglandular reticulin and interstitial collagen fibers. (11a) H-E, x50 (11b) Same as (11a) x125
a b Figures 12a-b (same as Figure 11a-b): Congo red staining according to Romhányi without alcoholic differentiation, covered with gum Arabic, viewed under polarized light. (12a) same as (11a), x50 (12b) same as (11b and 12a), x125
Discussion
only a few of these mention pancreatic involvement [21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41].
References Year of Publication Autopsy n= Prevalence of sAAa n – % Bayles 1943 [21] 23 ND* 3 of 23 – 13.0% ND Baggenstoss and Rosenberg 1943 [22] 30 2 – 6.6% 1 of 30 – 3.3% ND Rosenberg and Baggenstoss 1943 [23] 30 2 – 6.6% 1 of 30 – 3.3% ND Young and Schwedel 1944 [24] 33 5 – 15.2% 0 of 33 – 0% ND Unger et al. 1948 [25] 58 4 – 6.9% ND 1 of 4 – 25 % Teilum and Lindahl 1954 [26] 28 17 – 60.7% 7 of 28 – 25.0% ND Mortality of amyloidosis n – % Prevalence of pAAa n – %
| 1955 [27] | 45 | 11 – 24.4% | 9 of 45 – 20.0% | ND | |
| Sinclair and Cruickshank | 1956 [28] | 16 | 4 – 25.0% | 0 of 16 – 0% | 1 of 4 – 25 % |
| Missen and Tailor | 1956 [29] | 47 | 8 – 17.0% | 4 of 47 – 8.5% | ND |
| Lebowitz | 1963 [30] | 62 | 6 – 10.0% | ND | ND |
| Sokoloff | 1964 [31] | 19 | 0 – 0% | 0 of 19 – 0% | ND |
| Cohen | 1968 [32] | 42 | 11 – 26% | ND | ND |
| Gritsman | 1969 [33] | 15 | 6 – 40.0% | ND | ND |
| Ozdemir et al. | 1971 [34] | 47 | 1 – 2.1% | ND | 10 of 44 – 22.7% |
| Gardner | 1972 [35] | 142 | 17 – 11.97% | ND | ND |
| Püschel | 1973 [36] | 143 | 15 – 10.5% | ND | ND |
| Eulderink | 1976 [37] | 111 | ND | 6 of 111 – 5.4% | ND |
| Rainer et al. | 1978 [38] | 79 | ND | 4 of 79 – 5.0% | ND |
| Bély | 1990 [39] | 100 | 24 – 24.0% | ND | 18 of 21 – 85.71% |
| Bély | 1993 [40] | 161 | 34 – 21.1% | 17 of 161 – 11% | 26 of 29 – 89.65% |
| Suzuki et al. | 1994 [41] | 81 | 17 – 21.0% | 6 of 81 – 7.4% | ND |
Table 8: Prevalence and mortality of AA amyloidosis in patients with rheumatoid arthritis at autopsy*.
Table 5: Prevalence and mortality of AA amyloidosis in patients with rheumatoid arthritis at autopsy*. Remarks to Table 5 ND – No Data *– Amyloid deposits were identified with different staining methods: Toluidine blue, Crystal violet, Syrius red, Congo red staining according to Romhányi, Bennhold’s, Puchtler’s, Bély’s Congo red method.
According to our best knowledge a detailed analysis of the rate of systemic amyloid a deposition and its relationship to pAAa has not been available in the literature.
The precursors of amyloid protein fibrils are produced by the liver. The serum amyloid A proteins spread via the bloodstream are deposited throughout the body. The level of precursors in the blood depends on the production and/or elimination of amyloid proteins or, more succinctly, on the dynamics of these two processes.
Systemic amyloidosis is related to the cardiovascular system and becomes generalized via the bloodstream, while organ- or tissue-limited isolated amyloidosis is not directly related to the systemic circulation and remains localized [17, 42].
“All forms of amyloidosis related to the circulation of blood are systemic, and all forms of amyloidosis not connected to the circulation are isolated (localized)” [17]. This statement was confirmed by Sipe as an important conclusion of XIth International Symposium on A myloidosis, held in Woods Hole, Massachusetts, USA, November 5-9, 2006 [43].
The rate and amount of amyloid deposits existing in various organs may be linked to the differences in blood supply per unit volume and influenced by the possible incidental elimination of deposited amyloid [42, 44].
Amyloidosis is a progressive, cumulative process, involving in its early stage only a few structures in some organs, and increasingly more in the later stages of the disease [13, 18, 39, 40, 42, 45, 46].
The stages of amyloidosis in 14 RA patients with mild and 12 with severe pAAa demonstrated the same progressive, cumulative and basically linear pathological process shown in Figures 2 & 3, characterized by intensified deposition at the end stage.
Development of mild and severe amyloidosis are different aspect of the same process (based on the linear growth course of amyloid A deposition), determined only by production and circulating amounts of precursors. Quantitative differences in production of serum amyloid A may be related to a “benign” or “aggressive” clinical course of RA, which may be due to genetically and/or other factors.
Prevalence and severity of amyloid A deposits in different tissue structures of the pancreas signify different aspects of the same pathological process which usually run parallel to each other (Figure 4).
Amyloid A deposition starts in the most frequently involved structures of the most frequently involved organs [13, 40, 42, 44, 45].
In the pancreas the deposition of amyloid A starts in the wall of arterioles, small arteries and reticulum fibers.
Medium size veins and arteries, small veins, interstitial collagen fibers venules are involved later. Deposition within periductal basement membranes and involvement of the nerves indicates advanced stages of amyloidosis in the pancreas.
This chronology of amyloid A deposition allows an indirect assessment of the stage of amyloidosis. Based on the involved structures in biopsy specimens or surgical tissue samples the pathologist may estimate the involvement of other structures.
Involvement of arterioles and small arteries alone (without involvement of other structures) indicates an early stage of pancreatic amyloidosis, whereas amyloid A deposits periductal basement membranes and peripheral nerves suggest an advanced stage with massive involvement of numerous structures.
The nearly constant and permanent relationship between amyloid A deposits in different structures approximately indicates the amount of amyloid depositions in other structures of the pancreas, even in cases in which some structure is not present in a pancreatic biopsy specimen. Based on this assumption a biopsy specimen may have prognostic value in everyday pathological practice.
In the pancreas amyloid A deposition started later in comparison with average amyloid A deposition of other organs, increased gradually, and at the terminal stage showed a rapid progression in crossing the growth curve of amyloid A deposition of other organs (Figure 1). This may suggest unidentified protection mechanisms to ensure the function of vital organs such as heart, lung and kidneys (or others).
Conclusion
Systemic AAa is one of the main and most insidious complications of rheumatoid arthritis affecting the pancreas with high prevalence and severity.
Systemic AAa is related to the cardiovascular system, and pancreatic AAa is connected with it. In systemic AAa the amyloid A deposition in the pancreas starts after a latent stage. Systemic and pancreatic amyloid A deposition is a progressive and cumulative process, involving in its early stage only a few structures in the pancreas, and increasingly more in later stages of the disease. Amyloid a deposition starts in the most frequently involved structures of the pancreas with more massive deposits. The chronology of amyloid A deposition allows an indirect assessment of the stage of pancreatic amyloidosis, which may have a prognostic value in everyday surgical pathology as well.
From a prognostic point of view, amyloid a deposition in the pancreas did not prove to be a very serious, life- threatening complication of RA.
References
-
Tan SY, Pepys MB (1994) Amyloidosis. Histopathology 25: 403-414.
-
Mandema E, Ruinen L, Scholten JH, Cohen AS (1967) Amyloidosis. The Proceedings of the 1st International Symposium on Amyloidosis.
-
Wegelius O, Pasternack A (1974) Amyloidosis. The Proceedings of the 2nd International Symposium on Amyloidosis. The Fifth Sigrid Jusélius Foundation Symposium.
-
Glenner GG, Costa PP, Falcao de Freitas A (1979) Amyloid and amyloidosis. The Proceedings of the 3rd International Symposium on Amyloidosis, Povoa de Varzim.
-
Glenner GG, Osserman EF, Benditt EP, Calkins E, Cohen AS, et al. (1984) Amyloidosis. The Proceedings of the 4th International Symposium on Amyloidosis.
-
Isobe T, Araki S, Uchino F, Kito S, Tsubura E (1987) Amyloid and Amyloidosis. The Proceedings of the 5th International Symposium on Amyloidosis.
-
Natvig J, Forre O, Husby G, Husebekk A, Skogen B, et al. (1990) Amyloid and Amyloidosis 1990. The Proceedings of the 6th International Symposium on Amyloidosis.
-
Kisilevsky R, Benson MD, Frangione B, Gauldie J, Muckle TJ, et al. (1993) Oung ID Amyloid and Amyloidosis 1993, The Proceedings of the 7th International Symposium on Amyloidosis.
-
Kyle RA, Gertz MA (1998) Amyloid and Amyloidosis 1998. The Proceedings of the 8th International Symposium on Amyloidosis.
-
Bély M, Apáthy Á (2001) Amyloid and Amyloidosis the Proceedings of the IXth International Symposium on Amyloidosis.
-
Grateau G, Kyle RA, Skinner M (2004) Amyloid and Amyloidosis. The Proceedings of the 10th International Symposium on Amyloidosis.
-
Skinner M, Berk JL, Connors LH, Seldin DC (2007) XIth International Symposium on Amyloidosis. 1st (Edn), pp: 1-432.
-
Bély M, Apáthy Á (2012) Clinical pathology of rheumatoid arthritis: Cause of death, lethal complications and associated diseases in rheumatoid arthritis. 1st (Edn.), pp: 1-444.
-
Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, et al. (1988) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31(3): 315- 324.
-
Romhányi G (1971) Selective differentiation between amyloid and connective tissue structures based on the collagen specific topo-optical staining reaction with Congo red. Virchows Arch A Pathol Pathol Anat 354(3): 209-222.
-
Bély M, Makovitzky J (2006) Sensitivity and Specificity of Congo red Staining According to Romhányi - Comparison with Puchtler's or Bennhold's Methods. Acta Histochemica 108(3): 175- 180.
-
Bély M, Apáthy Á (2000) Histochemical and immunohistichemical differential diagnosis of amyloidosis - a brief illustrated essay and personal experience with Romhányi's method. Amyloid 7(3): 212-217.
-
Bély M (2006) Histochemical Differential Diagnosis and Polarization Optical Analysis of Amyloid and Amyloidosis. TheScientificWorldJournal 6: 154-168.
-
Szentágothai, Réthelyi J, Miklos (2006) Verőerek, Visszerek In: Funkcionális anatómia II. pp: 1-139.
-
Lentner C (1982) “Statistical methods” In Geigy scientific tables, 8th revised and enlarged. In: Lentner C, Compiled by: Diem K, Seldrup J (Eds.) 2: 227.
-
Bayles TB (1943) Rheumatoid arthritis and rheumatic heart disease in autopsied cases. 205: 42-48.
-
Baggenstoss AH, Rosenberg EF (1943) Visceral lesions associated with chronic infectious (rheumatoid) arthritis. Archives of Pathology 35: 503-
-
Rosenberg EF, Baggenstoss AH, Edward F, Hench PS (1944) The causes of death in thirty cases of rheumatoid arthritis. Annals of Internal Medicine 20: 903-919.
-
Young D, Schwedel JB (1944) The heart in rheumatoid arthritis. American Heart Journal 28: 1-23.
-
Unger PN, Zuckerbrod M, Beck GJ, Steele JM (1948) Amyloidosis in rheumatoid arthritis”. American Journal of Medical Sciences 216: 51-56.
-
Teilum G, Lindahl A (1954) Frequency and significance of amyloid changes in rheumatoid arthritis”. Acta Medica Scandinavica 149(6): 449-455.
-
Gedda PO (1955) On amyloidosis and other causes of death in rheumatoid arthritis. Acta Med Scand 60: 443-452.
-
Sinclair RJG, Cruickshank B (1956) A clinical and pathological study of sixteen cases of rheumatoid arthritis with extensive visceral involvement (Rheumatoid disease). Quarterly Journal of Medicine 25(3): 313-332.
-
Missen GAK, Taylor JD (1956) Amyloidosis in rheumatoid arthritis. Journal of Pathology and Bacteriology 71(1): 179-192.
-
Lebowitz WB (1963) The heart in rheumatoid arthritis (Rheumatoid disease). A clinical and pathological study of sixty-two cases. Ann Inter Med 58: 102-123.
-
Sokoloff L (1964) Cardiac involvement in rheumatoid arthritis and allied disorders: current concepts. Mod Concepts of Cardiovasc 33: 847-850.
-
Cohen AS (1968) Amyloidosis associated with rheumatoid arthritis. The Medical Clinics of Nrth America 52: 643-653.
-
Gritsman NN (1969) Morphological characteristics of affection of the heart in infectious nonspecific polyarthritis (rheumatoid arthritis. Archiv patologii 31: 49-53.
-
Ozdemir AI, Wright JR, Calkins E (1971) Influence of rheumatoid arthritis on amyloidosis of aging. Comparison of 47 rheumatoid patients with 47 controls matched for age and sex. N Engl J Med 285(10): 534-538.
-
Gardner DL (1972) Causes of death In The pathology of rheumatoid arthritis. Edward Arnold, London, pp:183-197.
-
Püschel W (1972) Sektionsstatistische Untersuchungen bei der Rheumatoid-Arthritis. Deutsche Gesundheitwesen 27: 754-756.
-
Eulderink F (1976) Doodsoorzak rheumatoide arthritis. Nederlands Tijdschrif voor Geneeskunde, 120: 357-363.
-
Rainer F, Klein G, Schmid P, Härringer M (1978) Untersuchungen über Art und Häufigkeit der Todesursachen bei chronischer Polyarthritis. Zeitschrift für Rheumatologie 37: 335-341.
-
Bély M (1990) Sekundäre Amyloidose bei chronischer Polyarthritis. Zentralblatt für allgemeine Pathologie und pathologische Anatomie 136(4): 337-357.
-
Bély M, Apathy A (1993) Krankheitsmodifizierende Faktoren bei chronischer Polyarthritis: Über Zusammenhänge zwischen generalisierter Vaskulitis, sekundärer Amyloidose, septischen Infektionen und Auftreten von miliaren epitheloidzelligen Granulomen. Zentralblatt fur Pathologie 139(1): 51-60.
-
Suzuki A, Ohosone Y, Obana M, Mita S, Matsuoka Y, et al. (1994) Cause of death in 81 autopsied patients with rheumatoid arthritis. J Rheumatol 21(1): 33-36.
-
Bely M, Apathy A, Pinter T, Ratko J (1992) Generalized secondary amyloidosis in rheumatoid arthritis. Acta Morphol Hung 40(1-4): 49-69.
-
Sipe JD (2008) Book review. The Proceedings of XIth International Symposium on Amyloidosis. Skinner M, Berk JL, Connors LH, Seldin DC (eds) Amyloid 15: 218-219.
-
Bély M, Apáthy Á (2006) Complications and associated diseases in Rheumatoid Arthritis A Retrospective Clinicopathologic Study of 234 Autopsy Patients [Hung]. Orvosi Hetilap 147: 1063-1076.
-
Bély M (2001) Identification of Amyloid Deposits by Histochemical Methods of Romhányi.” Amyloid: The Journal of Protein Folding Disorders, 8(S2): 177-182.
-
Bély M (2003) Differential diagnosis of amyloid and amyloidosis by histochemical methods of Romhányi and Wright. Acta Histochem 105(4): 361-365.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient