Humain Splenic Hydatidosis: A Review
Humain hydatidos is still endemic in several countries of the world and represents a major public health problem. Splenic involvement is rare, qualified as atypical/unusual or even "ectopic" and "aberrant" localizations by most authors. Its frequency is estimated at 0.9-8% and the splenic localization represents only 0.5 to 6% of the totality of abdominal Hydatidosis. It is exceptionally primary and isolated; classically integrating into a complex presentation of intraabdominal multi-visceral involvement or more diffuse Hydatidosis with pulmonary localization. Because of their rarity and the lack of knowledge on the part of medical practitioners, these unusual localizations of human Echinococcosis, but sometimes potentially fatal, often represent real diagnostic and therapeutic challenges, especially since clinical presentations are not stereotyped. In this review we present the different epidemiological, clinical, radiological, therapeutic, and evolutionary aspects of this localization in order to familiarize the health professionals with it.
Introduction
Echinococcosis is an anthropozoonosis that is still endemic in several countries of the world and represents a major public health problem [1, 2, 3, 4, 5]. Man represents an accidental intermediate host and all organs and/or tissues may be the seat of single or multiple hydatid cyst (HC) [6, 7]. The most frequent locations of human hydatid disease are the liver and lungs: 65-70% and 25% respectively [2, 4]. In rare cases, the embryos of Echinococcosis escape the hepatic and pulmonary filters to gain systemic circulation and cause other visceral localizations: the digestive tract, pancreas, spleen, urogenital system, retro peritoneum, peripheral nervous system, bones, endocrine glands, heart, soft tissues, etc. [8]. These localizations are described as atypical or unusual by most authors or even "ectopic" and "aberrant" by some [6, 7, 8, 9].
The overall frequency of these unusual localizations of HC, as well as the frequency of each localization apart, are difficult to define because of their rarity [9] and their frequent association with other typical localizations of the Parasitosis (concomitant liver and/or lung involvement) [6, 10, 11]. The average overall frequency retained by the majority of authors is around 10% and seems to be greater in the endemic regions of this Parasitosis [6, 7, 12, 13]. The primitive forms of these unusual localizations (isolated, without associated hepatic or pulmonary involvement) are, on the other hand, exceptional: only 0.9% in the series of Lianos GD et al collected over 33 years of experience [14].
Because of their rarity and the lack of knowledge on the part of medical practitioners, these unusual localizations of human Echinococcosis, but sometimes potentially fatal often represent a real diagnostic and therapeutic challenge, especially since clinical presentations are not stereotyped [6, 14, 15].
Splenic involvement remains rare during this Parasitosis. It is exceptionally primary and isolated; classically integrating into a complex presentation of intra-abdominal multi-visceral involvement or more diffuse Hydatidosis with pulmonary localization [3, 5, 16, 17].
In this review we present the different epidemiological, clinical, radiological, therapeutic, and evolutionary aspects of this localization in order to familiarize the health professionals with it, to be able to make the diagnosis quickly and to undertake an adapted treatment in time, to improve the prognosis of this location which can be fatal.
Epidemiology
Involvement of the spleen is rare even in countries endemic for HC and can occur at any age and in both sexes without preference [16, 17, 18]. Its frequency is estimated at 0.9-8% and the splenic localization represents only 0.5 to 6% of the totality of abdominal Hydatidosis [16]: in fact, in the large series of Vahedi MA, et al. [5] of 318 cases of HC collected in the department of Eastern Azerbaijan, an endemic region for HC in Iran, splenic localization was found in only one case (2.2%). Similarly Malik AA, et al. in their series of 382 cases of abdominal HC had objectified splenic localization in only 8 patients (2%) [5, 18].
In the Tunisian series of Bellil S, et al. of extra- pulmonary operated HC, the involvement of the spleen seems to be a little more frequent compared to the world literature, since found in 30 out of 265 patients (11.3%); this seems to be rather due to a recruitment bias. The spleen is generally the third site of HC infection after the liver and the lung [3, 19].
Pathophysiology/Mechanisms
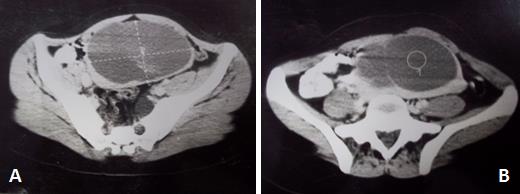
The physical examination of a patient with splenic HC shows in most cases splenomegaly or a mass of the left hypochondrium (Figure1). It sometimes objectifies associated hepatomegaly as it can remain strictly normal [16, 18, 19].
The rarity of splenic involvement during this Parasitosis is consistent with the natural life cycle of the Echinococcosis granulose where only 10 to 20% of hexacanthes embryos can escape the double hepatic and pulmonary circulation, said first and second filters, to spread in the different tissues and organs [16].
The hypothesis of a retrograde infection of the spleen from hepatic Hydatidosis in case of portal hypertension, via the portal vein and then the splenic vein, is also mentioned to explain the splenic localization of this Parasitosis, as well as involvement by gastric or colonic trans-parietal contiguity or by lymphatic dissemination [19].
Splenic HC is classically unique and solitary; more rarely the involvement of the spleen can be multiple or else associated with other hydatid localizations: in particular hepatic, peritoneal and more rarely cardiac, renal, retro-peritoneal, of the gastric wall or the mesocolon [16, 17, 19].
Clinical Presentations/Signs
Due to a very slow growth of the cyst, splenic Echinococcosis remains asymptomatic for a long time [3, 5, 16, 17] and is often fortuitously discovered during screening campaigns in endemic areas, during the exploration of non-specific symptoms, in the context of the lesional assessment of another hydatid localization, or on the occasion of a recurrence especially after surgery of HC of the liver [16, 19].
In the rare symptomatic cases, the clinic results either from a mass effect or from a crack or rupture of the cyst in the abdominal cavity [17].
It may be vague and nonspecific abdominal pain or feeling of heaviness in the left hypochondrium but may in some cases simulate a true acute abdomen [16, 17, 19].
In addition, some anecdotal clinical presentations of splenic HC have been observed: spontaneous fistulization to the skin, arterial hypertension by compression of the ipsilateral renal artery, segmental portal hypertension, hemoperitoneum or recurrent upper gastrointestinal bleeding by isolated gastric varices from the fundus caused by compression of the splenic vein by the HC [18, 20, 21].

Paraclinical Explorations
Confirmation of the diagnosis is based on the pair imaging-serology (immunofluorescence or ELISA) [19]. Abdominal ultrasound, often completed by CT scan, is very helpful for the diagnosis of spleen HC [16, 22]: calcifications of the cyst wall, the presence of daughter vesicles, the appearance of detached membrane (water- lily-sign), and intracystic septa in multilocular forms (rosette-like/honeycomb cyst) are very specific to this condition.
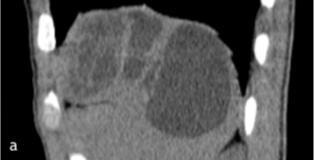
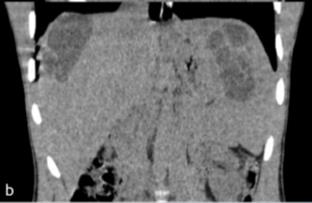
CT is particularly interesting and useful for the complete lesional assessment of splenic Hydatidosis (isolated or associated with other intra-abdominal visceral sites, in particular hepatic (Figures 2 & 3) [3, 5, 16, 17].
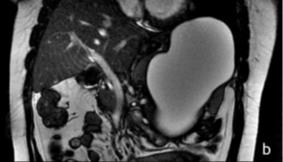
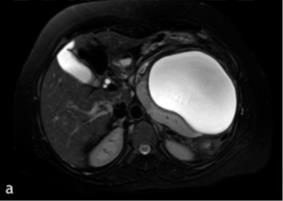
MRI is similar to CT for characterization of splenic HC and lesion balance of other locations; splenic HC is characterized on the MRI by the hypo signal of its own membrane on T2 weighted sequences [16, 17, 22] (Figure 4).
The ultrasound classification of Gharbi is the most used for the characterization of HC: type 1 (unilocular cyst), type 2 (cyst with detached membrane), type 3 (multivesicular cyst), type 4 (pseudotumoral cyst) and type 5 (calcified cyst) [16, 22].
Evolution/Complications
In the absence of treatment, the evolution of splenic HC can be towards the rupture or the micro-rupture causing the intra-peritoneal dissemination of the Parasitosis [16] or provoking a reaction of severe systemic anaphylaxis threatening sometimes the vital prognosis.
The cyst can also become infected, fistulate in adjacent viscera stomach, colon, small intestine or trans- diaphragmatic, compress the urinary tract and cause homolateral hydronephrosis, or invade the retro peritoneum and cause multiple adhesions and pseudotumoral inflammatory lesions [16, 19].
Treatment
Treatment of splenic HC is still non-consensual. Total surgical splenectomy represents the optimal radical treatment for several authors. It avoids local recurrence but can sometimes be difficult to achieve; especially if cysto-visceral adhesions [16, 17, 19].
It is also burdened with significant morbidity and mortality: mortality of 3.7 to 22.5% and morbidity of 21 to 25% (hemorrhagic shock, subphrenic abscess and infectious complications). Laparoscopic splenectomy has also been found to be effective in the treatment of these cysts [16, 23].
Splenic conservative surgery has also been proposed with different modalities: partial splenectomy, resection of the salient dome and surgical or laparoscopic cystectomy. Resection of the salient dome is more prone to postoperative complications: haemorrhage, residual cavity abscess and local recurrence [19].
The operative indication will depend on the size of the cyst, its location, the number of cysts and the association with other visceral involvement; as well as the type of cyst and the existence or not of a possible complication [19].
Thus, and in light of the results of a personal operating series, Ousadden A, et al. propose a therapeutic strategy of splenic HC in three modes [19]:
- Splenic HC type A: unipolar superior or inferior HC, sparing more than a quarter of the spleen: partial splenectomy is preferred,
- Splenic HC type B: not unipolar HC, sparing more than a quarter of the spleen: resection of the salient dome is preferred,
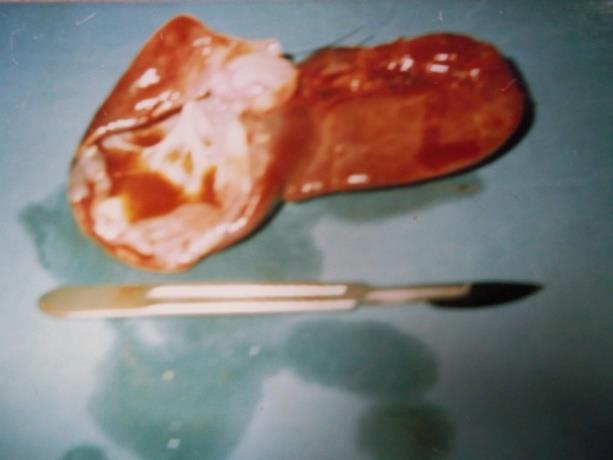
- Splenic HC type C: HC destroying more than three quarters of the spleen: total splenectomy is preferred (Figures 5 & 6).

Additional anti-parasitic treatment with oral Albendazole is recommended in all cases. Its purpose is to avoid post-operative recurrence [16, 17].
Conclusion
Far from being rare in endemic countries for this Parasitosis, splenic Hydatidosis deserves to be well known by all health professionals. It must be evoked in front of any splenic cystic mass diagnosed in a person living in or coming from an endemic zone. Diagnosis is currently facilitated by imaging, especially ultrasonography and computed tomography. The treatment of choice remains the radical surgery which must be carried out in time to avoid the possible complications, sometimes fatal. Conflicts of Interest: None
References
-
McManus DP, Thompson RCA (2003) Molecular epidemiology of cystic Echinococcosis. Parasitology 127: S37-S51.
-
Grosso G, Gruttadauria S, Biondi A, Marventano S, Mistretta A (2012) Worldwide epidemiology of liver Hydatidosis including the Mediterranean area. World J Gastroenterol 18(13):1425-1437.
-
Bellil S, Limaiem F, Bellil K, Chelly I, Mekni A, et al. (2009) Descriptive epidemiology of extrapulmonary hydatid cysts: a report of 265 Tunisian cases. Tunis Med 87(2): 123-126.
-
Moro P, Schantz PM (2009) Echinococcosis: a review. Int J Infect Dis 13(2): 125-133.
-
Vahedi MA, Vahedi ML (2012) Demographics of patients with surgical and nonsurgical cystic echinococcosis in East Azerbaijan from 2001 to 2012. Pak J Biol Sci 15(4): 186-91.
-
Gun E, Etit D, Buyuktalanci DO, Cakalagaoglu F (2017) Unusual locations of hydatid disease: A 10-year experience from a tertiary reference center in Western Turkey. Ann Diagn Pathol 29: 37-40.
-
Keser SH, Selek A, Ece D, Barişik CC, Şensu S, et al. (2017) Review of Hydatid Cyst with Focus on Cases with Unusual Locations. Turk Patoloji Derg 33(1): 30- 36.
-
Çakır M, Balasar M, Küçükkartallar T, Tekin A, Kartal A, et al. (2016) Management of Extra-Hepatopulmonary Hydatid Cysts (157 cases). Turkiye Parazitol Derg 40(2): 72-76.
-
Saadi A, Bouzouita A, Cherif M, Rebai MH, Kerkeni W, et al. (2015) Retrovesical hydatic cyst: About 4 cases. Can Urol Assoc J 9(5-6): E374-378.
-
Akcam AT, Ulku A, Koltas IS, Izol V, Bicer OS, et al. (2014) Clinical characterization of unusual cystic echinococcosis in southern part of Turkey. Ann Saudi Med 34(6): 508-516.
-
Lucandri G, D'Elia G, Chiavellati L, Sterpetti A, Meloni E, et al. (1994) Unusual location of hydatid cysts: clinical and therapeutic aspects. G Chir 15(11-12): 529-537.
-
Kireşi DA, Karabacakoğlu A, Odev K, Karaköse S (2003) Uncommon locations of hydatid cysts. Acta Radiol 44(6): 622-636.
-
Hakverdi S, Sayar H, Yaldiz M, Erdoğan S, Akansu B, et al. (2009) Unusual localization of echinococcosis in Cukurova (134 cases). Turkiye Parazitol Derg 33(1): 77-81.
-
Lianos GD, Lazaros A, Vlachos K, Georgiou GK, Harissis HV, et al. (2015) Unusual locations of hydatid disease: a 33 years’ experience analysis on 233 patients. Updates Surg 67(3): 279-282.
-
Salamone G, Licari L, Randisi B, Falco N, Tutino R, et al. (2016) Uncommon localizations of hydatid cyst. Review of the literature. G Chir 37(4): 180-185.
-
Vezakis A, Dellaportas D, Polymeneas G, Tasoulis MK, Chondrogiannis C, et al. (2012) Two cases of primary splenic hydatid cyst in Greece. Korean J Parasitol 50(2): 147-150.
-
Lianos G, Baltogiannis G, Lazaros A, Vlachos K (2012) Hydatid disease simulating acute abdomen: a case report and brief review of the literature. Case Rep Gastrointest Med 2012: 3.
-
Malik AA, Ul Bari S, Younis M, Wani KA, Rather AA (2011) Primary splenic hydatidosis. Indian J Gastroenterol 30(4): 175-177.
-
Ousadden A, Raiss M, Hrora A, Aitlaalim S, Alaoui M, et al. (2010) Hydatid cysts of the spleen: conservative or radical surgery? Pan Afr Med J 5: 21-25.
-
Eckert J, Deplazes P (2004) Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev 17(1): 107-135.
-
Kantarçeken B, Çetınkaya A, Bülbüloğlu E, Demırpolat G (2010) Splenic hydatic cyst as a cause of sinistral portal hypertension and isolated gastric variceal bleeding. Turk J Gastroenterol 21(3): 317-20.
-
Papavramidis TS, Laskou S, Michalopoulos N, Pliakos I, Kesisoglou I, et al. (2012) Typical image of splenic hydatidosis. Trop Doct 42(2): 118-119.
-
Ormeci N, Soykan I, Palabiyikolu M, Idilman R, Erdem H, et al. (2002) A New Therapeutic Approach for Treatment of Hydatid Cysts of the Spleen. Dig Dis Sci 47: 2037-2044.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient