Gastric Antral Vascular Ectasia (GAVE) Disorder
Gastric antral vascular ectasia (GAVE) syndrome is an uncommon cause of chronic gastrointestinal bleeding as well as iron deficiency anaemia. We present two cases of GAVE, one with pernicious anaemia associated and the other is portal hypertension related. In both cases, progressive mucosal changes, which results in formation of GAVE, were documented. The changes were progression of multiple antral erythematous spots into linear configuration and finally to watermelon stomach.
Zubin Pradeep Sharma*, Divya Sharma and Ravindra Sharma
Centre, SriGanganagar, Rajasthan, India
Endoscopy, Aditya Hospital and Gastroenterology Centre, Sri Ganganagar, Rajasthan, India, Email: adityagastrocenter@gmail.com to watermelon stomach.
Keywords: Gastric Antral; Anaemia; Venogram
Introduction
In 1953, Rider et al described gastric antral vascular abnormalities, which were known by the name of watermelon stomach by Jabbari, et al. in 1984. Clinically GAVE resents as chronic gastrointestinal bleeding and endoscopically its appearance resembling like a watermelon. A little is known about its pathogenesis [1]. Although surgical antrectomy is curative, which may not be achievable in diffuse disease or in presence of portal hypertensive collaterals, there is a role of medical as well as endoscopic management.
Till date to our knowledge, no description in the world literature has described progressive mucosal appearances that leads to the development of GAVE. We have documented endoscopically progressive changes of appearances in two cases, in which typical endoscopic picture of GAVE developed afterwards.
Case Reports
Case 1
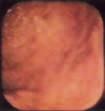
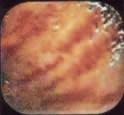
A 69 years male presented with pallor and weakness of six months duration. He was investigated as a case of anaemia and diagnosed to have pernicious anaemia on basis of megaloblastic type of anemia, positive anti- parietal cell antibodies, positive intrinsic factor antibodies, low vitamin B12 levels, achlorhydria and atrophic gastritis on upper GI scopy. He was put on longterm parenteral vitamin B12 supplementation and was doing well (hemoglobin ~ 11.5 gm/dl). After few follow ups in, 2017 his Hb started dropping (to 10 gm/dl and was found to have anaemia with positive occult blood test in stools. Colonoscopy and small bowel barium series were normal. His upper GI scopy at that time (2016) revealed atrophic gastritis with presence of multiple small red spots in whole of the antrum (Table 1, Figure 1). Follow up upper GI scopy in 2017 revealed linearly arranged multiple red sports at few sites in antrum and atrophic gastritis (Table 1, Figure 2). Upper GI scopy in 2018 revealed classical watermelon appearance in antrum in addition to gastric atrophy (Table 1, Figure 3) Hb further dropped to 7.2 mg/dl and patient developed microcytic hypochromic anemia suggesting iron deficiency anemia. Patient was put on iron supplementation in addition to vitamin B12 therapy since 2018 and is doing well and his hematologic indices improved nearing normalization.
| MCV | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Year | Hb Gm/Dl | Fe Mg | TIBC | Indication for Upper GI Scopy | Upper GI Scopy Findings | |||||||||||||||||
| fl | |||||||||||||||||||||||
| 1 | 2014 | 8 | 110 | 9 8 | 297 | Pernicious anaemia | Atrophic gastritis | ||||||||||||||||
| 2016 | 11.5 | 9 2 | 53 | 310 | Iron deficiency anemia, stool OB+ | Multiple red spots in antrum | |||||||||||||||||
| 2017 | 10 | 7 9 | 40 | 454 | Follow up, stool OB+ | Few linear red stripes | |||||||||||||||||
| 2018 | 7.2 | 6 3 | 2 3 | 488 | Iron deficiency anaemia, stool OB+ | Watermelon | |||||||||||||||||
| 2 | 2014 | 4.7 | 61 | 2 0 | 454 | Iron deficiency, stool OB+ | Multiple red spots in antrum | ||||||||||||||||
| 2015 | 6 | 67 | 5 3 | 387 | Persistent iron deficiency anaemia | Watermelon | |||||||||||||||||
| 2016 | 10 | 70 | 7 8 | 280 | Follow up endoscopy | Watermelon |
Table 1: Hematological parameters and upper GI endoscopy findings of both the patients.
Case 2
A 71 years female was investigated for iron deficiency anemia of four years duration, for which she required continuous iron supplementation and multiple blood transfusions. She had two hospital admissions for complaints of easy fatigability, weakness and dyspnea on exertion (in 2014 and 2015). Clinically she had pallor. She had iron deficiency anemia with normal liver and renal function tests. Cardiac work up, including ECG, chest X-ray and 2 D- echocardiography was normal. Her stool occult blood test was positive. Colonoscopy and small bowel barium series were normal. Upper GI scopy in 2014 revealed multiple tiny red spots in whole of the antrum (Table 1). Imaging studies revealed (USG and CT scan- abdomen) presence of spontaneous lienorenal shunt, dilated tortuous collaterals at splenic hilum, mild splenomegaly and normal liver. Again in 2015, her upper GI scopy revealed classical watermelon appearance in antrum without evidence of varices or portal hypertensive gastropathy (Table 1). Her hepatic and portal tolerance test was normal. She refused to undergo liver biopsy. She was put on Tranexamic acid 500 mg tablets three times a day and is maintaining hemoglobin ~ 10 gm/dl (2016) and is symptom-free for last one year (Table 1). venogram showed presence of portal hypertension, large lienorenal shunt and small portoazygous shunts. All the tests for viral and autoimmune etiology, lipid profile and glucose.
Discussion
Gastric antral vascular ectasia syndrome is an unusual entity. It is present in 3% of cirrhotics, whereas 30-40% of GAVE patients comprise portal hypertension. Classic noncirrhotic patient is middle-aged female with underlying autoimmune disease or atrophic gastritis [1].
Its relation with scleroderma, pernicious anaemia, chronic renal failure, aortic stenosis, gastric carcinoma, bone marrow transplantation and antral mucosal prolapse is reported in the world literature [2, 3, 4].
It is characterized by chronic gastrointestinal blood loss, iron deficiency anaemia and transfusion dependence. Very rarely, it may present as acute gastrointestinal bleed. Endoscopic appearances are classically described as watermelon stomach with prominent longitudinal red stripes on antral mucosa radiating out from pylorus. Each stripe represents several flat red mucosal lesions of 1 to 5 mm size, lying in close proximity [1].
Differentiation from portal hypertensive gastropathy is by Chapman RW, et al. [1] antrum as major site L Spahr, et al. [2] lack of snake-skin-like appearance Moss SF, et al. [3] dilated capillaries with thrombi, fibrohylinosis and spindle cell proliferation on biopsy Gostout CJ, et al. [4] no relation to grade of portal hypertension and Gracia N, et al. [5] no response to beta-blockers and portosystemic shunts. Pathogenesis of GAVE is unclear - mucosal atrophy, high gastrin levels, hypertrophy of neuroendocrine cells in the antral region (5-HT and VIP) mechanical stress and portal hypertension are drawn in L Spahr, et al. [2].
Treatment of GAVE is complicated. Medical treatments like steroids, estrogen-progesterone combination and tranexamic acid are tried with incompatible results. Endoscopic treatment with laser photocoagulation (Nd- Yag or APC) or heat probe diathermy is progressively more reported to be successful and can delay surgical management, which is definite the curative treatment [3, 5, 6]. None of the reports reviewed gradual development of GAVE. In our report, we describe natural course of formation of watermelon stomach. It starts as localized erythematous spots and then, develops into linear lesions and finally, into characteristic watermelon stomach.
References
-
Chapman RW, Peter WA (1999) Effect of liver disease on gastrointestinal tract. In: Oxford Textbook of Clinical hepatology, second ed. UK: Oxford University Press, pp: 1817-1822.
-
L Spahr, J Villeneuve, M Dufresne, D Tasse, B Bui, et al. (1999) GAVE in cirrhotic patients - absence of relation with portal hypertension. Gut 44(5): 739- 42.
-
Moss SF, Gosh P, Thomas DM, Jackson JE, Calam J (1992) Gastric antral vascular ectasia in maintenance treatment with estrogen - progesterone. Gut 33(5): 715-717.
-
Gostout CJ, Viggiano TR, Ahlquist DA, Wang KK, Larson MV, et al. (1992) Clinical and endoscopic spectrum of the watermelon stomach. J Clin Gastroenterol 15(3): 256-263.
-
Gracia N, Sanyal AJ (1992) Portal hypertensive gastropathy and endoscopic spectrum of the watermelon stomach. J Clin Gastroenterol 15: 256-63.
-
McCormick PA, Ooi H, Crosbie O (1998) Tranexamic acid for severe bleeding gastric antral vascular ectasia in cirrhosis. Gut 42(5): 750-752.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient