Increased Risk of Hepatocellular Carcinoma in Patient with Inflammatory Bowel Disease and Hemochromatosis: A Case Report
Inflammatory bowel diseases could be associated with extra-intestinal manifestation; in this report we describe the case of a patient with ulcerative colitis who was diagnosed with genetic hemochromatosis (homozygosity for C282Y in the HFE gene) after a colitis relapse with high levels of serum ferritin (2000 ng/mL). After the genetic diagnosis patient underwent to an upper abdomen US with CEUS, with evidence of a 2 cm nodule in VIIs, suggestive for hepatocellular carcinoma, then confirmed with MR and CT scan. Patient underwent surgical resection of the lesion with histological confirmation of the malignant neoplasia. A correlation between the two diseases is not clear, but inflammatory bowel diseases and genetic hemochromatosis have some similarity: both diseases are related with functional reduction of hepcidin and in both diseases the mutations are located in chromosome 6p. Furthermore, regarding therapies, there is no evidence that iron chelation therapies could aggravate symptoms of ulcerative colitis, instead a chronic therapy with mesalazine could induce a chronic liver damage, worsening the hemochromatosis related liver damage.
Introduction
Inflammatory Bowel Diseases (IBD) are often associated with extra-intestinal manifestations (EIMs), Increased Risk of Hepatocellular Carcinoma in Patient with Inflammatory Bowel Disease and Hemochromatosis: A Case Report which are mainly rheumatological (axial or peripheral spondyloarthritis, dactylitis, etc.) and/or dermatological (sweet syndrome, erythema nodosum, pyoderma gangrenosum, etc.), but can also involve the hepatobiliary tract. The most specific hepatobiliary disorder in IBD patients is primary sclerosing cholangitis, PSC (7,4% of IBD patients has PSC and 70% of PSC patients has IBD) [1, 2, 3, 4, 5].
Gastroenterol Hepatol Int J
Hereditary hemocromatosis is reported to induce liver damage due to iron accumulation that can lead to cancer [6]. In this report we describe a case of an IBD patient who was diagnosed with genetic hemochromatosis type 1 which was complicated by hepatocellular carcinoma (HCC).
Case Report
A 63-years-old Italian man, who was diagnosed with ulcerative colitis (UC) in July 2014, was referred to our Centre in June 2015 for a disease relapse (bloody diarrhea with abdominal pain and weight loss - full Mayo score 9) despite oral and topical mesalazine. Laboratory tests showed increased pro-inflammatory values, including serum ferritin (2000 ng/mL). At first, we attributed the high levels of serum ferritin to the UC relapse, but the persistence of elevated values despite resolution of
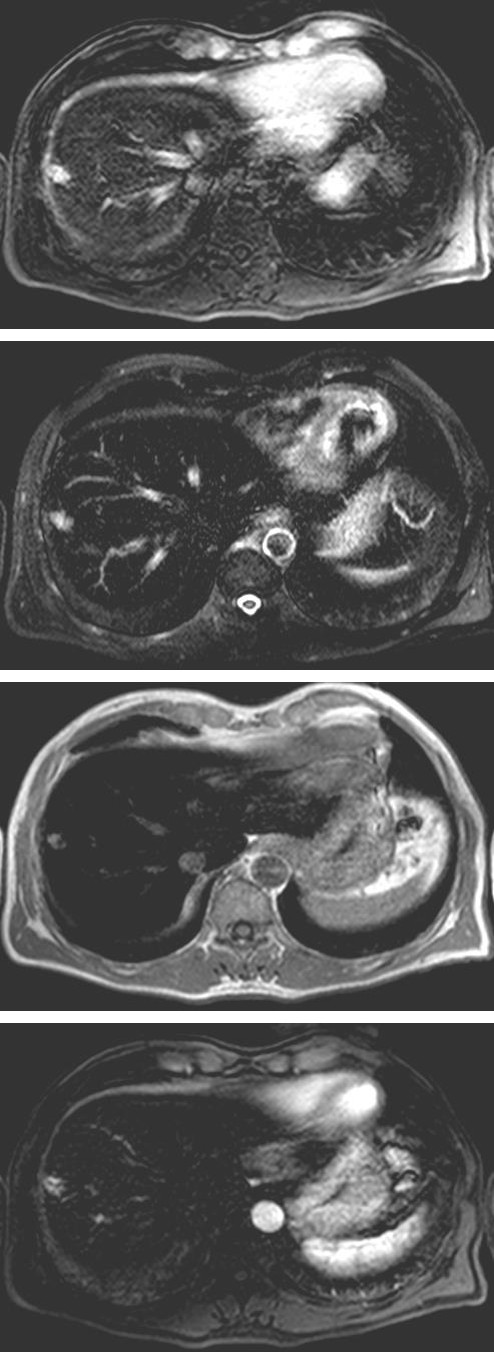
intestinal symptoms and a positive family history for cryptogenic liver disease, led us to further analyze the hepatic asset. After excluding common causes of hepatic damage related to high serum ferritin (NAFLD, ASH, metabolic syndrome, etc.), the patient underwent a genetic test, which showed homozygosity for C282Y in the HFE gene, so we were able to diagnose HFE hemochromatosis. The patient began iron chelation therapy with deferasirox 750 mg/die. An upper abdomen US with CEUS was performed and showed a 2 cm lesion in VIIs, suggestive for HCC which was confirmed with a CT scan and a liver MR (Figure 1). In December 2015 the patient underwent resection of the nodule with complete eradication. The patient regularly attends oncological and gastroenterological follow-up visits for hemochromatosis and ulcerative colitis at our Centre and continues specific therapies (oral and topical mesalazine and deferasirox).
Discussion
The Role of Hepcidin in Hereditary Hemocromatosis and IBD
In hereditary hemocromatosis, HFE gene mutations reduce or block hepcidin-induced internalization of Tarocchi M, et al. Increased Risk of Hepatocellular Carcinoma in Patient with Inflammatory Bowel Disease and Hemochromatosis: A Case Report. Gastroenterol Hepatol Int J 2019, 4(2): 000161.
ferroportin causing hyperabsorption of dietary iron and increased release of iron from macrophages to the bloodstream [7]. The exact connection between hepcidin and IBD is still unclear. Anaemia in IBD is partly due an increased expression of proinflammatory cytokines (TNF alfa, IFN alfa, IL1, IL6) and a reduced expression of hepcidin, which results in reduced intestinal iron Copyright© Tarocchi M, et al.
absorption and increased iron release from macrophages [8, 9, 10, 11, 12, 13]. Some authors have demonstrated that hepcidin levels are lower in IBD patients. This could be explained by the hyperactivation of pro-inflammatory pathways, which is seen in IBD patients, that leads to a reduction in circulating iron and iron reserves, which consequently reduces or blocks hepcidin syntheses. Body iron reserves are, in fact, amongst the main regulators of the production of hepcidin. Mecklenburg et al. [14] showed that hepcidin levels correlated with serum ferritin levels, with a serum ferritin cut-off of 30 microg/L and were independent of disease severity [14].
Is There a Genetic Correlation?
It is now commonly accepted that inflammatory bowel diseases have a multifactorial pathogenesis. To have a positive family history is amongst the greatest risk factors for IBD and many IBD susceptibility genes have been discovered. The strongest correlation has been found between single nucleotide polymorphisms (SNPs) within the HLA region, which is localized on the short arm of chromosome 6 (6p21) [15, 16]. Hereditary hemochromatosis is usually inherited in an autosomal- recessive pattern and is associated with mutations of the HFE gene, which is also localized on the short arm of chromosome 6 (6p22.2). The physical closeness of the loci involved in the two diseases (6p21 e 6p22.2) are been suggested to have a role in the coexistance of the two diseases in one single patient, as described in this case report and in other cases in literature [17, 18, 19].
Is There a Correlation Between First Line Therapies for IBD (Mesalazine and Steroids) and an Increased Risk of HCC in HFE Hemochromatosis?
An higher risk of HCC in HFE hemochromatosis patients is known. In our patient the IBD therapies could have worsened the liver damage, indeed an higher risk of chronic liver damage has been demonstrated in IBD patients ongoing chronic therapy with mesalazine [20, 21].
Could Deferasirox Worsen The Symptoms of Ulcerative Colitis?
There is no evidence of a correlation between iron chelation therapy for HFE hemochromatosis and the aggravation of symptoms of ulcerative colitis.
Tarocchi M, et al. Increased Risk of Hepatocellular Carcinoma in Patient with Inflammatory Bowel Disease and Hemochromatosis: A Case Report. Gastroenterol Hepatol Int J 2019, 4(2): 000161.
Conclusions
IBD patients in active treatment with mutations of HFE gene have an higher risk of manifestation of hemochromatosis and its complications: for this reason a follow-up of liver functions is strongly suggested.
Conflict of Interest
None
Funding
None
References
-
Harbord M, Annese V, Vavricka SR, Allez M, Barreiro- de Acos, et al. (2016) The first european evidence- based consensus on extra-intestinal manifestations in inflammatory bowel disease. J Crohns Colitis 10(3): 239-254
-
Broome U, Bergquist A (2006) Primary sclerosing cholangitis, inflammatory bowel disease and colon cancer. Semin Liver Dis 26(1): 31-41.
-
Rojas-Feria M, Castro M, Suárez E, Ampuero J, Romero-Gómez M (2013) Hepatobiliary manifestations in inflammatory bowel disease: the gut, the drugs and the liver. World J Gastroenterol 19(42): 7327-7340.
-
Silva J, Brito BS, Isaac Neri de NS, Nóbrega VG, da Silva MC (2019) Frequency of Hepatobiliary Manifestations and Concomitant Liver Disease in Inflammatory Bowel Disease Patients. Biomed Res In 2019: 7.
-
Fousekis FS, Theopistos VI, Katsanos KH, Tsianos EV, Christodoulou DK (2018) Hepatobiliary Manifestations and Complications in Inflammatory Bowel Disease: A Review. Gastroenterology Res 11(2): 83-94.
-
Kew MC (2014) Hepatic iron overload and hepatocellular carcinoma. Liver Cancer 3(1): 31-40.
-
Pantopoulos K (2008) Function of the hemochromatosis protein HFE: lessons from animal models. World J Gastroenterol 14(45): 6893-6901. Copyright© Tarocchi M, et al.
-
Dignas AU, Gasche C, Bettenworth D, Birgegard G, Danese S, et al. (2015) European consensus on the diagnosis and management of iron deficiency anaemia in inflammatory bowel disease. J Crohns Colitis 9(3): 211-222.
-
Semrin G, Fishman DS, Bousvaros A, Zholudev A, Saunders AC, et al. (2006) Impaired intestinal iron absorption in Crohn’s disease correlates with disease activity and markers of inflammation. Inflamm Bowel Dis 12(12): 1101-1106.
-
Dudkowiak R, Neubauer K, Poniewierka E (2013) Hepcidin and its role in inflammatory bowel disease. Adv Clin Exp Med 22(4): 585-591.
-
Nemeth E, Rivera S, Gabayan V, Keller C, Taudorf S, et al. (2004) IL6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J Clin Invest 113(9): 1271-1276.
-
Weiss G (2005) Anemia of chronic disease. N Engl J Med 352(10): 1011-1023.
-
Theurl I, Aigner E, Theurl M, Nairz M, Seifert M, et al. (2009) Regulation of iron homeostasis in anemia of chronic disease and iron deficiency anemia: diagnostic and therapeutic implications. Blood 113(21): 5277-5286.
-
Mecklenburg I, Reznik D, Fasler-Kan E, Drewe J, Beglinger C, et al. (2014) Serum hepcidin concentrations correlate with ferritin in patients with inflammatory bowel disease. J Crohns Colitis 8(11): 1392-1397. Tarocchi M, et al. Increased Risk of Hepatocellular Carcinoma in Patient with Inflammatory Bowel Disease and Hemochromatosis: A Case Report. Gastroenterol Hepatol Int J 2019, 4(2): 000161.
-
Ellinghaus D, Bethune J, Petersen BS, Franke A (2015) The genetics of Crohn’s disease and ulcerative colitis – status quo and beyond. Scandinavian J Gastroenterol 50(1): 13-23.
-
McGovern DP, Kugathasan S, Cho JH (2015) Genetics of inflammatory bowel disease. Gastroenterology 149(5): 1163-1176.
-
Beutler E (2003) The HFE Cys282Tyr mutation as a necessary but not sufficient cause of clinical hereditary hemocromatosis. Blood 101(9): 3347- 3350.
-
Ponsioen CY, Stokkers PC, vd Horst AR, Tytgat GN, van Deventer SJ (2001) A patient with hereditary hemochromatosis, ulcerative colitis and primary sclerosing cholangitis: genetic aspects. Eur J Intern Med 12(5): 518-521.
-
Sokorska k, Liberek A, Romanowski T, Szlagatys- Sidorkiewicz A, Landowski P, et al. (2011) Diagnosis and treatment difficulties in 18-year-old male patient with hereditary hemochromatosis, chronic hepatitis B, Gilbert syndrome and ulcerative colitis. Acta Biochim Pol 58(2): 251-254.
-
Khokhar OS, Lewis JH (2010) Hepatotoxicity of agents used in the management of inflammatory bowel disease. Dig Dis 28(3): 508-518.
-
Ransford RA, Langman MJ (2002) Sulphasalazine and mesalazine: serious adverse reaction re-evaluated on the basis of suspected adverse reaction reports to the Committee on Safety of Medicines. Gut 51(4): 536- 539. Copyright© Tarocchi M, et al.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient