Racial Differences for Gender, Age and BMI and the Presence of Adenomas in Screening and Surveillance Colonoscopies
Introduction: This study evaluated the correlation of the presence of polyps and adenomas with respect to age, gender, and BMI in the context of AA as compared to Non-AA patients in the setting of colonoscopy screening and surveillance. Methods: A retrospective medical chart review was conducted on 1095 screening or surveillance colonoscopy patients in 2017 to determine whether the colonoscopies were completed and if a polyp was removed successfully and sent for pathological examination. Results: There were 376 patients with at least one adenoma and 635 with no adenoma detected (376/1011=37%) with the majority undergoing screening by academic gastroenterologists. Age (OR 2.4) and gender (OR 1.95) were primary risk factors in screening whereas age (OR 5.6) and race (OR 4.07) dominated surveillance. Non-AA patients had an increase in adenoma risk with an increase in BMI (OR 6.58) while AA patients had the opposite result (OR 0.32). AA patients undergoing surveillance were also more likely to have a polyp be an adenoma (78%) than Non-AA patients (37%). Conclusion: The fact that BMI in AA as compared to Non-AA patients was not associated with the risk of adenomas was an unexpected observation. The fact that if a polyp was found on surveillance in AA patients, it was more likely to be an adenoma than in Non-AA patients may suggest an increased emphasis on the importance of repeat colonoscopy after detection of an adenoma in AA patients at shorter intervals.
Introduction
Colorectal cancer (CRC) is a common cancer in the world with geographic variability in incidence, prevalence, and mortality [1]. Progression from polyps to adenoma, advanced adenoma and CRC provides the opportunity for interrupting the development of CRC by removal of polyps and histologically characterizing them [2, 3, 4, 5]. Thus, screening for colon cancer and removal of adenomas are critical for reducing the incidence of colon cancer. Unfortunately, screening rates are suboptimal and the rates of detection of adenomas are variable as a function of the physician performing the colonoscopy [6, 7]. An awareness of the role of various demographic factors in the risk for the adenomatous polyps and subsequent CRC are useful with respect to identifying populations and settings where improved screening and adenoma detection rates should be targeted. While individuals of African American (AA) race as compared to Non-AA are at higher risk for CRC, the racial disparity of other risk factors for CRC such as age, gender, and body mass index (BMI) are less characterized. The incidence of adenoma clearly correlates with risk of CRC but the comparative relationship between the presence of adenomas and age, gender, and body mass index (BMI) has not been consistently demonstrated among populations especially African Americans (AA) [8, 9, 10, 11, 12]. Also relevant to this study is that CRC identification and outcomes are influenced by racial disparities with respect to health care, making CRC and the genetics of race less clear [13, 14, 15]. The evaluation of racial differences in adenoma development addresses this important issue of cancer development biology, since the presence of adenomas which are the precursors to CRC should reduce the role of disparity in health care as it related to CRC detection.
The objective of this study was to evaluate the correlation of the presence of polyps and adenomas with respect to age, gender, and BMI in the context of AA as compared to Non- AA patients in the setting of colonoscopy screening and surveillance. Although male gender and age are risk factors in CRC, it is not clear where in the adenoma progression to cancer these risks are manifested. Also, increased body mass index (BMI) is a recognized risk factor for the development of CRC but its relationship to the presence of adenomas is less clear. Certainly, variations of the prevalence of adenomatous polyps in different patient populations have the potential to affect screening recommendations. Using predominately African American patients from an urban medical center endoscopy suite, we evaluated potential racial diversity between AA and non-AA patients with respect to age, gender and BMI and adenomas. Given the shared nature of the endoscopy suite, we could also evaluate whether there was a variation in ADR and these factors with respect to the three specialties in the suite (Academic gastroenterologists, non- Academic gastroenterologists and surgeons).
Methods
From a procedure-based population of 1095 patients undergoing screening or surveillance colonoscopy in the last
6 months of 2017, a retrospective medical chart review was conducted to determine whether the colonoscopies were complete and if a polyp was identified, it was successfully biopsied and sent for pathological examination. Data collected included age, race, gender, BMI, time of procedure, reason for procedure (screening or surveillance), physician specialty (academic gastroenterologist (A-GI), private gastroenterologist (P-GI) or surgeon (S)), number and size of polyps, and the pathology report (to define CRC, adenoma or no adenoma). The strict definition of Adenoma Detection Rate (ADR) is the number of patients with at least 1 adenoma divided by the total number of patients undergoing screening colonoscopies (AADR). We could also use our data to calculate, over all adenoma detection rates, surveillance adenoma rate (SAR) and polyp detection rate (PDR). Analysis was performed using JMP/SAS statistical analysis tools.
Results
Colonoscopy Patient Demographics and Procedures
The review of the 1095 patient charts found that 8 patients (0.7%) had polyps that were not biopsied, 6 patients (0.5%) had missing pathology and 62 patients (6%) did not have a completed colonoscopy. CRC was identified in 8 patients. All of them were undergoing a first-time screening colonoscopy (8/1096= 0.6%). The age range of cancer patients was from 46-65 with 7 AA and 1 non-AA. Thus, this final study population contains 376 patients with at least one adenoma and 635 with no adenoma detected (376/1011=37%). The majority (837) were for screening and most of the procedures were performed by academic gastroenterologists (AG-I (665); P-GI (176); Surgeons (172)). Most patients were African Americans (88%) with slightly more males as compared to females (54%). There was no difference in age by race or gender (59 years of age; range 46-73 years). The BMI (kg/m2) was slightly higher in females as compared to males (32.4±-0.3 vs 29.3±-0.33 p<0.005) and in AA as compared to non-AA (31.1±-0.2 vs 29.5±-0.65 p<0.02).
Adenoma Detection and Patient Characteristics
The presence of at least one adenoma was found in 283 (35%) out of 804 patients undergoing a screening colonoscopy and in 93 (45%) of the 207 patients undergoing surveillance (p<0.01). More patients with adenomas were identified by A-GI (47%) as compared to P-GI (24%) and Surgeons (15%) (p< 0.0001). Screening and surveillance colonoscopies are highly effective in preventing subsequent interval colon cancer through the identification and removal of potential adenomas. Thus, it was hypothesized that increasing age, AA race (AA> Non-AA), male gender (male>female) and increasing body weight index (high BMI>low BMI) would all influence the development adenoma’s which are the precursors to colorectal cancer (Table 1). Based on univariate analysis, age (OR 2.41) and gender (OR 1.95) were the dominant factors with respect to the presence of adenomas in the screening colonoscopies. With respect to surveillance colonoscopies, age (OR 5.6) and race (OD 4.07) were dominant with respect to adenoma risk. Since Academic GI (A-GI) had a higher ADR, Table 1 also presents the data for the A-GP physicians and the Low ADR physicians with results based on odds ratios similar to all physicians primarily due to the dominant number of A-GI physicians in the dataset. With respect to the BMI hypothesis, the results were in contrast to the hypothesis with an odd ration less than 1 indicating a higher BMI did not correlate with an increase in the detection of an adenoma. When all variables were samples simultaneously in the Nominal Logistic Fit Model for Adenoma vs No Adenoma the results were also similar to the univariate analysis (Table 2).
| All Colonoscopies | Screening (n= 804) | Surveillance (n=207) | ||
|---|---|---|---|---|
| Odds Ratio | p value | Odds Ratio | p value | |
| Age (older more adenomas) | 2.41 | 0.0064 | 5.76 | 0.0016 |
| Gender (M>F) | 1.95 | 0.0001 | 1.07 | NS (0.95) |
| Race (AA > Non-AA) | 1.32 | NS (0.24) | 4.07 | 0.0019 |
| BMI (Older more adenomas) | 0.34 | 0.018 | 1.27 | NS (0.77) |
| A-GI Colonoscopies | Screening (n= 533) | Surveillance (n=130) | ||
| Odds Ratio | p value | Odds Ratio | p value | |
| Age (older more adenomas) | 2.15 | 0.047 | 6.67 | 0.0058 |
| Gender (M>F) | 1.85 | 0.0005 | 1.16 | NS (0.76) |
| Race (AA > Non-AA) | 1.23 | NS (0.45) | 2.33 | NS (0.12) |
| BMI (Older more adenomas) | 0.57 | NS (0.27) | 1.16 | NS (0.91) |
| Low ADR Colonoscopies | Screening (n= 271) | Surveillance (n=77) | ||
| Odds Ratio | p value | Odds Ratio | p value | |
| Age (older more adenomas) | 5.39 | 0.01 | 15.36 | 0.022 |
| Gender (M>F) | 2.69 | 0.0017 | 1.2 | NS(0.73) |
| Race (AA > Non-AA) | 1.71 | NS(0.33) | 1 | NS(0.17) |
| BMI (Older more adenomas) | 1.11 | NS(0.91) | 0.79 | NS(0.85) |
Table 1: Univariate Analysis of Significance with Respect to Adenoma Detection.
| All Colonoscopies | Screening (n= 804) | Surveillance (n=207) | ||
|---|---|---|---|---|
| Odds Ratio | p value | Odds Ratio | p value | |
| Age (older more adenomas) | 1.03 | 0.005 | 1.07 | 0.0011 |
| Gender (M>F) | 1.93 | 0.0001 | 1.28 | NS (0.43) |
| Race (AA > Non-AA) | 1.4 | NS (0.16) | 4.69 | 0.0007 |
| BMI (Older more adenomas) | 0.54 | NS (0.15) | 1.02 | NS (0.31) |
| A-GI Colonoscopies | Screening (n= 533) | Surveillance (n=130) | ||
| Odds Ratio | p value | Odds Ratio | p value | |
| Age (older more adenomas) | 2.5 | 0.02 | 6.09 | 0.008 |
| Gender (M>F) | 1.95 | 0.0004 | 1.2 | NS (0.64) |
| Race (AA > Non-AA) | 1.2 | NS (0.49) | 2.12 | NS (0.21) |
| BMI (Older more adenomas) | 0.83 | NS (0.71) | 1.92 | NS (0.55) |
| Low ADR Colonoscopies | Screening (n= 271) | Surveillance (n=77) | ||
| Odds Ratio | p value | Odds Ratio | p value | |
| Age (older more adenomas) | 5.47 | 0.013 | 33.9 | 0.0059 |
| Gender (M>F) | 2.65 | 0.0034 | 2.35 | NS(0.18) |
| Race (AA > Non-AA) | 2.11 | NS(0.17) | 100 | 0.0005 |
| BMI (Older more adenomas) | 0.91 | NS(0.91) | 1.1 | NS(0.94) |
Table 2: Multivariate Logistic Fit Analysis with Respect to Adenoma Detection.
Racial Disparity in Adenoma Detection
To assess disparity by race, we evaluated the correlation of Age, BMI and Gender as factors which could influence the presence of adenomas by race. The evaluation based on the similarities between endoscopists was primarily for all endoscopists with the patients stratified by screening vs surveillance. In most instances an additional assessment was also for only the high performing academic gastroenterologists.
Gender and Race
The influence of gender stratified by race and screening or surveillance, was assessed and the results presented in Figure 1. Males were more likely than females to have tumors (Odds ratio from 2.02 to 1.14), but the difference was statistically significant only in AA males undergoing screening colonoscopies. When only the high ADR performing A-GI physician data was use, a similar result was seen (Screening: AA OR= 1.97; p=0.0003 vs Non-AA OR= 1.01; p= 0.98; Surveillance: AA OR= 1.16; p= 0.69 vs Non-AA OR= 1.6; p= 0.66).
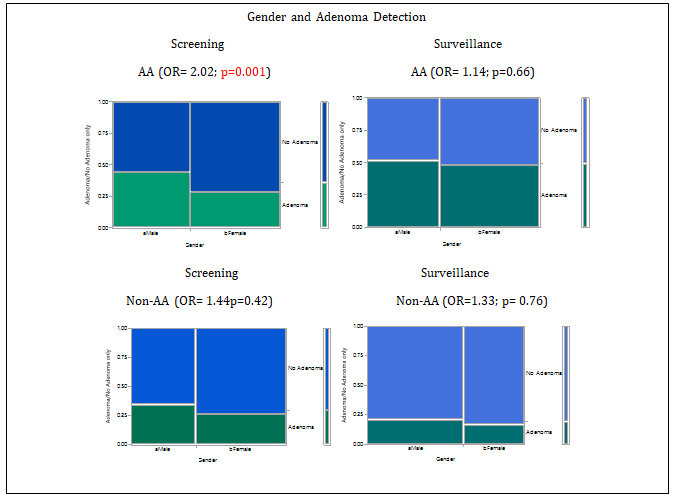
Figure 1: Racial diversity for gender and the detection of adenoma by all providers for both screening and surveillance colonoscopies. Patients are defined as either having or not having at least one adenoma. Male individuals had significantly higher adenoma rates compared to females in the AA Screening group (p=0.001 vs 0.66). Although males were more likely to have adenomas in the other groups the difference did not achieve significance. The width of the mosaic plot bars represents the distribution of the number of patients and was similar except for more males in the Non-AA surveillance group. OR is the Odds Ratio and significance is presented as p value for Pearson ChiSquare analysis.
Age and Race
Regardless of race (AA vs Non-AA) or procedure (screening vs surveillance), increasing age resulted in a higher likelihood of detecting an adenoma (Figure 2). When the statistical significance of the fit was evaluate using whole model logistic fit analysis, AA patients had a steeper curve and a statistically significant fit of the curve whereas Non-AA did not (Figure 2a). A similar observation was made when using age greater/equal to vs less than 60 years (Figure 2b). As with gender, the data suggests a racial difference in that age was more likely to correlate with a significant increase in adenomas in AA patients as compared to Non-AA patients.
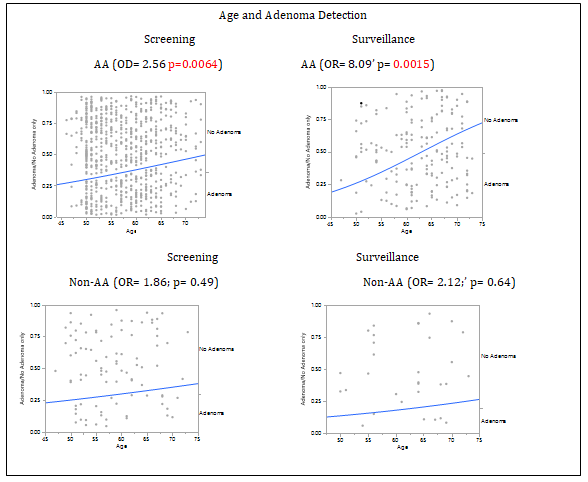
Figure 2a: Racial diversity for adenoma presence as a function of age. The data is for screening and surveillance colonoscopies performed by all providers and stratified by race. Patients are defined as either having or not having at least one adenoma. Age on the x-axis is treated as a continuous variable. The significance of the fit line is also presented for the graphs which represent the logistic fit model.
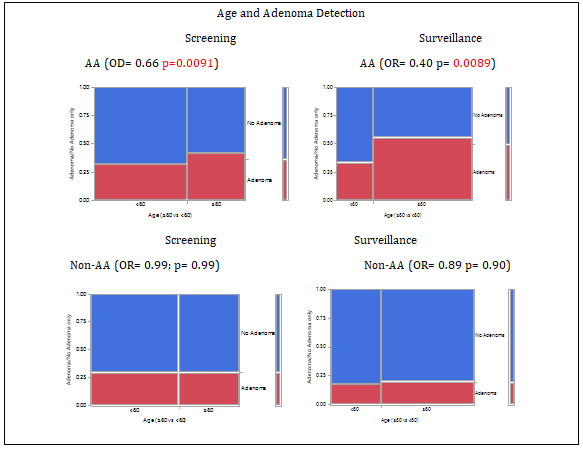
Figure 2b: Racial diversity for adenoma presence as a function of age. Patients were classified by their age using the cut off for the mid-range of AA males as demonstrated in figure 5a. On the mosaic plot, the width of the bars represents the population age distribution which is slightly greater for the surveillance as compared to the screening colonoscopies for both races. The data is for all providers and the odds ratio is for age <60 vs ≥60 years of age indicating fewer adenomas in the younger patients only in the AA patients. The p values represent the Pearson ChiSquare correlation significance.
BMI and Race
As shown in Figures 3-5, AA and Non-AA differ dramatically with respect to the influence of BMI on the presence of adenomas in both screening and surveillance colonoscopies. While Non-AA patients have an increase in adenomas detected with increasing BMI, AA patients have a decrease. This was true for BMI as a continuous variable (Figure 3) or when categorized as obese, overweight or normal (Figure 4). Similar results were found for all procedures and providers (AA OR= 0.32; p=0.035) vs Non-AA OR= 6.58) and for high performing Academic-GI colonoscopies for both screening (AA OR= 0.43 vs Non-AA OR= 3.73) and surveillance (AA OR= 0.49 vs Non-AA OR= 2.9) we also used all patients and all providers to evaluate whether gender might influence the results. As shown in Figure 5a & b, the racial difference for BMI was apparent in both genders.
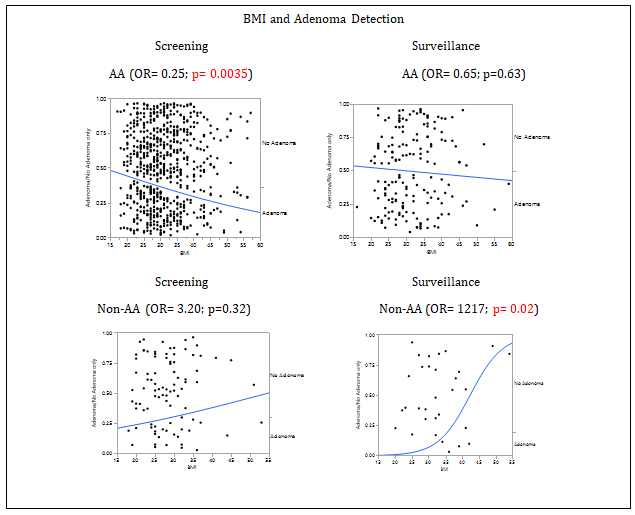
Figure 3: Racial Diversity for the presence of adenoma as a function of body weight. The data is plotted for the patients with or without an adenoma undergoing screening or surveillance colonoscopies by all providers as a function of body weight. The Odds Ratio (OR) and significance are presented for each graph. The OR less than one indicates an inverse relationship of ADR with BMI. The line represents the best line for the correlation between BMI and adenoma detection and the p value is for the closeness of the fit using the logistic fit model.
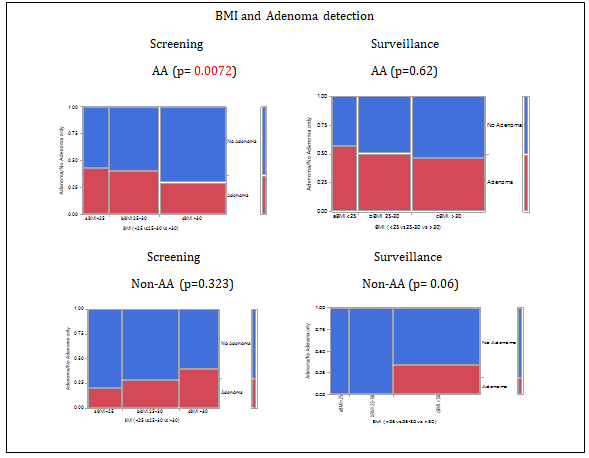
Figure 4: Racial Diversity for the presence of adenoma as a function of body weight classification. Patients were classified by their body weight using the typical categories: Normal (<25), Overweight (25-30) and Obese (>30). On the mosaic plot, the width of the bars represents the population distribution which as primarily overweight and obese for both races. The data is presented for patients with or without an adenoma undergoing screening or surveillance colonoscopies by all providers as a function of body weight classifications. The p values represent the Pearson ChiSquare correlation significance.
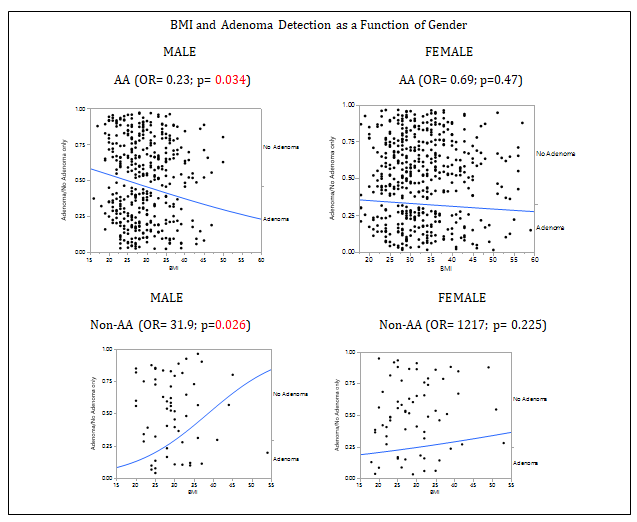
Figure 5a: Racial diversity for the presence of adenoma as a function of body weight and gender. The data is for all patients undergoing either a screening or surveillance colonoscopies by all providers since the BMI trends were similar for screening and surveillance. The Odds Ratio (OR) and significance are presented for each graph. The OR less than one indicates an inverse relationship of ADR with BMI. The line represents the best line for the correlation between BMI and adenoma detection and the p value is for the closeness of the fit using the logistic fit model.
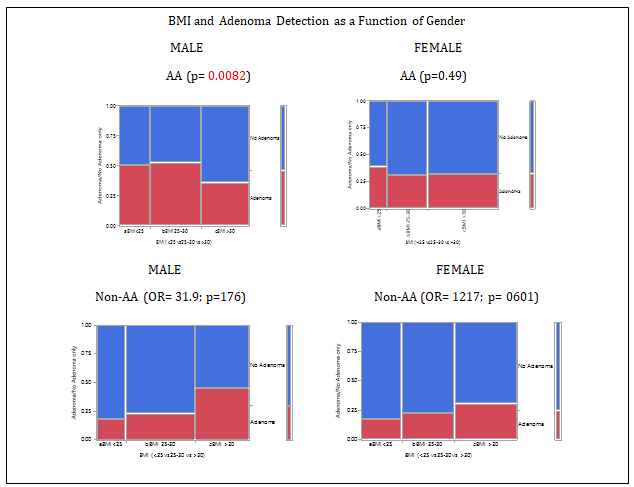
Figure 5b: Racial Diversity for the presence of adenoma as a function of body weight classification and gender. Patients were classified by their body weight using the typical categories: Normal (<25), Overweight (25-30) and Obese (>30). On the mosaic plot, the width of the bars represents the population distribution which is primarily overweight and obese for both races. The data is for patients undergoing either a screening or surveillance colonoscopies by all providers since racial diversity was similar between screening and surveillance as a function of BMI. The p values represent the Pearson ChiSquare correlation significance.
Race and Likelihood of Adenomatous Polyp
While the detection of adenomas was a key focus of the study, we also evaluated the relationship between race and the likelihood that a polyp would be an adenoma. As shown in Table 3, the largest variation between AA and Non-AA patients undergoing surveillance colonoscopy (78% vs 37% p<0.005). For the other settings the range was not significantly different (i.e., between 58% and 69%). This observation is confirmed by calculating the variation between polyps and adenomas in surveillance for AA as compared to non-AA (62% polyps vs 52% polyps p=0.24 as compared to 49% adenomas vs 21% adenomas).
| All Colonoscopies | |||||
|---|---|---|---|---|---|
| All Colonoscopies | AA | 243/501=67% | Non-AA | 33/57=58 | NS(p= 0.156) |
| Screening | AA | 256/399=64% | Non-AA | 27/41=66% | NS(p=0.829) |
| Surveillance | AA | 87/11=78% | Non-AA | 6/16=37% | p=0.0006 |
| High ADR A-GI | |||||
| All Colonoscopies | AA | 279/388=72% | Non-AA | 27/47=62% | NS(p=0.146) |
| Screening | AA | 209/302=69% | Non-AA | 23/34=68% | NS(p=0.852) |
| Surveillance | AA | 70/89=81% | Non-AA | 6/7=46% | p=0.005 |
Table 3: Racial Disparity in Percent of Polyps which are Adenomas.
Discussion
As predicted based on the literature, increasing age and male gender were both positive predictors in patients undergoing screening colonoscopies while BMI and race were not with respect to the detection adenomas in an endoscopy suite with predominately African American patients, we found the only setting where race was an independent predictor was in patients undergoing surveillance due to a previous adenoma detected on screening. The fact that polyps from AA surveillance patients were more likely to be adenomas than from non-AA patients undergoing surveillance at our study is important with respect to race and surveillance risk. The lack of race to be an independent factor in the detection of adenomas in screening colonoscopies but to be significant in surveillance suggests that the biology of adenoma development may be different and account for the observation that AA patients are more likely to be diagnosed with CRC that non-AA patients.
In contrast to most of the previous studies, we made a distinction between screening and surveillance colonoscopies. With respect to patients undergoing surveillance primarily due to a previous positive adenoma occurrence while age was clearly significant, the fact that AA patients were more likely than non-AA to have an adenoma detected on their repeat colonoscopy is novel and important. The fact that AA patients have a higher odds ratio for the presence of adenoma (4.07 vs 2.33) clearly suggests that extra effort to have AA patients who have previously had an adenoma should be encouraged to have a regular follow up. Whether this should have an impact with respect to having AA patients returning sooner than Caucasians are debatable given that both have a high odds ratio for finding adenomas. With respect to gender and the risk of adenoma in contrast to Non-AA where there was no gender difference, African American males are more likely to have an adenoma as compared to females in screening populations. The reason Non-AA individuals do not have a gender difference is puzzling given the known risk of gender for CRC. However, it may just be that a larger sample of Non-AA patients will be required to generate a statistical difference.
Our observation on screening colonoscopy patients provides another set of data to an ongoing controversy with respect to race and adenomas. David, et al. and Collazo, et al. both reported finding like ours with respect to screening [7, 16, 17, 18]. In contract several other studies found the opposite to be true [19, 20, 21, 22]. The reason for this variation in findings when comparing across studies may be due to inherent biases that are not apparent. Among the possibilities are that African Americans are different than Caribbean Blacks and the rations are different in various studies, there may be variations in adenoma detection rates in studies where multiple centers with different ADR contributed to the data set and that there are variations in gender ratios and age distribution between studies. Given our observation with respect to the opposite effect of BMI variations in BMI between groups may also play a role? Our study is single centered, has similar gender ratios and age and there was no difference between the whole group of physicians and when data analysis was restricted to the high ADR academic gastroenterologists.
The most dramatic observation with respect to racial differences occurred in the comparison of the effect of BMI on the detection of adenoma. The Non-AA patients were more likely to have adenomas as body weight increased as compared to AA patients where the opposite was true. This clearly contributes to the overall observation that BMI was not an independent predictor of adenoma in the whole population. With respect to the literature, a meta-analysis by Wong, et al. found that White and Asian patients had a positive correlation and AA patients had a negative correlation. Since most of the studies in the meta-analysis were rich in Asian patients, the odds ration variability between the White and AA patients (1.42 vs 0.88) did not reach statistical significance. A similar issue with respect to AA patients and BMI was found in several different studies including one using a large database which reflected the US population distribution and was thus low in AA patients [9, 23]. Also, in contrast to most of the literature, this study reduces the role of variation in endoscopists by also reporting the data for high adenoma detection rate academic GI physicians in a homogeneous population with respect to gender and age. The reason that AA patients have fewer adenomas as body weight increases is not clear and has not been addressed adequately in the literature. Possible explanations for these variations with respect to AA vs Non-AA in adenoma detection as a function of BMI include, differences in the distribution of adipose tissue, variation in microbiome in the large intestine, variations in diet, and the potential that despite the decrease in adenomas there may be an increased likely hood of a more rapid progression to CRC [9, 12]. Whether this suggests a need to modify repeat colonoscopy recommendations based on race cannot be determined by our study.
The primary outcome of this study is the observation that while racial differences in adenoma risk can be identified, the fact that AA patients overall do not have more adenomas than Non-AA patients suggests that health care disparity with respect to colon cancer screening probably plays the major role in the fact that AA patients are more likely to be diagnosed with CRC than Non-AA patients. As a result of the large AA population in this study, it was also determined that in contrast to Non-AA patients, BMI was inversely correlated with the detection of adenomas. While the significance of this observation with respect to obesity and cancer is unclear, future investigation of the reason for this disparity warrants investigation. The most important observation was that not only is AA race as compared to Non-AA a more significant risk factor for adenomas on surveillance, but the polyp was more likely to be an adenoma than in Non-AA patients. This supports the need to emphasize that AA patients with even small tubular adenomas on screening should be seen at 3-5 years intervals as opposed to Non-AA where a 7-10 years intervals can be comfortably recommended. Our data demonstrated that AA patients are not at higher risk than Non-AA patients at screening but do have an increased risk upon surveillance due to a previous adenoma, warrants an increased emphasis on the importance of repeat colonoscopy at shorter intervals after detection of an adenoma in AA patients.
References
-
Sung H, Ferly J, Siegel RL, Laversanne M, Soerjomataram I, et al. (2021) Global cancer statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71(3): 209- 249.
-
Winawer SJ, Zauber AG, Ho MN, O’Brien MJ, Gottlieb LS, et al. (1993) Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med 329(27): 1977-1981.
-
Corley DA, Levin TR, Doubeni CA (2014) Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med 370(26): 2541.
-
Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, et al. (2017) Colorectal cancer screening: recommendations for physicians and patients from the u.s. Multi-society task force on colorectal cancer. Am J Gastroenterol 112(7): 1016-1030.
-
Kaminski MF, Wieszczy P, Rupinski M, Wojciechowska U, Didkowska J, et al. (2017) Increased rate of adenoma detection associates with reduced risk of colorectal cancer and death. Gastroenterology 153(1): 98-105.
-
Cavicchi M, Tharsis G, Burtin P, Cattan P, Venezia F, et al. (2019) Difference in physicianand patientdependent factors contributing to adenoma detection rate and serrated polyp detection rate. Dig Dis Sci 64(12): 3579-3588.
-
David Y, Ottaviano L, Park J, Iqbal S, Likhtshteyn M, et al. (2019) Confounders in adenoma detection at initial screening colonoscopy: a factor in the assessment of racial disparities as a risk for colon cancer. J Cancer Ther 10(4): 269-289.
-
Wong MCS, Lam TY, Tsoi KK, Chan VCW, Hirai HW, et al. (2014) Predictors of advanced colorectal neoplasia for colorectal cancer screening. Am J Prev Med 46(5): 433- 439.
-
Dore MP, Longo NP, Manca A, Pes GM (2020) The impact of body weight on dysplasia of colonic adenomas: a case- control study. Scand J Gastroenterol 55(4): 460-465.
-
Roy HK, Bianchi LK (2009) Differences in colon adenomas and carcinomas among women and men: potential clinical implications. JAMA 302(15): 1696-1697.
-
Penn E, Garrow D, Romagnuolo J (2010) Influence of race and sex on prevalence and recurrence of colon polyps. Arch Intern Med 170(13): 1127-1132.
-
Wong MC, Chan CH, Cheung W, Fung DH, Liang M, et al. (2018) Association between investigator-measured body-mass index and colorectal adenoma: a systematic review and meta-analysis of 168,201 subjects. Eur J Epidemiol 33(1): 15-26.
-
Lieberman DA, Holub JL, Moravec MD, Eisen GM, Peters D, et al. (2008) Prevalence of colon polyps detected by colonoscopy screening in asymptomatic black and white patients. JAMA 300(12): 1417-1422.
-
Laiyemo AO, Doubeni C, Pinsky PF, Doria-Rose VP, Bresalier R, et al. (2010) Race and colorectal cancer disparities: health-care utilization vs different cancer susceptibilities. J Natl Cancer Inst 102(8): 538-546.
-
Augustus GJ, Ellis NA (2018) Colorectal cancer disparity in African Americans: risk factors and carcinogenic mechanisms. Am J Pathol 188(2): 291-303.
-
Jawitz NG, Gellad ZF, Lin L, Wood RK, Leiman DA, et al. (2020) Patient, physician and procedure characteristics are independently predictive of polyp detection rates in clinical practice. Dig Dis Sci.
-
Collazo TH, Jandorf L, Thelemaque L, Lee K, Itzkowitz SH, et al. (2015) Screening Colonoscopy among Uninsured and Underinsured Urban Minorities. Gut Liver 9(4): 502- 508.
-
Nouraie M, Hosseinkhah F, Zamanifekri B, Brim H, Smoot DT, et al. (2010) Clinicopathological features colon polyps from African Americans. Dig Dis Sci 55(5): 1442- 1449.
-
Thornton JG, Morris AM, Thornton JD, Flowers CR, McCashland TM, et al. (2007) Racial variation in colorectal polyp and tumor location. J Natl Med Assoc 99(7): 723-728.
-
Rex DK, Khan AM, Shah P, Newton J, Cummings OW, et al. (2000) Screening colonoscopy in asymptomatic average- risk African Americans. Gastrointest Endosc 51(5): 524- 527.
-
Lebwohl B, Capiak K, Neugut AI, Kastrinos F (2012) Risk of colorectal adenomas and advanced neoplasia in Hispanic, black and white patients undergoing screening colonoscopy. Aliment Pharmacol Ther 35(12): 1467- 1473.
-
Murphy CC, Martin CF, Sandler RS (2015) Racial differences in obesity measures and risk of colorectal adenomas in a large screening population. Nutr Cancer 67(1): 98-104.
-
Kobiela J, Wieszczy P, Reguła J, Kamiński MF (2018) Association of obesity with colonic findings in screening colonoscopy in a large population-based study. United European Gastroenterology J 6(10): 1538-1546.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient