Bone Lysis Revealing Primary Malignant Melanoma of the Esophagus: Case Report and Review of the Literature
Primary malignant melanoma of the esophagus is a rare, very aggressive entity with a bad prognosis. It is metastatic in 40 to 80% of cases at diagnosis. The symptoms are non-specific and the diagnosis is confirmed by histology. The treatment of choice is surgery in the early forms. We report the case of a metastatic primary melanoma of the esophagus discovered by retro sternal pain.
Introduction
Primary esophageal malignant melanoma is a very aggressive tumor with a bad prognosis and a very rare entity that accounts for only 0.1–0.2% of all primary esophageal malignancies [1]. We report the case of a primary esophageal melanoma in a 56-year-old patient discovered by chronic retro sternal pain, with bone metastases but no dysphagia.
Case Report
56-year-old patient with no particular pathological history, presented with atypical retro-sternal pain without dysphagia, evolving in a context of deterioration of the general condition. There was chronic dorso-lumbar bone pain, evolving for 3 months without motor or sensory deficit and without sphincter disorders. No history of trauma. The examination was unremarkable, notably no skin-mucous pigmentary lesions or peripheral lymphadenopathy. An eso- gastro-duodenal fibroscopy showed extensive pigmentary lesions in middle and distal third of the esophageal mucosa (Figure 1). Biopsies were performed. Rest of the endoscopic exploration, in particular gastric and duodenal, was without abnormalities.
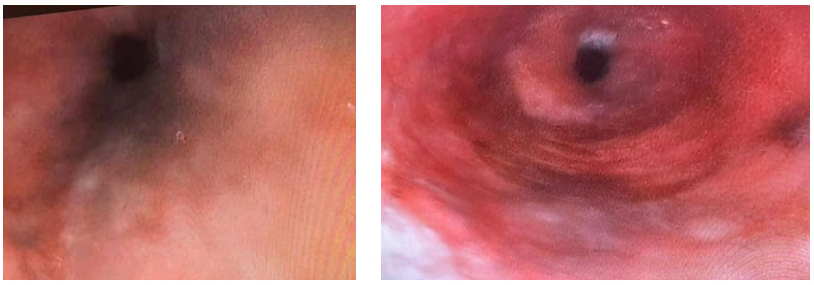
Figure1: Endoscopic appearance of pigmented lesions in the esophagus.
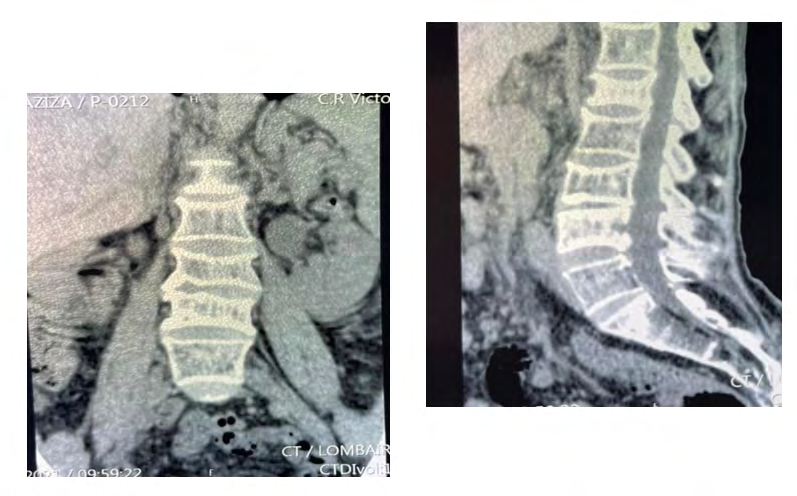
Thoraco-abdominal-pelvic CT and MRI dorso-lumbar revealed secondary lytic lesions of the dorsolumbar bone, without other parenchymal metastases (Figure 2).
The confirmation of the melanoma was provided by the histopathological study of esophageal biopsies objectifying diffuse layers of melanocytic cells with the histochemical complement compatible with a malignant melanoma.
Discussion
Primary malignant melanoma of the esophagus is a rare, very aggressive and often metastatic at presentation, associated with poor prognosis of the patient. It presents clinically like all other malignant tumors of the esophagus, with retro sternal pain, dysphagia, digestive hemorrhages, deterioration of the general condition or with metastasis, revealing the primary melanoma of the esophagus. Most of the described cases of primary esophageal melanoma present endoscopically as an intraluminal polypoid mass in the middle or distal third of the esophagus which may or may not be pigmented, usually single, although in 12% of cases the lesions are multiple [2]. Melanoma can present as a pink or red lesion instead of a pigmented lesion, which could be misdiagnosed as benign or other malignant tumors [3]. The diagnosis is difficult when the biopsy fragments lack melanin [4], in which case the definitive diagnosis could be obtained by positive staining of HMB45, melanin A, S100 and specific enolase of the neurons [5]. Differential diagnosis encompasses the spindle cell variant of squamous cell carcinoma, sarcomas, small cell carcinoma, carcinosarcoma and metastatic melanoma to the esophagus [6]. Distant metastases are common, 40 to 80% at the time of diagnosis [5], the organs most affected are: the liver, mediastinum, lungs and brain [2]. The 1-year and 5-year survival rates for these patients are 51% and 10%, respectively [7]. The treatment of choice is surgical excision with discretionary lymphadenectomy for operable melanomas, since lymph node metastases are an independent prognostic factor [8]. Total or near-total esophagostomy offering the best survival result (5 years against 9 months for local resection) [1]. There is a role for immunomodulatory therapy in patients with metastatic disease and for palliative external beam radiation therapy in patients with unrespectable esophageal melanoma [9]. The most recent treatment modalities, such as intraluminal brachytherapy and laser photo ablation have shown great promise, but are potentially toxic, causing esophagitis, ulcerations [10, 11].
Conclusion
Primary malignant melanoma of the esophagus is a rare and very aggressive tumor with a bad prognosis and poor survival even after surgery. It is highly metastatic, in 40 to 80% of cases at presentation. Esophagectomy with systematic lymphadenectomy is the treatment of choice in early forms, immunotherapy in metastatic forms and palliative radiotherapy in inoperable forms.
References
-
Sabanathan S, Eng J, Pradhan GN (1989) Primary malignant melanoma of the esophagus. Am J Gastroenterol 84(12): 1475-1481.
-
Chalkiadakis G, Wihlm JM, Morand G, Bousson MW, Witz JP (1985) Primary malignant melanoma of the esophagus**.** Ann Thorac Surg 39(5): 472-475.
-
Kibbi N, Kluger H, Choi JN (2016) Melanoma: clinical presentations. Cancer Treat Res 167: 107-129.
-
Chang F, Deere H (2006) Esophageal melanocytosis morphologic features and review of the literature. Arch Pathol Lab Med 130(4): 552-557.
-
Iwanuma Y, Tomita N, Amano T, Isayama F, Tsurumaru M, et al. (2012) Current status of primary malignant melanoma of the esophageal: clinical features, pathology, management and prognosis. J Gastroenterol 47(1): 21- 28.
-
DiCostanzo DP, Urmacher C (1987) Primary malignant melanoma of the esophagus. Am J Surg Pathol 11(1): 46- 52.
-
Gao S, Li J, Feng X, Shi S, He J (2016) Characteristics and surgical results of primary malignant melanoma of the esophagus. Sci Rep 6: 23804.
-
Wang S, Tachimori Y, Hokamura N, Igaki H, Kishino T, et al. (2013) Diagnosis and surgical outcomes for primary malignant melanoma of the esophagus: a single-center experience. Ann Thorac Surg 96(3): 1002-1006.
-
Fogarty GB, Tartaglia CJ, Peters LJ (2004) Primary melanoma of the oesophagus well palliated by radiotherapy. Br J Radiol 77(924): 983-1085.
-
Tessa M, Rotta P, Ragona R, Sola B, Grassini M, et al. (2005) Concomitant chemotherapy and external radiotherapy plus brachytherapy in locally advanced esophageal cancer: results of a retrospective multicenter study. Tumori J 91(5): 406-414.
-
Wayman J, Irving M, Russell N, Nicoll J, Raimes SA (2004) Intraluminal radiotherapy and Nd: YAG laser photoablation for primary malignant melanoma of the esophagus. Gastrointest Endosc 59(7): 927-929.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient