Gastrointestinal Stromal Tumor Revealed by Hemorrhagic Shock
Gastrointestinal stromal tumors (GISTs) are rare tumors of the digestive tract. The small intestine is the second most frequent localization of GIST after the stomach. We report a case of ileal stromal tumor. The patient was admitted with a picture of hemorrhagic shock due to massive rectal bleeding. The fibroscopy performed after stabilization was not objectified at the origin of the document while the CT scan objectified a mass of tissue density at the level of the right iliac fossa. Given the increasing evolution with the recurrence of patients to a target of a laparotomy for diagnostic and therapeutic purposes objectifying the tumor of the right iliac fossa at the expense of the ileum. The surgical procedure consisted of a major segmental resection of the tumor with ileo-ileal anastomosis. The anatomopathological study confirmed the diagnosis of stromal tumor with good evolution. Through a general review of the literature, we have described the various clinical, para-clinical, anatomopathological, prognostic and current therapeutic aspects specific to these tumors.
Introduction
Gastrointestinal stromal tumors or GIST are relatively rare pathologies well known in terms of digestive surgery [1]. Currently, their management is well codified with the availability of sophisticated diagnostic and therapeutic means [2, 3]. The objective of this work was to report the case of an ileal GIST in a 67-year-old patient revealed by massive rectal bleeding responsible for hemorrhagic shock.
Case Report
Patient Information
A 67-year-old man was admitted to the emergency department for heavy rectal bleeding for 1 week with profound asthenia and dyspnea without other manifestations.
He had a history of active smoking and occasional alcoholism. He was not taking any medication. He had no drug allergies.
Clinical Results
On clinical examination, he was asthenic, pale with a diuresis of 300 ml/24 hours. Her temperature was 37.5◦C, her blood pressure 90/50 mmHg and her heart rate 110 beats per minute. The abdomen was tender at the level of the right iliac fossa, without defense or contracture. On digital rectal examination, the finger cot had come back stained with red blood. The rest of the exam was normal.
Diagnostic Approach
Blood tests showed marked anemia with an Hb of 5.3 g/dL (MCV 83 fL) with normal platelets at 360,000 /mm3
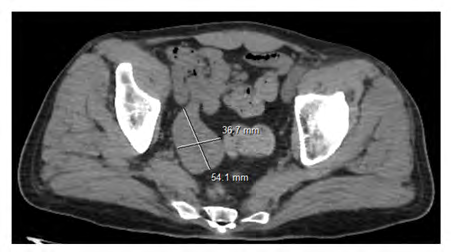
and a normal haemostasis assessment. On the second day of admission, a gastroscopy was performed which showed an aspect of erythematous pangastritis but without signs of recent bleeding. The total colonoscopy, for its part, did not objectify macroscopic anomalies apart from the bloody lake which lines the entire colonic mucosa. Abdominal CT had objectified a pelvic mass of tissue density, necrotic in the center, measuring 5x3.5cm in long axis communicating with the ileal loop (Figure 1).
Therapeutic Interventions and Follow-up
An exploratory laparotomy was performed which revealed a tissue mass at the expense of an ileal loop, measuring 4 x 5cm, with exophytic development, located 1 meter from the ileo-coecal junction. The procedure consisted of resection of the mass removing 5 hail on either side of the mass with end-to-end anastomosis (Figure 2).
Histology revealed a GIST with healthy resection margins and no lymph node invasion. Immunohistochemistry was positive for c-kit (CD117) and CD34 immunomarkers. The proliferation marker Ki67 marks 5% of the nuclei. Mitotic activity was less than 5/25 on high power fields. The risk of recurrence was moderate according to Miettinen and Lasota. The patient is followed regularly in consultation.

Discussion
Gastrointestinal stromal tumors (GIST) are primary digestive mesenchymal tumors that appear to develop from the interstitial cells of Cajal in the myenteric plexus, and express a KIT transmembrane receptor [4]. The age of onset of these tumors is between 50 and 70 years old, with a male predominance. The main risk factors are represented by neurofibromatosis type 1 and Carney’s triad [5]. They can affect the entire digestive tract with decreasing frequency from the stomach to the rectum. The stomach and small intestine are the most common locations. Other locations can be seen: greater omentum, mesentery, retroperitoneum. Small bowel stromal tumors appear most frequently in the jejunum, then the ileum and duodenum [5]. Symptoms vary depending on location. Thus, they can be asymptomatic and discovered by chance or manifest themselves by digestive bleeding, abdominal pain or, more rarely, by occlusive syndromes or perforations of the digestive tract [6, 7, 8]. From a Para clinical point of view, the video capsule is common practice in the management of ileal tumors with intraluminal growth [9]. The other option was CT, which guided management in our case. It is especially essential preoperatively to characterize the exophytic development of the tumor mass, to assess whether or not the lesions are respectable, to detect any metastasis or peritoneal carcinomatosis and to choose the surgical approach [2].
In terms of treatment of GISTs, complete surgical resection remains the only potentially curative treatment. A margin of 1 to 2 cm is recommended by most teams [2, 3, 10]. Lymph node dissection is not systematic because lymph node metastases are rare (less than 10%) and the risk of lymph node recurrence is limited (less than 5%) [10]. Radiotherapy and cytotoxic chemotherapy are ineffective in GISTs and are used only in refractory diseases for palliative purposes. Imatinib mesylate, a targeted therapy as a tyrosine kinase inhibitor of c-KIT and PDGFR-a, has become the standard treatment not only for relapsed or metastatic GISTs, but also for adjuvant treatment in adult patients after complete resection of KIT-positive GISTs [11, 12].
Conclusion
In conclusion, we presented a case of intestinal GIST responsible for hemorrhagic shock, which is rarely encountered in current practice. Intestinal GIST should be among the diagnostic hypotheses in patients with gastrointestinal bleeding of unknown origin and requires the realization of different endoscopic and radiological diagnostic modalities to detect the source of bleeding.
Authors Contributions: All authors contributed to this work. All have read and approved the final version of the manuscript.
Informed Consent: The patient declared his consent freely and in an informed way, in order to allow the realization and the publication of this manuscript.
References
-
Coindre JM, Emile JF, Monges G, Vince DR, Scoazec JY (2005) Gastrointestinal stromal tumors: definition, histological, immunohistochemical, and molecular features, and diagnostic strategy. Ann Pathol 25(5): 358- 385.
-
Obiol RM, Albir G, Mozos FL, Serrano JO (2013) Surgical treatment of gastrointestinal stromal tumours. Analysis of our experience. Cir Esp 91(1): 38-43.
-
Raventós VA, Pousa AL, Medina LO, Argüelles ADDL, Hernández JAF, et al. (2013) Primary, Non-metastatic Gastrointestinal Stromal Tumor Surgery: Results of the GRISK Study. Cir Esp 91(2): 96-102.
-
Rubin BP, Singer S, Tsao C, Duensing A, Lux ML, et al. (2001) KIT activation is a ubiquitous feature of gastrointestinal stromal tumors. Cancer Res 61(22): 8118- 8121.
-
Gupta P, Tewari M, Shukla HS (2008) Gastrointestinal Stromal Tumor. Surg Oncol 17(2): 129-138.
-
Balaton AJ, Coindre JM, Cvitkovic F (2001) Tumeurs stromales digestives. Gastroenterol Clin Biol 25: 473- 482.
-
Miettinen M, Lasota J (2006) Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med 130(10): 1466-1478.
-
Tateishi U, Hasegawa T, Satake M, Moriyama N (2003) Gastrointestinal stromal tumor. Correlation of computed tomography findings with tumor grade and mortality. J Comput Assist Tomogr 27(5): 792-798.
-
Serraj I, Amrani L, Atitar I, Kanouni N, Al Baroudi S, et al. (2008) Obscure gastrointestinal bleeding due to jejunal stromal tumor: the contribution of capsule endoscopy. Gastroenterol Clin Biol 32(12): 1022-1024.
-
Hueman MT, Schulick RD (2008) Management of gastrointestinal stromal tumors. Surgical Clinics of North America 88(3): 599-614.
-
GLEEVEC (2001) Highlights of Prescribing Information.
-
Eisenberg BL, Harris J, Blanke CD, Demetri GD, Heinrich MC, et al (2009) Phase II trial of neoadjuvant/adjuvant imatinib mesylate (IM) for advanced primary and metastatic/recurrent operable gastrointestinal stromal tumor (GIST): early results of RTOG 0132/ACRIN 6665. Journal of Surgical Oncology 99(1): 42-47.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient