GERD and Its Association with BMI in Adult Patients Undergoing Upper GI Endoscopy at the Kenyatta National Hospital
Background: Gastroesophageal reflux disease (GERD) is a common clinical problem affecting millions of people worldwide. GERD is highly prevalent in morbidly obese patients and a high body mass index (BMI) is a risk factor for this condition. However, there is differing data on the use of BMI as a predictor of GERD, its severity and frequency. We therefore aimed to determine the association between GERD and high BMI and to document the esophageal mucosal changes in these patients during endoscopy. Methodology: We conducted a cross-sectional study among the 174 GERD patients to investigate the association between BMI and GERD at Kenyatta National Hospital endoscopy unit. Patients aged 18 years and above presenting with classical symptoms of GERD were evaluated upon voluntary enrolment. Ethical approval was sought from the KNH-UON ethics& research committee. A questionnaire was administered with demographic data (age, gender, weight, height) and specific questions assessing for GERD. At endoscopy, the mucosal changes were recorded. Data was then summarized using means, frequencies and proportions. Association between patient demographics and GERD was evaluated using the Student t-test or Mann–Whitney U test for continuous variables. Chi-square analysis was applied for categorical variables. A p-value of
Introduction
Gastroesophageal Reflux disease is a common clinical problem affecting millions of people worldwide [1, 2]. Its typical manifestations are heartburn and/or regurgitation. GERD can further be classified into erosive GERD and non- erosive GERD based on the endoscopic appearance of the esophageal mucosa [3]. Significant complications of GERD include; esophagitis, stricture formation, adenocarcinoma, respiratory and ear, nose and throat (ENT) disorders [4]. Due to increasing prevalence, its epidemiology has been a subject of growing interest [2, 5]. Obesity is associated with GERD [6, 7]. Overweight and obesity are defined as excessive fat accumulation in the body posing a risk to health. Body mass index, which is calculated as weight in kilograms divided by height in meters squared is used as a marker of obesity. A BMI value 25–30 represents overweight and BMI >30 indicates obesity. A BMI value <25 is considered as normal. Some studies have shown that GERD is highly prevalent in patients who are morbidly obese and that a high BMI is a risk factor for this condition [8, 9, 10, 11, 12]. Epidemiologic data also demonstrates that overall obesity is a risk factor for esophageal adenocarcinoma [2]. Globally, obesity has become a major health problem and its prevalence is increasing both in the developed and developing countries [13, 14]. In Kenya, urbanization appears to be an important determinant in obesity [15, 16]. There is differing data on the use of BMI as a predictor of GERD, its severity and frequency. In western countries, some studies have shown a positive correlation between high BMI and frequency of reflux [10, 17], others have demonstrated a weak association [18] and others show no association [19, 20]. A study done in 2019 on the black population of South Africa showed that GERD was more common in black females than males and the prevalence rose with increasing BMI [21]. In Kenya, a focal study on the management of GERD was published by Okoth, et al. [22]. However, this article had limited information on BMI. This study therefore aims to determine the association between GERD and BMI among adult patients undergoing upper GI Endoscopy at the Kenyatta National Hospital endoscopy unit.
Literature Review
Gastroesophageal reflux disease is a specific clinical entity that results from the reflux of gastric material through the lower esophageal sphincter (LES) into the esophagus or oropharynx causing symptoms and/or injury to esophageal tissue. According to the Montreal definition, GERD is a condition that develops when the reflux of stomach contents causes troublesome symptoms and/complications [23]. It is commonly characterized by substernal chest pain referred to as heartburn [24]. Although heartburn is highly specific to characterize GERD, patients usually report a number of associated symptoms such as regurgitation, nausea, sore throat, cough and globus sensation [25, 26]. GERD is often diagnosed based on typical symptoms of heartburn and regurgitation. Numerous esophageal manifestations that can occur due to esophageal mucosal injury are; reflux esophagitis, stricture, Barrett’s esophagus (BE) and esophageal adenocarcinoma [27, 28, 29]. Extra esophageal symptoms include chronic cough, asthma, laryngitis and dental erosions [30]. If left untreated, GERD can complicate into Barrett’s esophagus and esophageal adenocarcinoma [31, 32]. In BE, metaplastic columnar mucosa replaces esophageal squamous mucosa damaged by GERD [33]. GERD and BE are major risk factors for esophageal adenocarcinoma [34]. The pathophysiology of GERD is complex and multifactorial and requires a tailored individual approach. Overall, it is due to a lack of balance between the protective mechanisms and aggressive chemical substances between the valvular mechanism and the trans-diaphragmatic pressure gradient. The esophagus propels food from the mouth to the stomach with regular contractions. It runs through the chest and through the tight esophageal hiatus in the diaphragm before reaching the stomach [35]. For the system to function optimally, the lower esophagus functions as an antegrade pump, pushing food contents towards the lower esophageal sphincter which acts as the valve [36]. The stomach acts as a reservoir and in delayed gastric emptying may contribute to reflux disease. Other underlying mechanisms include poor esophageal motility and dysfunctional LES [37]. Hiatus hernia (HH), is a condition in which parts of the abdominal contents, mainly the gastroesophageal junction and the stomach, are proximally displaced above the diaphragm through the esophageal hiatus into the mediastinum [38]. The relationship between hiatal hernia and GERD has been greatly debated over the past decades. It is now understood that both the anatomical (HH) and physiologic (LES) features of the gastroesophageal junction play an important role in the pathogenesis of GERD [35, 38]. Age and obesity are major risk factors for development of hiatus hernia [39, 40, 41]. People who are overweight experience a progressive increase in intra-abdominal pressure which promotes herniation [29]. As barium swallow examinations are rarely performed nowadays and esophageal manometry is not widely available, the diagnosis of hiatus hernia usually solely relies on upper gastrointestinal endoscopy [42, 43].
Both obesity and erosive esophagitis have a high prevalence worldwide. The relationship between them remains controversial [44]. Several hypotheses have been proposed to explain how obesity can cause erosive esophagitis. Abdominal fat may cause reflux through an increase in intra-abdominal pressure and subsequent esophageal acid exposure [8, 45]. Hormonal factors related to obesity are also important mechanical factors [46, 47]. In western countries, GERD is the most common gastrointestinal disease and it is associated with a huge economic burden and decreased quality of life [48, 49, 50, 51]. Gastroesophageal reflux disease affects 10% - 38% of adults in Europe and America [1] and the global incidence of GERD is expected to increase due to demographic, dietary and epidemiologic changes [52]. In Asia, the prevalence of GERD was estimated to be lower than the western countries [53]. However, studies done in the last decade show an increase in the prevalence [54, 55]. The continent of Africa is conspicuously missing in the Global epidemiology map of GERD [2, 56]. The true incidence of GERD is largely unknown in many African populations but its prevalence is believed to be increasing due to demographic, nutritional and lifestyle transition [57]. A study by Segal, et al. 2001 [58], found a lower prevalence of GERD in Sub Saharan Africa citing possible negative correlation between H. pylori infection and GERD. In their study, H. Pylori infection, which is usually acquired in childhood and is life long, was postulated to be protective against GERD [58]. Another study in Côte d’Ivoire, looking at a young population (mean age 28 ± 9), established an incidence of heartburn, once a week in 9.2 % of the subjects under study. The incidence was higher among female patients and individuals with a family history of heartburn [59]. Another study in Nigeria found an overall prevalence of 27.1% of GERD, with no significant sex differences [60]. In Kenya, the prevalence of GERD is largely unknown. A study by Kimang’a and Revathi et al, 2010 investigating the prevalence of H. pylori, reported a 28.9 % prevalence of GERD in patients positive for H.pylori. Among these, 56-65.6% was female [61].
A diagnosis of GERD can be made based on symptoms [23]. Although GERD is a disorder of motility, the therapy of reflux diseases is aimed at reducing gastric acidity in order to decrease esophageal mucosal injury [27, 49]. Lifestyle modifications maybe effective in decreasing or eliminating GERD symptoms, but the majority of patients require pharmacologic therapy. This varies with the severity of symptoms and ranges from intermittent antacid therapy for mild disease, to histamine-2 receptor antagonists (H2RA) for moderate symptoms, to daily proton pump inhibitor (PPI) therapy for severe symptoms of GERD [62, 63, 64]. A favorable response to anti-secretory medication is used to confirm the presence of GERD [64, 65]. The main tests used when GERD is suspected are esophageal PH monitoring, endoscopy and manometry. Endoscopy is indicated in patients with heartburn and alarm symptoms (e.g., dysphagia, bleeding, anemia, weight loss and recurrent vomiting). However, it is not an appropriate first step in most patients with GERD [66]. At least 50% of patients with reflux symptoms have normal esophageal endoscopic findings (non-erosive reflux disease) or uncomplicated GERD [23, 67]. The Los Angeles classification tool is used in the categorizing of GERD based on size and number of breakages on the esophageal mucosa [68] (Table 1).
| Grade A | One (or more) mucosal break no longer than 5 mm that does not extend between the tops of two mucosal folds |
|---|---|
| Grade B | One (or more) mucosal break more than 5 mm long that does not extend between the tops of two mucosal folds |
| Grade C | One (or more) mucosal break that is continuous between the tops of two or more mucosal folds but which involve less than 75% of the circumference |
| Grade D | One (or more) mucosal break which involves at least 75% of the esophageal circumference |
Table 1: Los Angeles endoscopic classification of GERD.
Relationship between GERD and BMI
Overweight and obesity are defined as excessive fat accumulation in the body posing a risk to health. Body mass index, which is calculated as weight in kilograms divided by height in meters squared is used as a marker of obesity. A BMI value of 25–30 represents overweight and BMI >30 indicates obesity. A BMI value <25 is considered as normal [69]. Multiple studies on the association between BMI and GERD have yielded inconsistent results. There is differing data on the use of BMI as a predictor of GERD, its severity and frequency. In western countries, some studies have shown a positive correlation between high BMI and frequency of reflux [10, 17], others have demonstrated a weak association [18] and others show no association [19, 20]. There is also a gender variation as women with increased BMI were found to have a higher risk for esophagitis compared to those without [70, 71]. There was no significant difference in males [71]. In normal weight females, moderate weight gain was also associated with GERD or GERD-like symptoms [72]. Erosive esophagitis has significant correlation with increasing BMI, but the staging and classification of endoscopic erosive esophagitis is independent of the BMI of the patients [73].
Globally, the association between BMI and GERD was high in the American population [17, 74] while Europe had no association [74]. In Africa, one study done in Nigeria in 2010 showed no correlation between increased body mass index and reflux symptoms in blacks [18, 57]. Another study found a weak association between body mass index and reflux symptoms [18]. A recent study done in 2019 on the black population of South Africa showed that GERD was more common in black females than males and the prevalence rose with increasing BMI [21]. In Kenya, a focal study on the management of GERD was published by Okoth, et al. [22]. However, this article had limited information on BMI.
GERD is one of the most common gastroenterological disorders in the world and remains a frequent cause of hospital visits. Its association with BMI has been a subject of interest in its etiology and various studies done across the world have yielded discrepant results [17, 18, 19, 20, 21, 70, 71, 72, 74]. There is no data in Kenya to show an association between the two.
Methodology
Study Area
This study was conducted at the Kenyatta National Hospital endoscopy unit. This is a dedicated outpatient unit where upper and lower gastrointestinal evaluation is performed using endoscopes. Patients seen in this unit are those referred for evaluation of GI symptoms.
Study Population
The study included adult patients at the endoscopic unit presenting with the classical symptoms of GERD (heartburn and/or regurgitation) and undergoing upper endoscopy during the study period.
Inclusion Criteria: Patients ≥18years Exclusion Criteria: Patients with contraindications to upper GI endoscopy such as bleeding disorders and altered consciousness were excluded.
Study Design
This study was a cross-sectional study.
A minimum of 173 GERD patients were sampled to determine proportion with obesity/overweight within 5% level of precision.
Sampling Procedure
Consecutive sampling procedure was used to sample patients for enrollment into the study. Patients with clinical diagnosis of GERD presenting at the endoscopy unit with request for Upper GI endoscopic evaluation were approached for recruitment to the study. The researcher explained to the subjects the objectives of the study and those who consented to participate were recruited.
Data Collection Materials and Techniques
Administering the Questionnaires: The validated GERD questionnaire tools were administered by trained research assistants to reduce inter-observer variability. The questionnaire had a section on demographic data such as age, gender, height and weight as well as a section assessing for GERD symptoms. The section assessing for GERD symptoms included a Likert scale for severity and frequency of symptoms (Appendix III). The weight (measured in kgs) and height (Meters) were taken using a standardized medical weighing scale. BMI was calculated as follows:
(Kgs) 2 ( ) weight height m The subjects were then be categorized into Normal (<25), overweight (25-29.9), Obese (> 30) based on their BMI findings. In this study, classical GERD symptoms were defined as the presence of either heartburn or acid regurgitation. Heartburn was defined as “a burning pain or discomfort behind the breast bone in the chest” and acid regurgitation as “a bitter or sour-tasting fluid coming into the throat or mouth,” definitions that have been validated previously [72]. The survey was conducted over a period of 3 months to give time for collection of required sample size.
Upper GI Endoscopy
- Purpose: To look at esophageal mucosal changes.
- Preparation & consent: The procedure was performed under local anesthetic. The back of the subject’s throat was sprayed with the anesthetic. Light sedation was administered as needed. As the scope was passed down towards the stomach, the presence of GERD was assessed based on the presence, size and number of mucosal breakages at the gastroesophageal junction as per the Los Angeles classification [68]. Presence or absence of hiatus hernia was determined by assessing the gastroesophageal flap valve using the Hill Classification [77]. The findings were recorded in a data sheet for each patient (Appendix IV). When the procedure was completed, the subject was taken to the recovery ward where the blood pressure, heart rate and oxygen levels were monitored until they were fully awake.
Data Management
Data was coded and cleaned in SPSS version 25. The data was then be summarized by calculating frequencies, means and proportions. The period prevalence of patients with GERD was calculated using the formula below:
& Numberof patients presenting with classicalGERDbetween Julyand October pp Total numberof patientsattheMOPC and EndoscopicUnitbetween July Oct = Associations between respondent demographic data (age, BMI from height and weight) and GERD was assessed by Student t test or Mann–Whitney U test for continuous variables. Chi-square analysis was applied for categorical variables (gender). A P-value of <0.05 was considered significant.
Results
This was an analysis of 174 patients who underwent endoscopy in the unit. As shown in Table 2, the mean age was 43± 14.1 years and majority (56.9%) was female. The patients had a mean weight of 71.2±10.8 Kg and mean height of 1.6± 0.1 meters.
| Variable | Frequency (%) |
|---|---|
| Age in years | |
| Mean (SD) | 43.0 (14.1) |
| Min – max | 18.0-80.0 |
| Gender | |
| Male | 75 (43.1) |
| Female | 99 (56.9) |
| Weight | |
| Mean (SD) | 71.2 (10.8) |
| Min – Max | 42.0-100.5 |
| Height | |
| Mean (SD) | 1.6 (0.1) |
| Min – Max | 1.4-1.9 |
Table 3: Characteristics of the 174 study participants.
Overweight and Obesity: As shown in Table 3, the mean BMI was 26.6 Kg/m2 ranging from 14.5 to 38.6 Kg/m2. The proportion of patients who were overweight was 40.2% and obese patients made up 21.8% of the population.
| Variable | Frequency (%) | 95% CI |
|---|---|---|
| BMI | ||
| Mean (SD) | 26.6 (3.9) | 26.0-27.1 |
| Min – Max Category, n (%) | 14.5-38.6 | - |
| Normal (<25) | 66 (37.9) | 31.0-44.8 |
| Overweight (25-29.9) | 70 (40.2) | 33.3-47.7 |
| Obese (≥30) | 38 (21.8) | 16.1-27.6 |
Table 2: Overweight and obesity in patients presenting with GERD.
When a Chi- Square was performed to determine the differences in the BMI by gender, it was found that males and females did not differ significantly as shown in Table 4 below.
| Variable | Female | Male | P-value |
|---|---|---|---|
| BMI | |||
| Normal | 37(37.4) | 29(38.7) | 0.663 |
| Overweight | 38(38.4) | 32(42.7) | |
| Obese | 24(24.2) | 14(18.7) | |
| BMI | |||
| Normal | 37(37.4) | 29(38.7) | 0.862 |
| Overweight | 62(62.6) | 46(61.3) |
Table 4: Comparison between males and females by BMI.
Frequency of GERD Symptoms and its Association with BMI: The mean score of the scale of GERD symptoms in the sample was 18 with 60.3% of the patients having scores of 10 to 19. As shown in Table 5, when BMI was categorized as normal and overweight/obese there was no association with the scale of GERD symptoms.
| Variable | Frequency (%) | BMI | P value | |
|---|---|---|---|---|
| Overweight/ Obese | Normal | |||
| FSSG | ||||
| Mean (SD) Category, n (%) | 18.0 (5.0) | 18.3 (5.0) | 17.4 (5.0) | 0.217 |
| <10 | 5 (2.9) | 3 (2.8) | 2 (3.0) | 0.759 |
| 19-Oct | 105 (60.3) | 63 (58.3) | 42 (63.9) | |
| 20+ | 64 (36.8) | 42 (38.9) | 22 (33.3) |
Table 5: Frequency of GERD symptoms by BMI status.
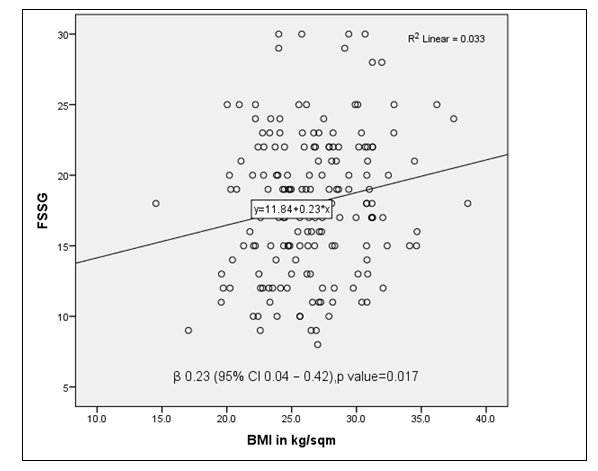
However, as illustrated in Figure 1, there was a positive relationship between BMI measurements and frequency scale of GERD symptoms. Increasing BMI was significantly correlated to higher frequency scale of symptoms, β 0.23 (95% CI 0.04-0.42), p=0.017.
Endoscopic findings among GERD Patients: As shown in Table 6, 35.6% of the patients had esophagitis and 28.7% were LA-A and 6.9% LA-B. Hiatal hernia was diagnosed in 20.7% of the patients. There was no significant association between diagnoses of esophagitis and hiatal hernia with BMI status of the patients (Table 6).
| Variable | Frequency (%) |
|---|---|
| Esophagitis | |
| Absent | 112 (64.4) |
| LA-A | 50 (28.7) |
| LA-B | 12 (6.9) |
| Hiatal hernia | |
| Absent | 138 (79.3) |
| Hills-I | 14 (8.0) |
| Hills-II | 14 (8.0) |
| Hills-III | 8 (4.6) |
Table 7: Endoscopic findings of the 174 study participants.
When we explored the association between endoscopic findings and BMI, there was no association as shown in the Table 7 below.
| Variable | Overweight/obese | Normal | P value |
|---|---|---|---|
| Esophagitis | |||
| Present | 38 (35.2) | 24 (36.4) | 0.875 |
| Absent | 70 (64.8) | 42 (63.6) | |
| Hiatal hernia | |||
| Present | 22 (20.4) | 14 (21.2) | 0.894 |
| Absent | 86 (79.6) | 52 (78.8) |
Table 6: Association between endoscopic findings and BMI.
Similarly, when we tested for the association between BMI and endoscopic findings, it was found that obesity and overweight were not associated with esophagitis and hiatal hernia.
The details are shown in Table 8 below.
| Variable | Normal | Obese | P value1 | Overweight | P value2 |
|---|---|---|---|---|---|
| Esophagitis | |||||
| Present | 24 (36.4) | 19 (50.0) | 0.174 | 19 (27.1) | 0.248 |
| Absent | 42 (63.6) | 19 (50.0) | 51 (72.9) | ||
| Hiatal hernia | |||||
| Present | 14 (21.2) | 7 (18.4) | 0.733 | 15 (21.4) | 0.975 |
| Absent | 52 (78.8) | 31 (81.6) | 55 (78.6) |
Table 8: Association between BMI and endoscopic findings.
Discussion
GERD is a common clinical problem worldwide and obesity is known to be one of the factors associated with GERD. It has been studied that increasing BMI increases the risk of developing GERD [2, 7] and that overweight and obesity contribute to its complications including esophagitis and esophageal adenocarcinoma [78]. Obese patients may experience extrinsic gastric compression by surrounding adipose tissue leading to an increase in intragastric pressure and subsequent relaxation of the LES [79, 80, 81] this study was undertaken with an aim to determine the association, if any between increasing BMI and severity of GERD symptoms and document the endoscopic findings in GERD patients with increasing BMI. In this study, more than 60% of the patients were overweight or obese. The proportion of patients who were overweight was 40.2% and obese patients made 21.8% of the population. There were more overweight and obese female patients (57.4%) than males (42.6%) although the differences were not statistically significant. However, these findings are indicative of the trends in previous studies. A study on prevalence and factors associated with overweight and obesity in Kenya showed that the likelihood of having overweight and obesity was increased among women, urban residents and individuals with higher education [82].
The mean frequency scale of GERD symptoms in the study population was 18. The overweight and obese had a mean frequency of 18.3 compared to 17.4 in the normal (Table 3). There was no significant difference between obese patients and those with normal weight in relation to the number of GERD symptoms. Similar results were seen when patients with normal weight were compared to the overweight category. However, there was a positive correlation between increasing BMI and frequency of symptoms (Figure 1). A 10 unit increase in BMI increased frequency of symptoms by a scale of 2 (β 0.23). Studies on the same have shown that the majority of GERD symptoms have likelihood of occurring with increasing BMI [76] and successful weight loss is associated with fewer GERD symptoms [3]. Many factors may contribute to the development of GERD. Among them, there are non- modifiable factors such as age, gender or genetic factors. It has been shown that the risk of GERD symptoms in the adult population increases with age [56, 83]. However, this study showed no age association with severity of symptoms (Table 4). This finding is in keeping with a previous study done on the influence of age on GERD in symptomatic patients [84]. In this study, the gender of the patients was not associated with severity of symptoms. This is in contrast to the West where several studies have shown that women are more likely to develop GERD symptoms [84, 85, 86, 87, 88]. However, some studies have shown that the disease occurs with similar frequency in men and women [89].
In this study, erosive esophagitis was absent in 64.4% of the population. About a third of the patients had esophagitis (35.6%). Of these, 28.7% were LA- A and 6.9% LA- B. Studies done have shown that at least 50% of patients with reflux symptoms have normal esophageal endoscopic findings (non-erosive reflux disease) [23, 67]. Many studies have also shown that reflux esophagitis is more common in men [90, 91, 92, 93]. Hiatal hernia was diagnosed in 20.6% of the patients. The presence of esophagitis was not significantly associated with age and gender. However, patients with hiatal hernia were significantly older (mean 49.3 years) compared to those without hernia (mean 41.3 years), p=0.002. Our study was not without limitations. The major limitation is that it was hospital based. This has the potential to cause underestimation of the prevalence because it focused on the patients who presented to hospital. In the same vein, our findings are valid to the study population but cannot be extrapolated to the entire population because the study participants were conveniently recruited. Therefore, our study findings should be interpreted in this context.
Conclusions
- The prevalence of overweight patients with GERD is high in the study population
- The prevalence of obesity in the study population was fairly low
- Increasing BMI influences the severity of GERD symptoms in the study population.
- Increasing BMI does not predict the presence of Hiatal hernia and esophagitis in the study population.
References
-
Clarrett DM, Hachem C (2018) Gastroesophageal Reflux Disease (GERD). Mo Med 115(3): 214-218.
-
Serag HBE, Sweet S, Winchester CC, Dent J (2014) Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 63(6): 871-880.
-
Chang P, Friedenberg F (2014) Obesity and GERD. Gastroenterol Clin North Am 43(1): 161-173.
-
Lee KJ (2011) Nocturnal gastroesophageal reflux: assessment and clinical implications. J Neurogastroenterol Motil 17(2): 105-107.
-
Nocon M, Labenz J, Willich SN (2006) Lifestyle factors and symptoms of gastro-oesophageal reflux -- a population- based study. Aliment Pharmacol Ther 23(1): 169-174.
-
Serag HBE, Graham DY, Satia JA, Rabeneck L (2005) Obesity is an independent risk factor for GERD symptoms and erosive esophagitis. Am J Gastroenterol 100(6): 1243-1250.
-
Kumar A, Kazi A, Riaz SU, Kumar R, Kumar N, et al. (2017) Obesity-An Impactful Risk Factor for Gastro- Oesophageal Reflux Disease. ASH & KMDC 22(3): 214- 218.
-
Serag HBE, Ergun GA, Pandolfino J, Fitzgerald S, Tran T, et al. (2007) Obesity increases oesophageal acid exposure. Gut 56(6): 749-755.
-
Herbella FA, Patti MG (2010) Gastroesophageal reflux disease: From pathophysiology to treatment. World J Gastroenterol 16(30): 3745-3749.
-
Murray L, Johnston B, Lane A, Harvey I, Donovan J, et al. (2003) Relationship between body mass and gastro- oesophageal reflux symptoms: The Bristol Helicobacter Project. Int J Epidemiol 32(4): 645-650.
-
Nadaleto BF, Herbella FA, Patti MG (2016) Gastroesophageal reflux disease in the obese: Pathophysiology and treatment. Surgery 159(2): 475- 486.
-
Patti MG, Schlottmann F (2019) Correction to: Gastroesophageal reflux disease: from heartburn to Barrett esophagus, and beyond. Updates Surg 71(1): 189.
-
Engin A (2017) The Definition and Prevalence of Obesity and Metabolic Syndrome. Adv Exp Med Biol 960: 1-17.
-
Friedrich MJ (2017) Global Obesity Epidemic Worsening. JAMA 318(7): 603.
-
Mbochi RW, Kuria E, Kimiywe J, Ochola S, Steyn NP (2012) Predictors of overweight and obesity in adult women in Nairobi Province, Kenya. BMC Public Health 12: 823.
-
Peters R, Amugsi DA, Mberu B, Ensor T, Hill AJ, et al. (2019) Nutrition transition, overweight and obesity among rural-to-urban migrant women in Kenya. Public Health Nutr 22(17): 3200-3210.
-
Icitovic N, Onyebeke LC, Wallenstein S, Dasaro CR, Harrison D, et al. (2016) The association between body mass index and gastroesophageal reflux disease in the World Trade Center Health Program General Responder Cohort. Am J Ind Med 59(9): 761-766.
-
Akere A, Afolabi BA, Adebusoye LA (2010) Association between body mass index and gastroesophageal reflux disease in blacks. Niger J Gastroenterol Hepatol 2(2): 89- 94.
-
Kasyap AK, Sah SK, Chaudhary S, Shrestha R, Shrestha D (2015) Association between Body Mass Index and Gastroesophageal Reflux Symptoms in Nepalese Adult Population. A Single Centered Hospital Based Study. JCMS Nepal 11(2): 23-26.
-
Lagergren J, Bergström R, Nyrén O (2000) No relation between body mass and gastro-oesophageal reflux symptoms in a Swedish population based study. Gut 47(1): 26-29.
-
Hunter MP, Crowther NJ (2019) The prevalence of gastroesophageal reflux disease in an adult, South African black population, and the association with obesity. Minerva Gastroenterol Dietol 65(2): 100-106.
-
Okoth FA, Lule GN, Ogutu EO, Pilczer S, Dubois C (1994) Famotidine in the management of gastro-oesophageal reflux. East Afr Med J 71(1): 44-48.
-
Vakil N, Zanten SVV, Kahrilas P, Dent J, Jones R, (2006) The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 101(8): 1900-1920.
-
Smith H (2016) Heartburn, gastro-oesophageal reflux disease and non-erosive reflux disease. S Afr Fam Pract 58(5): 44-48.
-
Varannes SBD, Cestari R, Usova L, Triantafyllou K, Sanchez AA, et al. (2014) Classification of adults suffering from typical gastroesophageal reflux disease symptoms: contribution of latent class analysis in a European observational study. BMC Gastroenterol 14: 112.
-
Klauser AG, Schindlbeck NE, Lissner SAM (1990) Symptoms in gastro-oesophageal reflux disease. Lancet 335(8683): 205-208.
-
Kahrilas PJ (2003) GERD pathogenesis, pathophysiology, and clinical manifestations. Cleve Clin J Med 70 (5): S4- S19.
-
Menezes MA, Herbella FAM (2017) Pathophysiology of Gastroesophageal Reflux Disease. World J Surg 41(7): 1666-1671.
-
Pandolfino JE, Serag HBE, Zhang Q, Shah N, Ghosh SK, et al. (2006) Obesity: a challenge to esophagogastric junction integrity. Gastroenterology 130(3): 639-649.
-
Hom C, Vaezi MF (2013) Extra-esophageal manifestations of gastroesophageal reflux disease: diagnosis and treatment. Drugs 73(12): 1281-1295.
-
Coleman HG, Xie SH, Lagergren J (2018) The Epidemiology of Esophageal Adenocarcinoma. Gastroenterology 154(2): 390-405.
-
Westerhof GA, Coumou H, Nijs SBD, Weersink EJ, Bel EH (2018) Clinical predictors of remission and persistence of adult-onset asthma. J Allergy Clin Immunol 141(1): 104-109.
-
Spechler SJ, Souza RF (2014) Barrett’s esophagus. N Engl J Med 371(9): 836-845.
-
Spechler SJ (2013) Barrett esophagus and risk of esophageal cancer: a clinical review. JAMA 310(6): 627- 636.
-
Roman S, Kahrilas PJ (2014) The diagnosis and management of hiatus hernia. BMJ 349: g6154.
-
Singhal V, Khaitan L (2014) Gastroesophageal reflux disease: diagnosis and patient selection. Indian J Surg 76(6): 453-460.
-
Martinucci I, Bortoli ND, Giacchino M, Bodini G, Marabotto E, et al. (2014) Esophageal motility abnormalities in gastroesophageal reflux disease. World J Gastrointest Pharmacol Ther 5(2): 86-96.
-
Hyun JJ, Bak YT (2011) Clinical significance of hiatal hernia. Gut Liver 5(3): 267-277.
-
Berstad A, Weberg R, Larsen IF, Hoel B, Jensen MH (1986) Relationship of hiatus hernia to reflux oesophagitis. A prospective study of coincidence, using endoscopy. Scand J Gastroenterol 21(1): 55-58.
-
Larsen GS, Weberg R, Larsen IF, Bjortuft O, Hoel B, et al. (1988) Relationship of overweight to hiatus hernia and reflux oesophagitis. Scand J Gastroenterol 23(4): 427- 432.
-
Wilson LJ, Ma W, Hirschowitz BI (1999) Association of obesity with hiatal hernia and esophagitis. Am J Gastroenterol 94(10): 2840-2844.
-
Dimou FM, Gonzalez C, Velanovich V (2018) Utility of Endoscopy in the Diagnosis of Hiatus Hernia and Correlation with GERD. In: Memon MA (Ed.), Hiatal Hernia Surgery: An Evidence Based Approach Cham. Springer International Publishing, pp: 1-16.
-
Weyenberg SJBV (2013) Diagnosis and Grading of Sliding Hiatal Hernia. Video Journal and Encyclopedia of GI Endoscopy 1(1): 117-119.
-
Cai N, Ji GZ, Fan ZN, Wu YF, Zhang FM, et al. (2012) Association between body mass index and erosive esophagitis: a meta-analysis. World J Gastroenterol 18(20): 2545-2553.
-
Serag HBE, Tran T, Richardson P, Ergun G (2006) Anthropometric correlates of intragastric pressure. Scand J Gastroenterol 41(8): 887-891.
-
Wu JCY, Mui LM, Cheung CMY, Chan Y, Sung JJY (2007) Obesity is associated with increased transient lower esophageal sphincter relaxation. Gastroenterology 132(3): 883-889.
-
Wu YW, Tseng PH, Lee YC, Wang SY, Chiu HM, et al. (2014) Association of esophageal inflammation, obesity and gastroesophageal reflux disease: from FDG PET/CT perspective. PLoS One 9(3): e92001.
-
Dika SE, Guyatt GH, Armstrong D, Degl’innocenti A, Wiklund I, et al. (2005) The impact of illness in patients with moderate to severe gastro-esophageal reflux disease. BMC Gastroenterol 5: 23.
-
Kahrilas PJ (2008) Clinical practice. Gastroesophageal reflux disease. N Engl J Med 359(16): 1700-1707.
-
Shaheen NJ, Hansen RA, Morgan DR, Gangarosa LM, Ringel Y, et al. (2006) The burden of gastrointestinal and liver diseases, 2006. Am J Gastroenterol 101(9): 2128- 2138.
-
Wahlqvist P, Reilly MC, Barkun A (2006) Systematic review: the impact of gastro-oesophageal reflux disease on work productivity. Aliment Pharmacol Ther 24(2): 259-272.
-
Shaw MJ, Talley NJ, Beebe TJ, Rockwood T, Carlsson R, et al. (2001) Initial validation of a diagnostic questionnaire for gastroesophageal reflux disease. Am J Gastroenterol 96(1): 52-57.
-
Sharma P, Wani S, Romero Y, Johnson D, Hamilton F (2008) Racial and geographic issues in gastroesophageal reflux disease. Am J Gastroenterol 103(11): 2669-2680.
-
Bhatia SJ, Reddy DN, Ghoshal UC, Jayanthi V, Abraham P, et al. (2011) Epidemiology and symptom profile of gastroesophageal reflux in the Indian population: report of the Indian Society of Gastroenterology Task Force. Indian J Gastroenterol 30(3): 118-127.
-
Fock KM, Talley N, Goh KL, Sugano K, Katelaris P, et al. (2016) Asia-Pacific consensus on the management of gastro-oesophageal reflux disease: an update focusing on refractory reflux disease and Barrett’s oesophagus. Gut 65(9): 1402-1415.
-
Eusebi LH, Ratnakumaran R, Yuan Y, Dodaran MS, Bazzoli F, et al. (2018) Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut 67(3): 430-440.
-
Nwokediuko SC, Adekanle O, Akere A, Olokoba A, Anyanechi C, et al. (2020) Gastroesophageal reflux disease in a typical African population: a symptom- based multicenter study. BMC Gastroenterol 20(1): 107.
-
Segal I (2001) The gastro-oesophageal reflux disease complex in sub-Saharan Africa. Eur J Cancer Prev 10(3): 209-212.
-
Assi C, Kone S, Ndjitoyap AWN, Ouattara A, Ananissoh LML, et al. (2014) Prevalence of heartburn in Abidjan, a black African Country, and associated factors. OJG 4(4): 175-180.
-
Ajayi AO, Solomon OA, Adegun PT (2013) Prevalence of GERD in Ado-Ekiti, Nigeria. Niger J Gastroenterol Hepatol 5(2): 79-84.
-
Kimang’a AN, Revathi G, Kariuki S, Sayed S, Devani S (2010) Helicobacter pylori: prevalence and antibiotic susceptibility among Kenyans. S Afr Med J 100(1): 53-57.
-
Katz PO (2003) Optimizing medical therapy for gastroesophageal reflux disease: state of the art. Rev Gastroenterol Disord 3(2): 59-69.
-
Katz PO (2007) Medical therapy for gastroesophageal reflux disease in 2007. Rev Gastroenterol Disord 7(4): 193-203.
-
Katz PO, Gerson LB, Vela MF (2013) Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 108(3): 308-328.
-
Numans ME (2006) The use of proton pump inhibitors as a diagnostic test for gastroesophageal reflux disease. Arch Intern Med 166(2): 247-248.
-
Shaheen NJ, Weinberg DS, Denberg TD, Chou R, Qaseem A, et al. (2012) Upper endoscopy for gastroesophageal reflux disease: best practice advice from the clinical guidelines committee of the American College of Physicians. Ann Intern Med 157(11): 808-816.
-
Ronkainen J, Aro P, Storskrubb T, Johansson SE, Lind T, et al. (2005) High prevalence of gastroesophageal reflux symptoms and esophagitis with or without symptoms in the general adult Swedish population: a Kalixanda study report. Scand J Gastroenterol 40(3): 275-285.
-
Sami SS, Ragunath K (2013) The Los Angeles Classification of Gastroesophageal Reflux Disease. Video Journal and Encyclopedia of GI Endoscopy 1(1): 103- 104.
-
World Health Orgnization (2020) Obesity and overweight.
-
Bouchoucha M, Fysekidis M, Julia C, Airinei G, Catheline JM, et al. (2016) Body mass index association with functional gastrointestinal disorders: differences between genders. Results from a study in a tertiary center. J Gastroenterol 51(4): 337-345.
-
Nocon M, Labenz J, Jaspersen D, Sabellek WM, Stolte M, et al. (2007) Association of body mass index with heartburn, regurgitation and esophagitis: results of the Progression of Gastroesophageal Reflux Disease study. J Gastroenterol Hepatol 22(11): 1728-1731.
-
Jacobson BC, Somers SC, Fuchs CS, Kelly CP, Camargo CA (2006) Body-mass index and symptoms of gastroesophageal reflux in women. N Engl J Med 354(22): 2340-2348.
-
Vaishnav B, Bamanikar A, Maske P, Reddy A, Dasgupta S (2017) Gastroesophageal Reflux Disease and its Association with Body Mass Index: Clinical and Endoscopic Study. J Clin Diagn Res 11(4): OC01-OC04.
-
Corley DA, Kubo A (2006) Body mass index and gastroesophageal reflux disease: a systematic review and meta-analysis. Am J Gastroenterol 101(11): 2619- 2628.
-
Department KNHDR (2020).
-
Zafar S, Haque IU, Tayyab GUN, Rehman AU, Rehman AU, et al. (2008) Correlation of gastroesophageal reflux disease symptoms with body mass index. Saudi J Gastroenterol 14(2): 53-57.
-
Hansdotter I, Bjor O, Andreasson A, Agreus L, Hellstrom P, et al. (2016) Hill classification is superior to the axial length of a hiatal hernia for assessment of the mechanical anti-reflux barrier at the gastroesophageal junction. Endosc Int Open 4(3): E311-E317.
-
Hampel H, Abraham NS, Serag HBE (2005) Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med 143(3): 199-211.
-
Mercer CD, Wren SF, DaCosta LR, Beck IT (1987) Lower esophageal sphincter pressure and gastroesophageal pressure gradients in excessively obese patients. J Med 18(3-4): 135-146.
-
Mercer CD, Rue C, Hanelin L, Hill LD (1985) Effect of obesity on esophageal transit. Am J Surg 149(1): 177- 181.
-
Zacchi P, Mearin F, Humbert P, Formiguera X, Malagelada JR (1991) Effect of obesity on gastroesophageal resistance to flow in man. Dig Dis Sci 36(10): 1473-1480.
-
Mkuu R, Barry A, Yonga G, Nafukho F, Wernz C, et al. (2021) Prevalence and factors associated with overweight and obesity in Kenya. Prev Med Rep 22: 101340.
-
Taraszewska A (2021) Risk factors for gastroesophageal reflux disease symptoms related to lifestyle and diet. Rocz Panstw Zakl Hig 72(1): 21-28.
-
Ter RB, Johnston BT, Castell DO (1998) Influence of age and gender on gastroesophageal reflux in symptomatic patients. Dis Esophagus 11(2): 106-108.
-
Dore MP, Maragkoudakis E, Fraley K, Pedroni A, Tadeu V, et al. (2008) Diet, lifestyle and gender in gastro- esophageal reflux disease. Dig Dis Sci 53(8): 2027-2032.
-
Serag HBE, Satia JA, Rabeneck L (2005) Dietary intake and the risk of gastro-oesophageal reflux disease: a cross sectional study in volunteers. Gut 54(1): 11-17.
-
Hallan A, Bomme M, Hveem K, Hansen JM, Jensen EN (2015) Risk factors on the development of new-onset gastroesophageal reflux symptoms. A population- based prospective cohort study: the HUNT study. Am J Gastroenterol 110(3): 393-400.
-
Nirwan JS, Hasan SS, Babar ZUD, Conway BR, Ghori MU (2020) Global Prevalence and Risk Factors of Gastro- oesophageal Reflux Disease (GORD): Systematic Review with Meta-analysis. Sci Rep 10(1): 5814.
-
Moayyedi P, Talley NJ (2006) Gastro-oesophageal reflux disease. Lancet 367(9528): 2086-2100.
-
Chih PC, Yang YC, Wu JS, Chang YF, Lu FH, et al. (2013) Overweight associated with increased risk of erosive esophagitis in a non-obese Taiwanese population. PLoS One 8(11): e77932.
-
Crews NR, Johnson ML, Schleck CD, Enders FT, Wongkeesong LM, et al. (2016) Prevalence and Predictors of Gastroesophageal Reflux Complications in Community Subjects. Dig Dis Sci 61(11): 3221-3228.
-
Jonaitis L, Kriukas D, Kiudelis G, Kupcinskas L (2011) Risk factors for erosive esophagitis and Barrett’s esophagus in a high Helicobacter pylori prevalence area. Medicina (Kaunas) 47(8): 434-439.
-
Nozu T, Komiyama H (2008) Clinical characteristics of asymptomatic esophagitis. J Gastroenterol 43(1): 27-31.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient