Rectal Carcinoma
Rectum is the distal part of the large intestine, placed between the sigmoid colon and large gut. It serves as a temporary reservoir for fecal contents. Rectal carcinoma is the second most common cancer of large intestine accounting for 28% of the cases. Large numbers of cases are asymptomatic in early stages. Extension of rectal tumors into adjacent organs or into the lumen of GI tract leads to symptomatic presentation. In regard to the improved access to and use of screening and standard treatment, overall incidence rate has decreased by approximate 3% per year during the past decade. The location and adjacent structure to the rectum makes the treatment of rectal carcinoma different to that of tumors located in other part of GI Tract. In this article, the anatomy and physiology of rectum, risk factors, pathogenesis, clinical types, clinical features, screening, diagnosis, spread, staging and treatment of rectal carcinoma are reviewed along with the prognosis.
Introduction
Rectal carcinoma is the third most common cancer in men and second in women. It is the second most common cancer of large intestine accounting for 28% after proximal colon cancer (42%). The accumulation of genetic mutation, either somatic (acquired) and/or germ line (inherited), results transformation of normal rectal or colonic epithelium to pre-cancerous lesions; adenomas and ultimately to invasive carcinoma. Once the diagnosis of rectal cancer is established, the local and distant extent of tumor should be determined for further therapeutic approach. Surgery is the mainstay of treatment. Adjuvant chemotherapy and radiotherapy is a must.
Methodology
Text books, various published articles, authentic website data, etc. on ‘Rectal carcinoma’, ‘Staging’, ‘Prognosis’ were studied and used as materials to highlight the subject.
Results
Anatomy of Rectum
Rectum is the distal part of the large intestine placed between the sigmoid colon and large gut. The three cardinal features of large intestine- sacculation, appendices epiploicae and taenia are absent in the rectum. It is 12 cm long with the diameter of 4cm starting as the continuation of sigmoid colon (S3) till the anal canal, 2 to 3 cm in front and below the tip of coccyx. It has got 3 lateral flexions left, right and left from below upwards. It is related anteriorly to rectovesical pouch (upper tow-third) and base of urinary bladder, terminal part of ureter, seminal vesicle, deferent duct, and prostate in males, and lower part of vagina in females [1]. Posteriorly, three pieces of sacrum, coccyx, ano- coccygeus ligament, sympathetic chains, and superior rectal and median sacral artery are present. It has been pulled anteriorly by puborectalis muscle forming the anorectic sling which is primarily responsible for the rectal continence. Rectum has been supported by pelvic floor inferiorly, fascia of Waldeyer posteriorly, lateral ligaments of rectum on posterior-lateral aspect and Dononvillier’s fascia anteriorly separating from prostate in male and vagina in female. Rectal wall compromises 5 layers including mucosa, sub mucosa, inner circular muscle, outer longitudinal muscle and serosa. At the junction of proximal 2/3rd and distal 1/3rd, rectum separates into intra and extra-peritoneal portion by anterior peritoneal reflection. Proximal 2/3rd is covered by peritoneum and distal portion lacks serosa. 3 mucosal folds called the Valves of Houston extend into the rectal lumen. Recto-sigmoid junction implies segment of bowel compromising last 7cm of sigmoid colon and upper 5cm of rectum. At the end of rectum is a section called rectal ampulla which connects to the anal canal. Rectum is supplied and drained by vessels originating from superior, middle and inferior rectal vessels. Lymphatic drainage from upper half of rectum is to inferior mesenteric nodes and from lower half to internal iliac nodes.
Physiology of Rectum
Rectum serves as a temporary reservoir for fecal contents, before it releases via anal canal. When the rectal ampulla becomes full, the intra-rectal pressure causes the anal canal walls to dilate and expand, allowing faeces to enter the anal canal. Rectum has been innervated by the autonomic nervous system, sympathetic (L1,L2) is motor to sphincter and inhibitory to musculature, parasympathetic (S2,S3,S4) is motor to musculature and inhibitor to sphincter.
Carcinoma Rectum
Epidemiology: Rectal carcinoma is the third most common cancer in men and second in women. It is the second most common cancer of large intestine accounting for 28% after proximal colon cancer (42%) [2]. Colorectal cancer is more common in developed region, but their mortality seems to be more in less developed regions of the world. It is the third most leading cause of cancer deaths in USA. Globocan 2012 has estimated the cancer incidence in lifetime with the probability of 4.7-5% [3]. In regard to the improved access to and use of screening and standard treatment, overall incidence rate has decreased by approximate 3% per year during the past decade.
Risk Factors
Age: The risk of Rectal Ca increases after 50 years of age.
Gender: Female are at higher risk as compared to male.
BMI: Every 5 kg/m2 increase in BMI is associated with a 24% and 9% increased incidence of colorectal carcinomas in men and women, respectively [4].
Diet: Low fiber diet, high fat diet, red meat, processed meat and burnt or charred meat increase the risk of rectal carcinoma [5]. Cholesterol increases the bile acid concentration in intestinal lumen which acts as carcinogen. Patient with rectal cancer tended to have slightly higher folate and slightly lower calcium intake. Decreased Magnesium intake increases the risk of rectal Ca. higher intake of milk and dairy products are associated with significant reduction in risk of colon cancer but not affecting the risk of rectal cancer.
Habit: Tobacco consumption, smoking, heavy alcohol intake and sedentary lifestyle increase the risk.
Diseases: Ulcerative Colitis, Crohn’s disease, long standing inflammatory bowel disease and hereditary diseases like Familial adenomatous polyposis (FAP), hereditary non- polyposis colorectal carcinoma (HNPCC). MUTYH associated polyposis (MAP) are high risk factors. Risk of rectal cancer is 20% higher among the patients with Diabetes Mellitus and insulin resistance than non-diabetic patients. Personal history of Colorectal Carcinoma or adenomatous polyp promotes the risk for Rectal Ca. History of radiation therapy for prostate cancer is the risk factor of rectal cancer.
Genetic: Any 1st degree relative of a person with rectal carcinoma will show two times increased risk of Ca rectum.
Pathogenesis
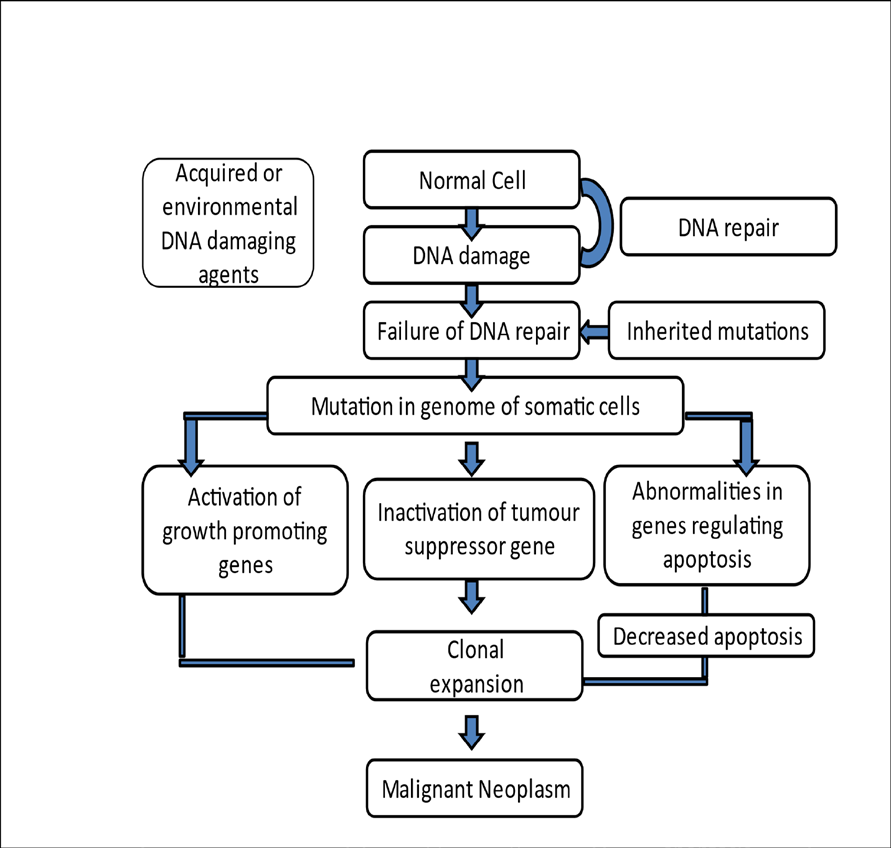
The accumulation of genetic mutation, either somatic (acquired) and / or germ line (inherited), results transformation of normal rectal or colonic epithelium to pre-cancerous lesions; adenomas and ultimately to invasive carcinoma. The mutation of these cells causes clonal expansion resulting in the self-sufficiency in growth signals, insensitivity to growth inhibitory signals, altered cell metabolism, evasion of apoptosis, limitless replicating potential, sustained angiogenesis, ability to invade and metastasize and ability to evade host immune response, grossly viewed as the cancer hallmarks. Clinical evidence has shown that the colorectal cancer frequently arises from adenomatous polyps that typically acquire dysplastic changes over ten to fifteen years, leading to invasive carcinoma development. Thus, early detection and removal of polyp reduces the incidence of colorectal carcinoma (Figure 1).
Classifications
Pathological Types
- Annular Variety: This is common at the recto-sigmoid junction. It presents with constipation and Intestinal Obstruction [6]. It takes about a year for the growth to completely encircle the lumen of the gut (napkin ring deformity).
- Polypoidal Variety: This is common in ampulla of the rectum.
- Ulcerative Variety: This can occur anywhere in the rectum with raised edges and the growth occurs in transverse direction.
- Diffuse Variety: This is similar to linitis plastica (of carcinoma of stomach). It develops from UC. It has a poor prognosis.
- Colloid Variety: This is rare. The tumor contents are gelatinous due to increased mucus production. This variety is seen in young patients. The cell is filled with mucus and nucleus is displaced. It is called ‘Signet Ring’ carcinoma. It is also associated with poor prognosis.
Histological Types
Adenocarcinoma which may be Well-differentiated (11%) Good prognosis Moderately Differentiated (65%) Poor prognosis Undifferentiated (25%) Bad prognosis
Clinical Features
Symptoms
- Large numbers of cases are asymptomatic in early stages. Extension of rectal tumors into adjacent organs or into the lumen of GI tract leads to symptomatic presentation.
- Bleeding per anum is the earliest symptom. It usually occurs at the end of defecation in slight amount, or it is noticed by the stained underclothings. Hemorrhoids and carcinoma sometimes co-exist further misleading the diagnosis.
- Sense of incomplete evacuation- The patient’s bowels open, but there is the remaining sensation that there are more faeces to be passed (tenesmus, a distressing straining during defecation to empty the bowels without resultant evacuation.). This is almost invariably present in tumors involving lower half of rectum. The patient may endeavor to empty the rectum several times a day (spurious diarrhea), often with the passage of flatus and little blood-stained mucus; bloody slime.
- Altered bowel habit is the next most frequent symptom. The patient sometimes finds it necessary to start the intake of aperient or to supplement the usual dose. A patient who has to get up early in order to defecate, or one who passes blood and mucus in addition to the faeces (early morning bloody diarrhea), is usually found to have rectal carcinoma. Often, it is patient with an annular carcinoma at the recto sigmoid junction who suffers with increasing constipation, and the one with a growth in ampulla of the rectum who has early- morning diarrhea.
- Spurious diarrhea- Over accumulation of mucus overnight in the rectum creates urgency for defecation in the early morning. But it results in spurious diarrhea with incomplete painful defecation.
- Tenesmus
- Pain is late symptom, but pain of a colicky nature may be present in advanced tumors of recto sigmoid, and is caused by some degree of IO. When a deep carcinomatous ulcer of rectum erodes the prostate or the bladder, there may be severe pain. Pain in the back, or sciatica, occurs when the cancer invades the sacral plexus.
- Loss of appetite and weight, malnutrition. Weight loss is suggestive of the hepatic metastases.
- May present emergently with obstructive symptoms (IO), acute GI bleed or peritonitis following perforation into the peritoneal cavity.
Secondary Symptoms
- Anemia
- Back pain due to invasion of sacral plexus
- Urinary symptoms due to infiltration of bladder or prostate
- Ascites, liver secondary’s
- Peritonitis following perforation into the peritoneal cavity.
Signs
- Piles mass due to proximal venous congestion by tumor
- Fistula in perianal region which itself is tumor extension into anal canal
- Pallor Rare Manifestation
- Fistula formation into the adjacent organs
- Fever of unknown origin
- Abscess (due to localized perforated Ca)
- Bacteremia or sepsis
Pre-Rectal Examination
Digital Rectal Examination: 90% of the mass can be felt by DRE. Superficial mass is mobile while deep penetrating tumor is immobile. Typical induration is felt in RCa. When the center ulcerates, a shallow depression will be found, with raised and everted edges. After the finger has been withdrawn, if it has been in direct contact with carcinoma, it gets smeared with blood or mucopurulent material tinged with blood. In higher growth, at the recto-sigmoid junction, bimanual examination should be performed. The one finger in the rectum and another hand on the lower abdomen may feel such carcinoma. In case of female patient, one finger in the rectum and another is in the vagina may provide the idea of extension of the growth, usually when the neoplasm is situated on the anterior wall of the rectum. When the carcinoma is situated in distal third of the rectum, involved lymph nodes can sometimes be felt as one or more, hard, oval swellings in the mesorectum posteriorly or postero-laterally above the tumors. Abdominal Examination: It is normal usually but may reveal hepatomegaly or palpable liver metastases or ascites in case of liver metastasis. When an advanced annular tumor is situated at recto sigmoid junction, signs of obstruction of large intestine are present.
Investigations
- Stool test
- Fecal Occult Blood test
- Proctoscopy
- Sigmoidoscopy
- Colonoscopy is ideal to rule out presence of any synchronous growths proximally (5%) or polyps. It helps to visualize full length of the colon. Proctosigmoidoscopy is must to identify the precise location of the tumor and to measure the tumor distance from anal sphincter accurately.
- Biopsy using Yeoman’s forceps
- Ultrasound Abdomen to look for secondary’s in liver, ascities.
- CT scan to see operability, local extension, size, nodal status, ureteral involvement, presence of perforation or fistula. Ct is very useful to assess nodal status. Local extension is better assessed by TRUS. Any mesorectal node detected in CT scan is considered as malignant spread. Liver secondary’s are well-identified in CT. Ureteral involvement in CT scan signifies requirement of stenting prior to surgery. Chest CT is essential to look for secondaries.
- Trans-rectal Ultrasonography (TRUS)/ Endo-rectal Ultrasonography- It is very useful to assess the extent of the tumor. It gives more accurate picture of primary tumor, layers, perirectal tissues and nodes. It is superior is T staging of rectal cancers. TRUS detects nodes more or equal to 5mm size.
- Endo-rectal coil MRI (EC MRI) - It gives larger field of view compared to TRUS. Extents, adjacent organ spread are better assessed by MRI.
- Barium enema in case of FAP and synchronous growth.
- Fluorine - 18 fluro de-oxy flucose PET scan is useful to detect recurrent local tumors, metastatic diseases, to detect pathologic response in preoperative chemo- radiation. PET is not accurate for nodal spread.
- Blood Test
- Serum markers; CEA (Carcino Embryonic Antigen) Estimation- it is raised in metastatic disease. It is important during follow-up after treatment.
- CA19-9 Carbohydrate antigen 19-9.
Screening
Screening in Average Risk Person: Colorectal cancer screening can be done by structural examination in diagnosing adenomatous polyps and adenocarcinoma via Colonoscopy, Flexible Sigmoidoscopy, Double Contrast Barium Enema and Computed Tomography Colonoscopy in every 5 or 10 years. Screening for detection of cancer can be done by stool test; guaiac-based Fecal Occult Blood Test (gFOBT), immunochemical based Fecal Occult Blood Test (iFOBT) done annually or Fecal DNA test with high sensitivity for cancer -American Cancer Society [7]. Screening for High-Risk Person: As per American College of Gastro Enterology, screening with colonoscopy is recommended in every 10 years beginning at age 50 for person with single 1st degree relatives diagnosed at age 60 or older with CRC or advanced adenoma. The American Gastroenterological Association recommended screening after 8 years of age in patients with pancolitis and after 15 years of age in patient with left sided colitis using colonoscopy every 1-2 years. American Society of Gastrointestinal Endoscopy recommends obtaining 4 biopsies from every
10 cm of colon from caecum to the rectum during each colonoscopy.
Spread
Once the diagnosis of rectal cancer is established, the local and distant extent of tumor should be determined for further therapeutic approach. Local Spread: The local spread is circumferential initially. It takes a period of 6 months for involvement of a quarter and 18-24 months to complete the circumference and later spreads out to the muscular coat and the perirectal tissues. Later, it spreads anteriorly to urinary bladder, prostate, seminal vesicles in males and uterus and vagina in females. Posteriorly into the sacrum and sacral plexus, laterally into the ureter. Downward spread of more than a centimeter is rare. Venous Spread: Based on venous drainage of upper rectum via portal system, most common site of hematogenous metastasis is liver (34%), followed by the lungs (22%), adrenals (11%), bone, brain and other areas. Distal rectum drains into inferior rectal veins and then into IVC and it may metastasize initially to lungs. Lymphatic Spread: Above the peritoneal reflection, spread occurs upwards along the colonic lymph nodes. In mid- rectum, into the para rectal and mid-rectal lymph nodes. Downward spread is rare, occurs when growth is close to the anal canal into the inguinal lymph nodes. Obturtator nodes nay be involved in 8% of lower rectal growths. Perineural Spread: It carries poor prognosis. Peritoneal Dissemination Spread: It may follow penetration of peritoneal coat by a high- lying rectal carcinoma.
Staging
TNM Staging of Rectal Cancer (Tables 1-10) [8]
| Tx | Primary not assessed |
| To | No primary tumor |
| Tis | Carcinoma in situ: intraepithelial or invasion into lamina propria |
| T1 | Sub mucosa |
| T2 | Muscularis propria |
| T3 | Sub serous/perirectal tissue |
| T3 | T3a<1mm, |
| T3 | T3b 1-5mm, |
| T3 | T3c 5-15mm, |
| T3 | T3d 15+mm |
| T4 | T4a -Perforation into visceral peritoneum, |
| T4 | T4b - Invasion to other organs |
Table 4: Tumour -T.
| Mo | No distant metastases |
|---|---|
| Spread | Distant metastasis |
| Spread | M1a- One distant organ (liver/lungs/ovary) or set of non-regional lymph nodes |
| Spread | M1b - More than one organ or site or to the peritoneum |
Table 1: Grading of distant metastasis-M.
| Nx | Nodes cannot be assessed | |
|---|---|---|
| No | No nodal spread | |
| N1 | Regional nodes 1-3 involved | |
| N1 | N1a - 1 regional node | |
| N1 | N1b - 2 to 3 regional nodes | |
| N1 | N1c - Tumour deposits in serosa/ mesentery/ non-peritonealised pericolic or perirectal tissues without regional nodes | |
| N1 | N2 | Regional nodes 4 or more involved |
| N2a - 4 to 6 regional nodes | N2 | |
| N2b - 7 or more regional nodes | N2 | |
Table 2: Regional Nodes- N.
| Vo | No venous invasion |
| V1 | Presence of venous invasion |
| Lo | No lymphatic vessel invasion |
| L1 | Presence of lymphatic vessel invasion |
Table 3: Vessel’s involvement.
| Ro | No residual tumour | |
|---|---|---|
| Tx | No residual tumour | |
| To | Microscopic residual tumour | |
| Tis | Macroscopic residual tumour |
Table 5: Residual tumor after resection-R.
| T2 | Muscularis propria |
| T3 | Sub serous/perirectal tissue |
| T3 | T3a<1mm, |
| T3 | T3b 1-5mm, |
| T3 | T3c 5-15mm, |
| T3 | T3d 15+mm |
| I | T1-2, No, Mo |
| IIA | T3, No, Mo |
| IIB | T4a, No, Mo |
| IIC | T4b, No, Mo |
| IIIA | T1-2, N1/N1c, Mo; |
| IIIA | T1, N2a, Mo |
| IIIB | T3-T4a, N1/N1c, Mo; |
| IIIB | T2-T3, N2a, Mo; |
| IIIB | T1-2,N2b, Mo |
| IIIC | T4a, N2a, Mo; |
| IIIC | T3-4a, N2b, Mo; |
| IIIC | T4b, N1-2, Mo |
| IVA | T1-4, N1-2, M1a |
| IVB | T1-4, N1-2, M1b |
Table 6: Histological grade-G.
| A | Confined to bowel wall, mucosa and sub mucosa |
| B | Extends across the bowel wall to the muscularis propria with no lymph nodes involved |
| C | Lymph nodes are involved |
Table 7: Duke’s staging of Carcinoma Rectum.
| A | Growth limited to the rectal wall |
| B | Growth extending into extra rectal tissues but no lymph node spread (35%) |
| B | B1- Invading muscularis mucosa |
| B | B2- Invading into or through the serosa |
| C | Lymph node secondaries (50%) |
| D | Distant spread to liver, lungs, bone, brain |
Table 8: Modified Duke’s staging.
| A | Intramucosal |
| B | B1 - Involvement up to muscularis propria |
| B | B2- Spread through the wall in to peritoneum |
| C | C1 - B1 + involvement of lymph nodes |
| C | C2 - B2 + involvement of lymph nodes |
| D | Distant spread |
Table 9: Astler-Coller’s Grading of Rectal cancer.
Differential Diagnosis
When an adenoma shows evidence of induration or unusual friability, it is almost certain that the malignancy has occurred, even in spite of biopsy findings to be contrary. On the other hand, biopsy in invaluable in distinguishing carcinoma from an inflammatory structure or an amoebic granuloma. The possibility of a neoplasm being endometrioma should always be considered in patients with dysmenorrhea. The possibility of carcinoid tumor in atypical cases must be remembered. In the last four instances, the biopsy should establish the correct diagnosis. The solitary ulcer syndrome should also be ruled out.
Treatment
Surgery is the mainstay of treatment. Preoperative chemo-radiotherapy is often used if growth is invading into adjacent tissues (T4). Adjuvant chemotherapy and radiotherapy is a must.
Abdomino-perineal resection
Indication - APR is the treatment of choice when meso- rectum is involved or when it is poorly differentiated tumor or when nodes are involved. It gives adequate clearance. Here, sigmoid, descending colon and upper rectum is mobilized per abdominally. Anal canal with perianal and perirectal tissues are dissected per anally. Retained colon is brought out as end colostomy in left iliac fossa.
Types
- Miles-abdomen first, perineum later
- Gabriel-perineum first, abdomen later
- Lloyd-Davies-synchronized Procedure Incision-Lower midline Position-Lithotomy Anesthesia-General or Spinal Painting and draping-As per standard protocol Abdominal Approach
- Abdomen opened in layers.
- Left-sided colon and entire rectum is mobilized from above. Rectum is mobilized posteriorly in avascular plane in front of nerve plane (hypo-gastric nerve) between meso-rectum and sacrum.
- Inferior mesenteric artery is ligated high proximal at its origin or just beyond its first branch.
- Colon is transected and proximal cut end is fashioned for end colostomy in left iliac fossa.
Perineal Approach
- Through perineum, a purse string suture is placed around anal margin.
- Circumferential incision is placed around the anus.
- Dissection is deepened using scissor and cautery into the perineal body, coccyx, ischial tuberosity, ischiorectal fossa. First posterior and lateral dissections are undertaken until it reaches above. Lastly, anterior dissection is done to reach above and specimen is removed through perineal wound.
- Perineal wound is closed in layers often with a drain. Abdomen drain is placed. Colostomy is created by suturing skin to mucosa using silk.
Complications
- Bleeding
- Infection of perineal wound
- Complications of colostomy like prolapse, stenosis, and infection
- Injury to urinary system, ureter, impotence, urinary incontinence
- Operative mortality is less than 2%.
Anterior resection
Indication
- Upper and middle third rectal growth
- Above peritoneal reflection
- Well-differentiated tumor
- 4 cm size tumor
- In females, growth 7 cm above the anal verge
- T1-2 No tumor
- Tumor without lymphatic or venous spread Types
- Anterior resection (AR) / anterior proctosigmoidectomy
- Low anterior resection (LAR)
Anterior resection
Procedure- Through abdominal approach, rectum above the peritoneal reflection is resected with colorectal anastomosis.
Low anterior resection
Procedure - Resection of rectum below the peritoneal reflection along with the sigmoid colon with total meso-rectal excision (TME) through abdominal approach and colorectal anastomosis using circular stapler device.
Advantages
- Avoids permanent colostomy.
- Sphincter is retained.
- Patient’s acceptance Disadvantages
- Uncertainty of clearance which is very important in cancer surgeries and so chances of local recurrence is high.
- Anastomotic leak
- Infection
- Stenosis Laparoscopic APR/AR Nowadays, these are gaining much popularity, Features being
- Dissection will be more meticulous.
- Less blood loss, less postoperative pain.
- Early bowel function.
- Clearance is same as open method in relation to primary tumor and nodes.
- Short hospital stay, mortality and morbidity are similar to open method.
- Port site recurrence chances are 0.5-2% (Earlier it was higher; now it has reduced due to proper technique, careful handling of the specimen, specimen isolation prior to extraction, trocar site irrigation with cytotoxic agents and povidone iodine).
Hartmann’s operation
Indication
- It is an excellent palliative procedure, done in elderly people who are not fit for major surgery like AP resection
- Locally advanced tumors.
Procedure: Rectal growth is resected and upper end of the rectum is closed completely. Proximal colon is brought out as end colostomy.
Pelvic evisceration (Brunschwig’s operation)
Procedure: It is removal of rectum with the tumor, all the lymph nodes, urinary bladder, fat, fascia, uterus, vagina, with colostomy and urinary diversion.
Palliative colostomy
Indication: It is done in advanced unresectable growth which presents with intestinal obstruction.
Neoadjuvant Therapy
Indication
- Strongly recommended for locally advanced cancers located in the middle or distal rectum.
- Presence of T4 rectal cancer
- Node positive disease Procedure: Short-course radiotherapy and long-course chemo radiotherapy are accepted approaches for delivering preoperative neoadjuvant therapy.
Adjuvant Therapy: It is given after the primary management of carcinoma. Postoperative chemo radiotherapy is the preferred adjuvant therapy for patients who have not received neo-adjuvant therapy.
Radiotherapy
Radiotherapy is beneficial when growth is below the level of peritoneal reflection. Only rectal adenocarcinoma in GIT responds well for radiotherapy.
Preoperative Radiotherapy: It is given to downstage the tumor so as to make it operatable by APR or AR Intraoperative Radiotherapy: It is used in pelvic wall diseases. It can cause peripheral neurotherapy and ureteral stenosis.
Postoperative radiotherapy: It is commonly used.
Course
- Short course 25 Gy in 5 fractions in 5 days.
- Long course 5040 Gy in 28 fractions in 6 weeks.
Chemotherapy
Indication
- Positive nodes
- T2 stage
- Blood spread
- Recurrent tumor
- Metastatic disease Agents used Endoxan, 5 FU, Semustine with Leucoverin (Folinic Acid) or Levamisole Biological agents like Bevacizumab VEGF receptor antagonist, Cetuximab EGFR antagonist.
Chemoradiotherapy
Indication
- To prevent recurrence after AR
- Locally advanced disease or metastatic disease
- Carcinoma of rectum presenting with obstruction, after loop colostomy Treatment of rectal cancer with liver metastases: For patients with resectable colon cancer with resectable liver metastases, resection of the primary tumor followed by hepatic resection is the preferred strategy. Treatment may start with short-course radiotherapy or a long course chemo-radiation followed by resection of the rectal cancer. Liver metastases will be resected at a later stage. Treatment of liver metastases consists of radical resection and/or local ablative therapy (e.g. radiofrequency ablation) combined with adjuvant chemotherapy. Liver-first approach is another alternative, in which resection of the liver metastases is performed first followed by a radiation therapy to the rectum and resection of the rectal cancer at a later stage [9].
Treatment of unresectable rectal cancer: A fixed or adhesive tumor that cannot be resected from adjacent organs without leaving microscopic or gross residual disease at local site might be consider as an unresectable tumor. Thin cut MRI with pelvic phased-array coil is the modality of choice in evaluating the local tumor resectability. Depth of transmural invasion, nodal involvement, invasion into adjacent structures and circumferential margins can be assessed using MRI. A multimodality plan including preoperative neoadjuvant chemo-radiotherapy, multi-visceral surgical resection (with or without intra-operative radiotherapy) and postoperative adjuvant chemotherapy are the current approach for unresectable rectal cancers. Multi-visceral resections, such as total pelvic exenteration (TPE), involve the removal of the rectum, anus, lower ureters, urinary bladder, and prostate in males; the uterus, ovaries and vagina are also removed in females. Posterior pelvic exenteration and supra-levator pelvic exenteration have also been studied.
Prognosis of Ca Rectum
- Prognostic factor is dependent on factors like
- Size of tumor
- Differentiation
- Mesorectal involvement
- Stages of disease
- Nodal status, Perineural spread
- Distant spread
- Circumferential resected margin
- Adjuvant therapy used
5 year survival is estimated to be
- 90%in Stage I
- 75% in Stage II
- 40% in Stage III
- 5% in Stage IV The prognosis of Ca rectum can be insured by regular colonoscopy, CEA assessment, PET scan, CT/MRI, and proper colostomy care in APR during follow-up.
Complications
Complications of rectal cancer include bowel obstruction, recurring cancer/developing another colorectal cancer, and metastatic disease.
Discussion
In this article, the anatomy and physiology of rectum, risk factors, pathogenesis, clinical types, clinical features, screening, diagnosis, spread, staging and treatment of rectal carcinoma have been reviewed along with the prognosis.
References
-
Chaurasia B (2019) Human Anatomy. 8th (Edn.), CBS Publishers and Distributors, pp: 2080.
-
Siegel R, Desantis C, Jemal A (2014) Colorectal cancer statistics, 2014. CA: A cancer journal for clinicians 64(2): 104-117.
-
GLOBOCAN (2012) Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012: International Agency for research on Cancer. World Health Organization.
-
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371(9612): 569-578.
-
Bhat MS (2013) SRB’s Manual of Surgery. 4th (Edn.), Jaypee Brothers Medical Publisher, pp: 1358.
-
Pareek A (2018) A Textbook of Ayurveda Surgery. 1st (Edn.), Chaukhamba Surabharati Prakashan.
-
Levin B, Lieberman DA, McFarland B, Andrews KS, Brooks D, et al. (2008) Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 134(5): 1570-1595.
-
Williams NS, Bulstrode CJK, Connell PRO (2008) Bailey and Love’s Short Practice of Surgery. 25th(Edn.), Hodder Arnold Publisher, pp: 1536.
-
Adam R (2007) Colorectal cancer with synchronous liver metastases. The British Journal of Surgery 94(2): 129- 131.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient