Pancreatitis-Panniculitis-Polyarthritis (PPP) Syndrome with Plexopathy
Triple P Syndrome or “Pancreatitis-Panniculitis-Polyarthritis (PPP) syndrome is a syndrome with unclear physiopathology comprising of rare pancreatic disease complications. There is very limited literature , mostly available in the case report forms, about this syndrome of pancreatitis along with extra-pancreatic manifestations like panniculitis and polyarthritis, and therefore often called “triple P” or ‘PPP syndrome’. We report a patient with 4th “P” which is Plexopathy in a patient with this “Triple P” syndrome. There is scanty literature and information about this type of presentation especially “4 P syndrome, instead of 3 P Syndrome”.
Introduction
We have seen a 38 year male, nonsmoker, nonalcoholic, with no prior co morbidities. He developed first episode of mild acute pancreatitis about 2 years back, which was treated conservatively. He again had similar recurrences of mild acute pancreatitis (4-5 episodes) over last 1.5 years. During the first episode of pancreatitis 2 years back, he had symmetrical polyarthritis involving bilateral wrist, bilateral ankle and bilateral knee joints, which was conservatively managed but he subsequently developed flexion deformity at knee and left ankle joints, other joints recovered. He also noticed subcutaneous nodules in both arms and over left leg. After 2 months of first pancreatitis episode, he also had decreased sensations in upper left arm and left elbow weakness. There is no accompanying cough, altered bowel habits, gastrointestinal bleeding, burning micturition, altered sensorium or decreased urine output. There is no history of any intoxications, indigenous medications, major surgeries, blood transfusions or drug abuse prior to onset of the disease.
During Examination in recent hospitalization, his vital parameters were normal, and joint examinations showed synovitis in left knee and both ankle joints with decreased range of movement, hyperextended left elbow along with sensory loss in left arm which is poorly demarcated .Other joint and spine examination was normal .There were multiple, sub-centimetric approx. 0.5- to 1-cm sized nodular lesions in left leg and bilateral forearms. Abdominal examination showed mild to moderate tenderness in epigastrium without rebound tenderness. Laboratory tests showed leukocytosis (white cells 18,000/cu. mm, neutrophils 91%) and raised C-reactive protein, 17.3 g/dL. Autoimmunity profile including antinuclear antibodies (ANA), Extractable Nuclear Antigen( ENA), Anti-double stranded DNA (Anti- dsDNA) antibodies, rheumatoid factor(RF), anti- CCP (cyclic citrullinated peptide) antibodies, antineutrophil cytoplasmic antibodies (ANCA), complement C3 and C4, were negative. X-Ray evaluation of involved joints did not show any articular/ bone changes. Arthrocentesis revealed a yellowish synovial fluid with no evidence of septic arthritis and no crystals. His initial labs including complete hemogram, liver function tests (LFT) and kidney function tests (KFT) were within normal limits. Serum amylase and lipase was 1937 U/L, 5714 U/L respectively. Blood and body fluid cultures were sterile. Metabolic parameters including serum calcium, phosphate (Po4), Vitamin D3, lipid profile and parathyroid hormone were within normal limits.
Contrast enhanced CT scans of Abdomen (pancreatic protocol) revealed diffuse pancreatic atrophy, mild peripancreatic fluid with thrombosis of segmental branches of left portal vein. There was no gallstone, no evidence of pancreatic divisum and normal common bile duct. Subsequently Endoscopic Retrograde Cholangio- Pancreatography (ERCP) showed short stricture of main pancreatic duct at head region with changes of chronic pancreatitis. A 5F plastic stent was placed in main pancreatic duct. Biopsy from subcutaneous nodule was suggestive of eosinophilic panniculitis. He also had weakness in left upper limb that was diagnosed to have brachial plexopathy on nerve conduction studies. Based on a fore mentioned details, patient had recurrent mild acute exacerbation of chronic pancreatitis, without endocrine or exocrine insufficiency. A provisional diagnosis of PPP syndrome was made in view of recurrent acute pancreatitis, panniculitis and undifferentiated deforming polyarthritis with Plexopathy. Pancreatitis episodes were effectively managed conservatively with analgesics, bowel rest and intravenous fluids. For his arthritis, a short course of systemic steroids was given, methylprednisolone, started with 60 mg once daily, with weekly tapering along with intrarticular steroid therapy in joints which resulted in a modest benefit in pain without improvement in joint deformity. His Plexopathy was managed in consultation with neurologist with short course of steroids along with neuromodulators like pregabalin and amitriptyline without significant improvement.
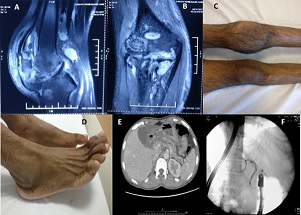
Figure 1: A & B) MRI of knee joints showing joint effusion, soft tissue swelling and inflammation along with erosion in articular surface, joint deformity with Bone marrow edema. C) Left knee joint synovitis with effusion. D) Right ankle joint synovitis. E) CT abdomen showing- Atrophic pancreas with dilated main pancreatic duct (MPD), mild peri-pancreatic fluid with thrombosis of segmental branches of left portal vein. F) Fluoroscopic image showed pancreatic head short stricture with mildly dilated and irregular main pancreatic duct.
Pancreatitis-Panniculitis-Polyarthritis (PPP) syndrome is rare manifestation in a patient with recurrent acute pancreatitis only 33 cases [1] have been reported in the literature till date, mostly reported in middle-aged male with a history of heavy alcohol abuse. It can precede the pancreatic disease and can coincide or succeed the pancreatic diseases as well. The pathogenesis of this syndrome is not clear, but most widely accepted and popular theory consider that as a result of pancreatitis , serum lipases level increases, which results in extravasation of serum lipase into the peripheral tissues and also penetrates into the periarticular space, which results in lipolysis and secondary inflammation in peripheral tissues, and results in its clinical manifestations like subcutaneous tissues involvements results in panniculitis and joints involvement causes polyarthritis, similarly neural involvement can results in plexopathy. Extensive investigations had shown high levels of fatty acids and pancreatic lipase in the affected tissues [2].
Pancreatic panniculitis is an infrequent complication that is characterized by fat necrosis of the retroperitoneum, mesentery, omentum and lower limbs. Pancreatic panniculitis can occur in 2-3 % of patients with pancreatitis, first described by Chiari in 1883 [3]. Arthritis is much rarer and can occur as severe monoarthritis, but more often as symmetric polyarthritis [4] of the ankle, knees, wrists, metacarpal joints, elbows and tarsal joints, following the distribution of the cutaneous manifestations. PPP can present with prolonged pyrexia [5], pancreticoplural fistula [6]. We suggest a detailed history and examination should be directed towards the “triple P “ components and also should not get misguided with other etiologies , as management of “triple P” components is directed toward the treatment of underlying pancreatitis and its cause . The clinician who is dealing with pancreatic diseases, should be aware of the “triple P or PPP syndrome”, as its early diagnosis, recognition is paramount for management and patient care (Figure 1).
Conclusion
Pancreatitis can have extra pancreatic manifestations like Panniculitis, Polyarthritis, plexopathy. Early recognition, diagnosis and treatment is of crucial importance.
References
-
Dieker W, Derer J, Henzler T, Schneider A, Ruckert F, et al. (2017) Pancreatitis, panniculitis and polyarthritis (PPP) syndrome caused by post-pancreatitis pseudocyst with mesenteric fistula. Diagnosis and successful surgical treatment. Case report and review of literature. International Journal of Surgery Case Reports 31: 170- 175.
-
Loverdos I, Swan MC, Shekherdimian S, Rasheed AAA, Schneider R, et al. (2015) A case of pancreatitis, panniculitis and polyarthritis syndrome: Elucidating the pathophysiologic mechanisms of a rare condition. J Pediatr Surg Case Rep 3(5): 223-226.
-
Laureano A, Mestre T, Ricardo L, Rodrigues AM, Cardoso J (2014) Pancreatic panniculitis - a cutaneous manifestation of acute pancreatitis. J Dermatol Case Rep 8(1): 35-37.
-
Narvaez J, Bianchi MM, Santo P, Fuente DDl, Rodriguez VR, et al. (2010) Pancreatitis, panniculitis, and polyarthritis. Semin Arthritis Rheum 39(5): 417-423.
-
Jose T, Biju IK, Kumar A, Anver PC, Kuruvila R, et al. (2009) Pancreatitis, polyarthritis, panniculitis syndrome (PPP syndrome) plus prolonged pyrexia--a rare presentation of chronic pancreatitis. Indian J Gastroenterol 28(5): 186-188.
-
Vorawut Thanthitaweewat, Wongkarnjana A, Chirakalwasan N (2017) Pancreatitis panniculitis and polyarthritis (PPP) syndrome with Pancreatico pleural fistula: Case Report. European Respiratory Journal 50(61).
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient