The menace of Anesthetic Agents used for Intentional Self-harm by Healthcare Professionals
The incidences of suicide cases are alarmingly increasing among healthcare professionals. The common causes are distress from burnout and an uninterrupted work schedule leading to disrupted family life. The young professionals succumb to the frustrations of the workplace stressors like - diminished autonomy, poor self-care, unrewarding, incessant workload. Usually, female healthcare professionals are at greater risk for suicide. The suicides mostly took place at the workplace; if not all, in most cases, the stressor for self-harm is related to the victim's profession. And almost all cases that took place at the workplace were due to fatal drug overdose or toxicity. This is probably due to the easy accessibility of healthcare professionals to dangerous drugs. Using insulin and intravenous anesthetics agents are common modes of intentional self-harm among healthcare professionals. In both situations, postmortem detection becomes challenging and fixing the exact cause and the manner of death thereof. Here, we have discussed a suicide case of a scrub nurse from the General Surgery Department using intravenous vecuronium bromide.
Background
Suicide is the second leading cause of death following road traffic accidents. According to WHO, 8,00,000 people die yearly due to suicide, of which 79% occur in developing countries. The rate has increased to 60% in the past 45 years [1]. Suicide risk increased in certain occupational groups, especially medical professionals (Physicians) [2]. Healthcare workers, such as nurses, were categorized as a high-risk group for suicide in different countries. The most common method of suicide among medical and paramedical professionals in the western population is poisoning, followed by firearm. Among poisoning, drug overdose is the most common method adopted by medical-related professionals. A review of studies conducted globally across many countries indicated a relative risk ranges between 1.1 and 3.4 in male doctors and 2.5 and 5.7 in female doctors. Barbiturates were the most frequently used drug, and anaesthesiologists were higher in suicide rates among medical professionals. Half of the anaesthesiologists committed to using anesthetic drugs. Among anaesthetic drugs induction agents, e.g. propofol) most commonly used, followed by neuromuscular blockers, e.g. Atracurium, Vecuronium bromide [3]. The suicide rates among medical professionals are because the doctors and paramedics have easy access to drugs and knowledge about medications and their lethal dosage [4]. Here, we discuss a fatal case report of a young female nurse from the surgery department who committed suicide by self-injection of an anesthetic agent, vecuronium bromide. Though vecuronium bromide is not uncommon, this case highlights the pharmacokinetics of the drug and importance of skin bit from injection site for toxicological analysis.
Case Report
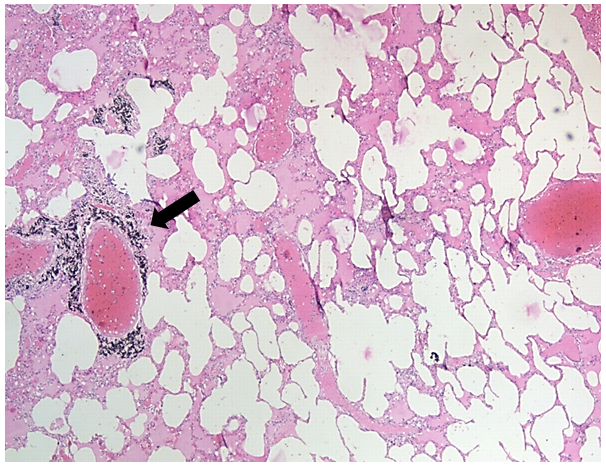
A 24 year-old-female, a paramedical (scrub nurse) staff, was found unresponsive in her retiring room by her duty reliever nursing staff at early morning 7am. Her colleague tried to knock on the door during the shift change time at 7am. When there was no response from within, the door was broke opened. She was found to be dead for long hours on her bed in the retiring room adjacent to the operation theater. Police intimation was given, and the police requested an autopsy. Autopsy examination revealed multiple injection marks in the left cubital fossa and left dorsum of the hand. The postmortem changes showed a death interval within 12-16 hours. Dissection revealed all organs were found to be congested and oedematous. Both lungs were edematous and congested to a variable degree. Toxicological analysis of samples like femoral blood, bile, viscera and skin bits from the injection sites was made at the concerned state forensic laboratory. In addition, tissue bits from the injection site, lungs, liver, and kidneys were collected for histopathological analysis. From the scene of scene occurrence, two empty vials of vecuronium bromide, distilled water, and an intravenous venflon set was recovered by the police and sent for the toxicological confirmation. Chemical analysis reports detected the presence of vecuronium bromide in all samples (Figure 1). Histopathology analysis of lungs showed alveolar rupture with edema, liver and kidney appearing normal (Figure 2). The cause of death was due to vecuronium bromide and its complications. The manner is intentional self-harm.
The macerated Visceral samples were soaked in rectified spirit and acetic acid for 12hrs, and the extract was filtered and dried. The dried residue was dissolved in water and basified with aqueous ammonia extracted with chloroform and ether (1:3) in ratio. The organic layer was separated, dried, and dissolved in methanol. A control sample of vecuronium bromide was spotted on TLC using a solvent system to give orange color spots with Dagendroff’s reagent.
Discussion
Vecuronium bromide is a steroidal mono-quaternary neuromuscular blocking agent with an intermediate duration of action (20-50min). The presence of acetyl ester in its structure facilitates the interaction of steroidal compounds with nicotinic acetylcholine receptors at the post synaptic muscle membrane. Vecuronium bromide is a commonly used muscle relaxant during anaesthetic procedures administered at its usual ED95 dose of 0.1mg/kg with a peak of onset of action at 3-5minutes [5, 6, 7].
Vecuronium bromide is primarily metabolised in the liver (70%) and eliminated by kidney thereafter. Around 30- 40% of vecuronium is cleared in the bile as parent compound. Thus the duration of vecuronium-induced neuromuscular blockade is dependent primarily on hepatic function and to a lesser extent on renal function. Vecuronium bromide is metabolized in the liver by deacetylation into three possible metabolites, 3-OH, 17-OH, and 3,17-di-OH vecuronium. The 3-OH vecuronium metabolite has 80% the neuromuscular blocking potency of vecuronium. Vecuronium is available as a lyophilized powder because of its lesser stability in its solution form. On intravenous administration, due to its high lipophilic nature, drug molecules enter neuromuscular junction quickly via circulation. The peak onset of action starts within 3-5minutes as the drug molecule reaches the neuromuscular junction and blocks the neuromuscular transmission causing skeletal muscle paralysis [5, 6, 7, 8]. In our case, the patient has injected two ampoules of vecuronium bromide (16mg) twice the recommended dose for anaesthetics induction and intubation of the trachea. With its immediate onset of action, the patient might have developed respiratory paralysis and died immediately after its administration. In toxicological analysis, this is the important reason for detecting vecuronium bromide in tissues like the liver, kidney, and blood, because the liver metabolizes less quantity. The respiratory muscle paralysis leading to violent respiratory activity had led to massive intra-alveolar haemorrhage and oedema in this case.
Similar case reports by Khanna R, et al. have also demonstrated vecuronium bromide in viscera, blood and skin using Gas-Chromatography-Mass Spectrophotometer (GC-MS) and Thin Layer Chromatography (TLC) techniques [9].
Yadukul, et al. reported a similar case of suicidal death in a paramedic using vecuronium bromide at her workplace. However, in this case report, only the skin bit detected the presence of vecuronium bromide, rest of the viscera samples are negative [10]. In these two cases, the skin bit samples showed positive even when toxicological analyses of other samples like blood and viscera were negative. This may be either due to incorrect sample collection/transport or may be due to faulty toxicological analysis.
There are challenges associated with detecting such anesthetic agents or other drugs like insulin used for suicidal purposes by the healthcare workers. The results may be affected by many factors like the duration of death, sample collection and analysis techniques, and mixed with other drugs or poisons like alcohol, morphine, etc., which further complicate the issues. Hence, the forensic pathologist should consider all such possibilities before concluding an opinion.
Conclusion
Before forming an opinion as to the cause and the manner of death, one should be mindful that the detection methods in anesthetic deaths can be influenced by many inherent factors, i.e. sample collection, preservation, transport, analysis technique, duration of death, physical composition of the deceased and co-poisoning by the other agents like alcohol, morphine, etc.
The workplace-related health risks from burnout, anxiety and depression primarily blur the reasoning capacity and suicide ideation thereof. And this mostly leads to alcohol or other substances that create a vicious cycle of diminished cognitive ability.
Conflict of Interest: The authors don’t have any conflict of interest to disclose in relation to this paper.
Funding: None
Recommendations
- Early detection and intervention of signs of workplace stress of a healthcare professional should be the primary responsibility of the employer and the policy makers, i.e. measures to reduce burnout and compassion fatigue at the workplace.
- In India, many healthcare organizations offer lifestyle management approaches, e.g. yoga, pranayam, meditation and other contemplative practices, to their employees for stress and burnout management.
- The healthcare organizations should design their policy to reduce the time and task burdens imposed by busy schedules for the healthcare professionals. In addition, mental health counseling, physician wellness programs and work-and-life management techniques may offer a practical benefit to healthcare workers.
References
-
World health organisation (2020) Suicide data.
-
Milner AJ, Maheen H, Bismark MM, Spittal MJ (2016) Suicide by health professionals: a retrospective mortality study in Australia. Med J Aust 205(6): 260-265.
-
Yentis SM, Shinde S, Plunkett E, Mortimore A (2019) Suicide amongst anaesthetists–an Association of Anaesthetists survey. Anesthesia 74(11): 1365-1373.
-
Hawton K, Clements A, Simkin S, Malmberg A (2000) Doctors who kill themselves: a study of the methods used for suicide. Q J Med 93(6): 351-357.
-
Hunter JM (2001) Muscle function and neuromuscular blockade. In: Aitkenhead AR, Rowbotham DJ, et al. (Eds.), Textbook of Anesthesia. London: Churchill Livingstone, pp: 223-235.
-
Atherton DP, Hunter JM (1999) Clinical pharmacokinetics of the newer neuromuscular blocking drugs. Clin Pharmacokinet 36(3): 169-189.
-
Flood P, Rathmell JP, Shafer S (2014) Stoelting’s Pharmacology & Physiology in Anesthetic Practice. Philadelphia: LWW, pp: 544.
-
Jonas AA, Hunter JM (2004) Pharmacology of neuromuscular blocking drugs. Contin Educ Anaesth Crit Care Pain 4(1): 2-7.
-
Khanna R, Sharma RS (2015) Detection of metabolites of vecuronium bromide in visceral samples solves a typical death mystery-(toxicokinetics-studies using Gc- Ms technique). Acta Medica International 2(1): 125-133.
-
Yadukul S, Suresh V, Havanur B (2014) Paramedic Suicide with Vecuronium Bromide – A Case Report. J Forensic Toxicol Pharmacol 3(3).
- Forensic Implications of Adverse Drug Reactions in Schizophrenia A Case Series
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers