Cystic Adenoid Carcinomas of the Parotid: About 3 Cases and Review of Literature
Adenoids cystic carcinomas (CAKs) represent 2-4% of parotid tumors and 12% of malignant tumors. These are slow growing tumors that are characterized by their ability to infiltrate the nerve sheaths. We collected three cases of CAK of the parotid gland diagnosed and treated between 2012 and 2018. These were 03 women who consulted in front of the appearance of a swelling of the parotid compartment associated with a facial paralysis in a case. The lymph node areas were free. All patients underwent exploration including ultrasound, CT in one case, and MRI in one patient. Treatment consisted of a total parotidectomy associated with lymph node dissection in all cases and additional radiotherapy. The evolution was favorable in two cases. The adenoid cystic carcinoma of the parotid is a rare tumor, characterized by a very slow evolution, a local aggressiveness, a strongly recurrent character locally and a high metastatic capacity at a distance.
Introduction
Head and neck adenoid cystic carcinomas (CAKs) are malignant epithelial tumors that develop mainly in the salivary glands and mainly in the parotid gland. These tumors are relatively rare (2 to 4% of parotid tumors and 12% of malignant tumors), and are characterized by their ability to infiltrate the nerve sheaths. Their development is marked by frequent local recurrences after surgical treatment and by the appearance of distant metastases. We report three cases of adenoid cystic carcinoma with parotid localization. The aim of our study is to define the clinical characteristics of parotid CAK and to identify the prognostic factors.
Observations
Observation n°1
This was an 82-year-old patient who saw us for a swelling of the left parotid pocket that had progressed for 6 months, gradually increasing in size. On clinical examination, there was a swelling of the left parotid compartment which was 2cm long along the axis with healthy looking skin. The cervical lymph node areas were free. The patient also did not have trismus or facial paralysis. The Steno hole was free.
A cervical ultrasound was performed showing tissue formation of the parotid gland of 20mm. The exploration was completed by a TAP CT showing a 20mm intra-parotid nodule which was heterogeneously enhanced after injection of contrast product. An exofacial parotidectomy without lymph node dissection was performed and the histological examination was in favor of adenoid cystic carcinoma (Figure 1A). The operative consequences were simple marked by a transient facial paralysis. The tumor was classified T3N0M0. Our patient received postoperative three-dimensional (3D) radiotherapy at a dose of 70Gy in 35fractions of 2Gy per fraction, 05days over 07days over a 58-day spread, weekly monitoring of the patient showed mucositis and mycosis in the course of treatment having received symptomatic treatment with good improvement, the evolution was favorable with a follow-up of 06 years.
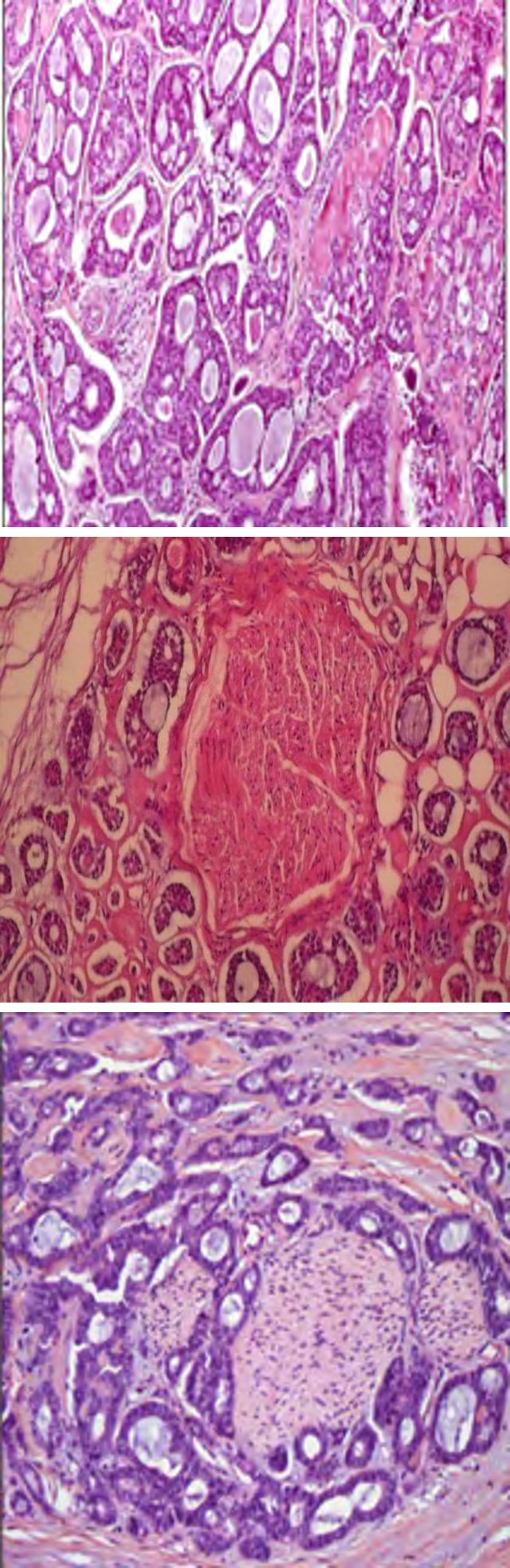
Figure 1A: The 1st case.
Observation n°2
It was a 56-year-old woman who consulted us for an isolated swelling of the right parotid compartment which had progressed for 5 months. Clinical examination showed a right parotid swelling 3 cm in diameter, well defined and of firm consistency. The patient also had no cervical lymphadenopathy, facial paralysis or trismus. The salivary gland ultrasound revealed a hypoechoic, homogeneous, well-encapsulated 30 mm formation within the right parotid gland. An exofacial parotidectomy was performed and the extemporaneous anatomopathological examination concluded in a cylindroma; hence the performance of a total parotidectomy without lymph node dissection. The definitive pathological examination was in favor of an adenoid cystic carcinoma of the parotid (Figure 1B) but without adjacent parotid involvement. The extension record was negative. The tumor was classified T1N0M0. Our patient received conformational intensity-modulated radiotherapy (IMRG) at a dose of 66 Gy in 33 fractions over a 58-day spread with a favorable outcome and no recurrence at a follow-up of 3 years and 3 months.
Figure 1B: 2nd case.
Observation n°3
This is an 18-year-old woman with swelling of the left parotid compartment without facial nerve involvement. Without notable pathological history. Clinical examination revealed a left retro-Angelo-mandibular swelling 2 cm long, hard, painful, fixed in relation to the deep and superficial plane with the onset of skin infiltration. The lymph node areas were free. Ultrasound showed a hypoechoic, heterogeneous formation of the left parotid gland measuring 30 x 30 mm, poorly limited with left intra-parotid lymph nodes, left jugulocarotid and bilateral centimetric submaxillae. The exploration was completed by a tomodensitometric examination which objectified a tissue mass at the expense of the left parotid gland which was enhanced heterogeneously after injection of contrast product.
Figure 1C: 3rd case.
Histological study shows adenoid cystic carcinoma with HE 100 nerve infiltration (A).
A total parotidectomy was performed with sacrifice of the facial nerve which was infiltrated by the tumor. This procedure was completed by a complete conservative functional left dissection associated with resection of the lesion of the scalp. Histology was in favor of a 2 cm adenoid cystic carcinoma with peri-nervous infiltration (Figure 1C).
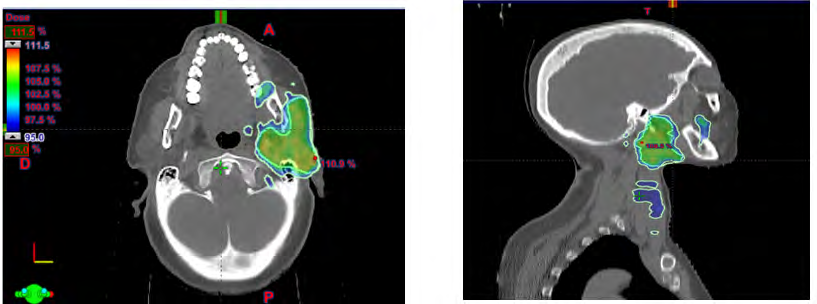
The excisional limits were sound. Lymph node dissection brought back 30 lymph nodes, 10 of which were metastatic without capsular rupture. The tumor was classified T4a N2b M0. The patient underwent conformational intensity- modulated radiotherapy (IMRG) in post; at a dose of 66 Gy in 33 fractions over a spread of 58 days (Figure 2). The course was marked by lymph node recurrence after 2 years, treated with radiotherapy and then our patient was lost to follow-up.
Discussion
Cervicofacial adenoid cystic carcinomas (CAKs) are relatively rare malignant epithelial tumors (less than 1% of cervicofacial malignancies). They mainly develop in the accessory and main salivary glands, lacrimal glands and mucous glands of the nasal cavities and para-nasal sinuses. These tumors represent 5% of all major salivary gland tumors. The parotid gland is the gland most often affected [1, 2]. A slight male predominance is noted in most series [2, 3]. In our series, the sex was female. CAKs are characterized by a very slow evolution, extending over 10 to 15 years and by local aggressiveness, with invasion of adjacent soft and bone tissues, and a tendency to follow areas of least resistance represented by the vasculo-sheaths. Nerves of the base, either by respecting them or by infiltrating them [3, 4, 5]. Due to their local aggressiveness, these carcinomas tend to recur locally, but metastases by hematogenous route are frequent. They affect the lungs in more than 70% of cases, but also the bone and the liver [4, 5]. Brain metastases are single or multiple. Lymph node metastases are more likely to occur with solid tumors, regardless of their location, and have a poor prognosis. Bone and extradural spinal metastasis have also been reported [5, 6]. Other, rarer sites have been described in the skin, subcutaneous tissue, hand, thyroid and pleura [5, 7]. In our study, No distant metastasis was noted. Clinically, the presentation is that of a hard, painful parotid swelling with slowly progressive facial paralysis successively involving all branches of the facial nerve [2]. In our series, facial paralysis was observed in one patient by perinervous tumor infiltration. From a histological point of view, CAKs are tumors composed of cylindrical cell cords enclosed in an amorphous tubular sheath. The tumor is composed of cylindromatous tissue; hence the old name “cylindroma”. This cylindromatous tissue should be distinguished from the cylindrical space surrounded by small cells, characteristic of salivary tissue [8]. Two cellular contingents are present: myoepithelial and ductal secreting.
Three different histological types of CAK are described [8]:
- The tubular type, in which the tumor cells are organized around tubular cavities containing PAS positive mucus
- The cribriform or glandular type, where the tumor cells are grouped in cellular cords, hollowed out with rounded cavities containing mucoid or hyaline cylinders
- The solid type, where the monomorphic tumor cells are organized in a sheet, hyperchromatic, sometimes with areas of necrosis.
The three histological types are often all present within the same tumor. The tumor is classified according to the predominant histologic type which determines the prognosis: the tubular type has the best prognosis, the most undifferentiated solid form the worst with a survival of 5% at 15 years [9]. The glandular form being of intermediate prognosis.
The other prognostic factors are tumor location, size, degree of bone, nerve and lymph node invasion and the presence of tumor tissue on the resection margins. Treatment is mainly surgical, consisting of total parotidectomy with conservation of the facial nerve if possible with complete cervical lymph node dissection in the event of lymph node metastasis associated with postoperative radiotherapy at a dose of 64 Gy [9]. The sacrifice of the facial nerve is only carried out in the event of nerve infiltration by the tumor, which was the case in one of our patients. In our series, lymph node dissection including zones IIa, IIb is systematically performed with an extemporaneous histological examination which, in the event of positivity, would encourage us to perform ipsilateral functional lymph node dissection. Postoperative radiotherapy allows local control of the lesions avoiding the risk of recurrence, especially in cases where the resection limits are healthy [10]. Chemotherapy is sometimes offered alone or in combination with radiotherapy. The most widely used agents are cisplatin and epirubicin.
Chemotherapy is usually reserved for rapidly progressing CAKs, locoregional recurrences, and distant metastases when symptoms are not improved by other treatments [5, 9, 11]. The benefit of chemotherapy is moderate, with a disappointing response rate (from 0 to 30% depending on the studies) because CAKs are slowly proliferating tumors. Rafael [12] mentioned the role of Imatinib mesylate (Glivec or Gleevec at a dose of 400 mg/day) which is an inhibitor of protein tyrosine kinases having a role in the proliferation of tumor cells, with an antitumor effect but the results are not satisfactory.
The prognosis is poor in case of [9, 10]:
- Age> 45 years old,
- Rapid clinical course (<18 months),
- Advanced clinical stage,
- Solid histological type,
- Nerve damage or invaded resection margins.
Survival is around 75% at 5 years and 20% at 20 years [13].
Conclusion
The adenoid cystic carcinoma of the parotid is a rare tumor, characterized by a very slow evolution, a local aggressiveness, a strongly recurrent character locally and a high metastatic capacity at a distance. The treatment combines a total parotidectomy, lymph node dissection and additional radiotherapy. The prognosis is generally poor.
References
-
Hallacq P, Labrousse F, Roullet B, Orsel S, Bessede JP, et al. (2001) Adenoid cystic carcinomas invading the skull base. Apropos of 4 cases and review of the literature. Neurosurgery 47(6): 542-551.
-
Alleyne CH, Bakay RAE, Costigan D, Thomas B, Joseph GJ (1996) Intracranial adenoid cystic carcinoma: case report and reviewof the literature. Surg Neurol 45(6): 265-271.
-
Garden AS, Weber RS, Morrison WH, Ang KK, Peters LJ (1995) The influence of positivemargins and nerve invasion in adenoid cystic carcinoma of the head and neck treated with surgery and radiation. Int J Radiat Oncol Biol Phys 32(3): 619-626.
-
Perez D, Alves FA, Nishimoto I, Almeida OP, Kowalski LP (2006) Prognostic factors in head and neck adenoid cystic carcinoma. Oral Oncology 42(2): 139-146.
-
Tannock IF, Sutherland DJ (1980) Chemotherapy for adenocystic carcinoma. Cancer 46(3): 452-454.
-
Chang CH, Liao YL, Hong HS (2003) Cutaneous metastasis from adenoid cystic carcinoma of the parotid gland. Dermatol Surg 29(7): 775-779.
-
Paris J, Coulet O, Facon F, Christian MA, Giovanni A, et al. (2004) Primary cancer of the parotid: clinicopathological approachPrimary cancer of the parotid gland: an approach anatomoclinical. Journal of Stomatology and Maxillofacial Surgery 105(6): 309-315.
-
Prokopakis EP, Snyderman CH, Hanna EY, Carrau RL, Johnson JT, et al. (1999) Risk Factors for local recurrence of adenoid cystic carcinoma: The role of postoperative radiation therapy. Am J Otolaryngol 20(5): 281-286.
-
Gurney TA, Eisele DW, Weinberg V, Shin E, Lee N (2005) Adenoid Cystic carcinoma of the major salivary glands treated with surgery and radiation. Laryngoscope 115(7): 1278-1282.
-
Vernat SS, Tochet F (2016) Radiotherapy of carcinoma of the salivary glands. Cancer Radiother 20: 136-138.
-
Kawamata T, Harashima S, Kubo O, Hori T (2006) Intrasellar remote metastasis from adenoid cystic carcinoma of parotid gland: case report. Endocr J 53(5): 659-663.
-
Pfeffer MR, Talmi Y, Catane R, Symon Z, Yosepovitch A, et al. (2007) A phase II study of Imatinib for advanced adenoid cystic carcinoma of head and neck salivary glands. Oral Oncol 43(1): 33-36.
-
(2014) Bondue Clémence Chu-Amiens Dr Fourquet, Salivary Gland Tumors.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO