Study of Radiation Doses during Cerebral, Thoracic and Abdominal-Pelvic Ct Scans in Adults at the Teaching University Hospital of Cotonou (Cnhu-Hkm)
Introduction: Knowledge of CT scan dose delivery is a legal obligation and an imperative of good practice. In Africa, radiation protection is a concern due to the non-compliance with established laws and regulations. The objective of this study was to study the radiation doses emitted by cerebral, thoracic and abdominal-pelvic computed tomography at the CNHU-HKM in Cotonou. Methods: This was a cross-sectional descriptive study with prospective collection. It took place from August 2019 to January 2020, over a period of six (06) months. An exhaustive census of scans exploring the skull, and/or trunk was made. The variables studied were the clinical data, the status of the examination prescriber, the type of examination and the dosimetric data of the examinations. Results: During our study period, 2788 CT scans were performed, 1150 were retained including 1046 (91.0%) in adults. CT scans were performed in overweight patients (38.6%). The majority of the performed exams were justified regardless of floor explored. The 75th percentile values of CTDI and LDP were not compliant in 59.7% and 58.4% of cases, respectively. The average effective dose for a brain scan is 3.2 mSv. Doses variation was observed according to body mass index. Conclusion: At the end of this study, the majority of the exams carried out were justified. The 75th percentile values of the dosimetric indices (CTDI, LDP) were higher than the diagnostic reference levels established by the Nuclear Safety Authority in 2019.
Introduction
During the last decades, the medical sector has experienced a rapid growth in the use of ionizing radiation for better diagnosis and treatment [1]. The demand for radiological examinations is growing, with particular reference to computed tomography scan, which alone accounts for about 50% of the overall medical exposure to ionizing radiation [2], but this diagnostic radiology technique poses a risk to human health due to the ionizing radiation it uses [3]. Radiation protection consists in protecting oneself by justifying exposures, optimizing and limiting doses [2]. Thus, the general principle of ALARA (As Low as Reasonably Available) radiation protection applied to patients and handling personnel makes it possible to reduce radiation exposures while being effective [4]. Knowledge of the doses delivered during CT scans is a legal obligation and an absolute imperative of good practice [5]. Despite the initiatives taken by several international organizations, the radiation protection situation in the majority of African countries is alarming due to the non-compliance with laws, regulations and radiation protection organizations. The International Atomic Energy Agency (IAEA) is initiating several training workshops for users, managers and regulatory authorities in the field of ionizing radiation use. However, the impact of these trainings on the patients management of radiation protection (RP) remains limited [6, 7].
In Benin, under the law n° 2017-29 of March 15, 2018 on radiological safety and nuclear security in the Republic of Benin, a regulatory authority for practices and activities using ionizing radiation has been created [8]. Knowing and controlling the radiation exposure generated by our machines is the essential prerequisite to ensure efficient radiation protection for our patients. On each scanner model, the user has indicators for estimating the dose delivered. He can modify the parameters to which he has access; to adapt this exposure to the information requested [5]. To date, no study on radiation doses delivered to patients by CT scan has been conducted in Benin, so it was appropriate to review the exposure doses to which patients and medical personnel are exposed. The present study aims at studying the radiation doses emitted by brain, thoracic and abdominal-pelvic CT scans in adult patients at the CNHU-HKM in Cotonou, Benin.
Materials and Methods
This was a cross-sectional descriptive study with prospective collection, which took place over 6 months, from August 2019 to January 2020 in the scanning department of the CNHU-HKM. It covered all CT scans performed without and or with injection of iodinated contrast material, exploring the skull and or trunk, in all adult patients (over 18 years old). All examinations were performed on a Siemens SOMATOM EMOTION® 16-slice scanner, which was commissioned in December 2013. At the end of each examination, data were collected on a survey sheet based on examination prescription forms and dose reports, with two (02) types of variables:
- Qualitative: gender, indication of the examination, prescriber status, anatomical region (s) explored during each examination, justification of the examination based on the 2013 edition of the French Society of Radiology’s guide for the proper use of medical imaging exams and the injection of iodinated contrast material.
- Quantitative: age, body mass index (BMI), data collected on dose report: the number of acquisitions for each examination performed, the voltage at the terminals of the generator in kilovolts (kV), the charge expressed in milliamps (mA), the thickness of the slices in millimeters (mm), the pitch, the Computed Tomography Dose Index (CTDI) in milligrays (mGy), the Dose Length Product (DLP) in milligrays centimetre (mGy.cm). The cumulative dose length product (cumulative DLP), expressed in mGy.cm, derived from the summation of the DLP of all the acquisitions obtained during each examination (collected directly on the scanner console at the end of each examination). The effective dose (E), in millisieverts (mSv), was obtained and calculated for each examination by factoring the DLP (mGy.cm) by conversion factors defined according to age and the anatomical region explored. These different factors are presented in the following Table 1.
| 0 year old | 1 year old | 5 years old | 10 years old | 15 years old | Adult | |
|---|---|---|---|---|---|---|
| Skull | 0.009 | 0.006 | 0.004 | 0.003 | 0.002 | 0.002 |
| Thorax | 0.099 | 0.064 | 0.047 | 0.033 | 0.024 | 0.021 |
| AP | 0.092 | 0.06 | 0.043 | 0.028 | 0.022 | 0.018 |
| TAP | 0.086 | 0.056 | 0.041 | 0.028 | 0.021 | 0.018 |
Table 1: ICRP Reference Conversion Factors by Type of Examination according to age.
Data entry was done in Epi Data Entry software version 3.5.1. The data analysis was done using R software version 3.6.2. Proportions (numbers and percentages) were used to describe the qualitative variables (age, sex, clinical indications of the different examinations), then central tendency and dispersion parameters (average, standard deviation, and 75th percentiles) were used to describe the quantitative variables (weight, height, body mass index, CTDI, length dose product, effective dose).
Student’s t-test and the ANOVA test were used to compare the different parameters. The significance threshold of the statistical tests was set at 5%. The average, the 75th percentile, and the standard deviation of the dosimetric indices per acquisition and for a complete act were calculated and compared to the recommendations set by the French Nuclear Safety Authority (NSA). The comparison of the average values of CTDI and LDP according to the physical condition of each patient was performed. The comparison of the values of the examinations performed with or without injection of iodinated contrast material was also performed, using the Student t-test and ANOVA.
Results
During the study period, 2788 CT scans were performed, out of which 1150 were retained with 1046 (91.0%) in adults. The epidemiological data are presented in Table 2.
| Exams | (N) | (%) |
|---|---|---|
| Skull | 608 | 58.13 |
| Thorax | 38 | 3.63 |
| TA | 104 | 9.94 |
| AP | 141 | 13.48 |
| TAP | 155 | 14.82 |
| Total | 1046 | 100 |
Table 2: Distribution of examinations according to the stage explored
AT: angioscanner-thoracic; AP: abdomino-pelvic; TAP: thoraco-abdomino-pelvic Cranio-encephalic scans were mostly performed. Table 2: Distribution of examinations according to the stage explored
Socio-Demographic Characteristics
The average age was 53.7+/-16.5 years old [19-96 years old] with male gender predominance (sex ratio of 1.02). Distribution of examinations according to physical conditions (BMI of patients). The distribution of examinations according to the physical condition of each patient and the stage explored is illustrated in Figures 1 & 2.
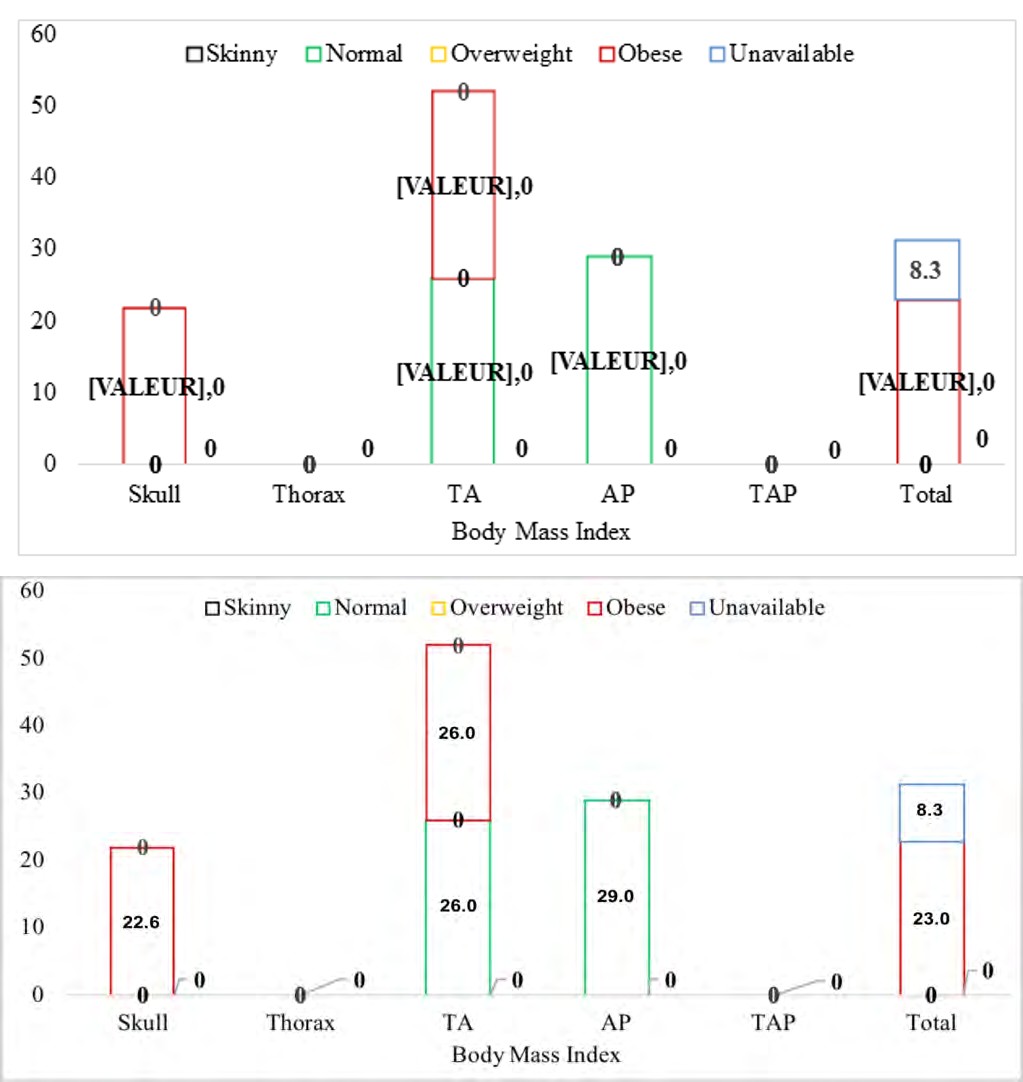
Figures 1 & 2: Distribution of examinations according to body mass index (BMI) and the stage explored.
Irrespective of the type of examination, CT scans were performed more often in overweight patients (404 accounting for 38.6%).
Justification of prescriptions
Clinical Indications: The clinical indications of the various examinations are set in Table 3 below.
| Indications | (N) | (%) |
|---|---|---|
| Brain scans | ||
| Injury from a stroke | 439 | 72.2 |
| Traumatic brain injury | 120 | 19.7 |
| Generalized convulsive crisis | 30 | 5 |
| Extension assessment of a primary neoplasia | 13 | 2.1 |
| Confusional syndrom | 6 | 1 |
| CT angiography | ||
| Suspected pulmonary embolism | 87 | 83.7 |
| Hypoxic syndrom | 13 | 12.5 |
| Hemoptysis | 4 | 3.8 |
| Abdomino-pelvic Scanners | ||
| Characterization of abdominal mass | 57 | 40.4 |
| Extension assessement of a primary tumor | 51 | 36.1 |
| Search for primary lesions | 21 | 14.9 |
| Colic renephritis | 12 | 8.6 |
Table 3: Distribution of examinations performed according to the clinical indications.
The majority of TAP scans were performed as part of a primary tumor extension assessment (128 accounting for 81.9%), followed by the search for primary lesions (28 accounting for 18.1%).
Prescriber Status: Figures 3 & 4 describes the distribution of examinations according to the status of the prescriber and the stage explored.
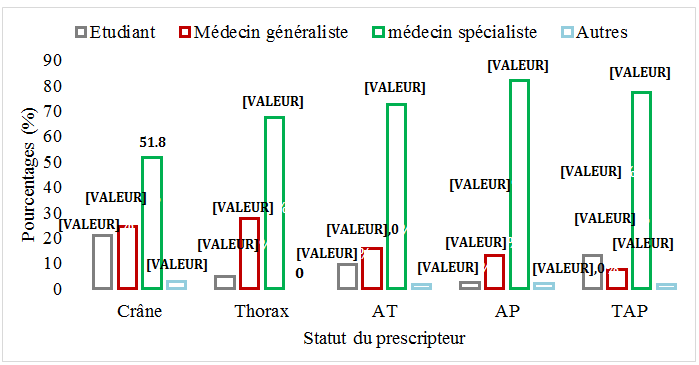
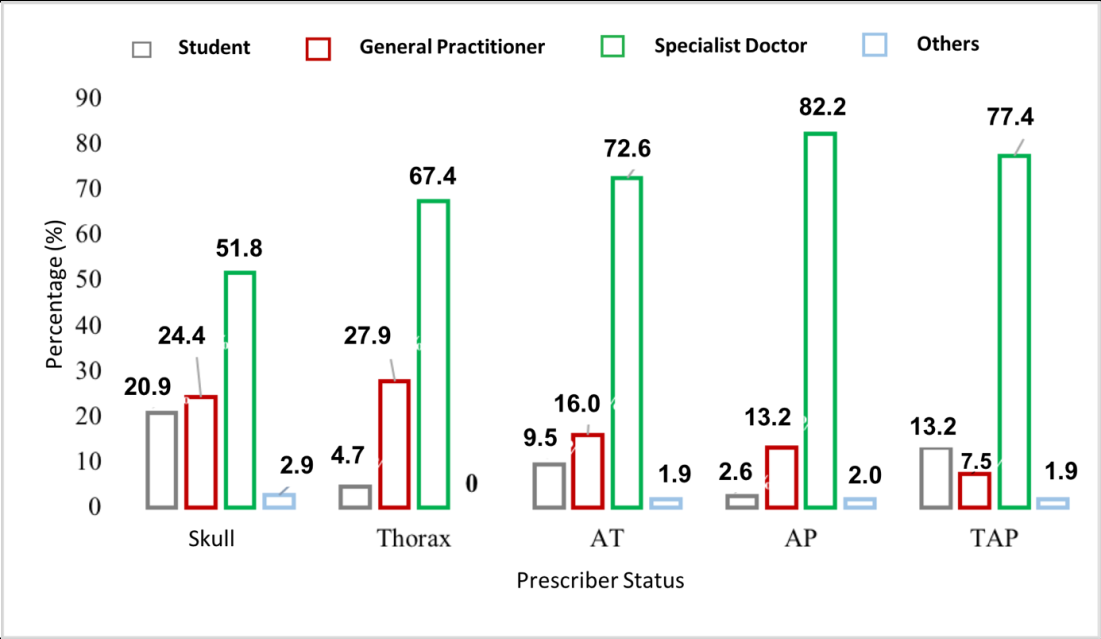
Figures 3 & 4: Distribution of examinations by prescriber status according to the stages explored Almost all of the requests for examination were justified regardless of the stage being explored.
Dosimetric data
Dosimetric Index by Acquisition and For a Complete Act: The dosimetric data by acquisition and for a complete act according to the stage explored are presented in Table 4.
| Unit | Skull | Thorax | TA | AP | TAP | |
|---|---|---|---|---|---|---|
| Value of the 75th percentile of the CTDI and DLP | ||||||
| CTDI | (mGy) | 58.3 | 7.5 | 5.7 | 8.4 | 8.7 |
| DLP | (mGy.cm) | 1221.4 | 312 | 98.7 | 395.8 | 437.6 |
| Average and 75th percentile of the DLP | ||||||
| μ | 1606.3 | 276.3 | 301.8 | 1202.5 | 1530.1 | |
| Q 3 | 2114.9 | 354.3 | 303.2 | 1584.2 | 1775.2 | |
| Average and 75th percentile of the efficient dose (mSv) | ||||||
| μ | 3.2 | 5.6 | 6.3 | 22.2 | 27.5 | |
| Q 3 | 4.2 | 7.1 | 6.4 | 28.7 | 32 |
Table 4: The dosimetric data by acquisition and for a complete act according to the stage explored are presented in table 4.
CTDI: Computed Tomography Dose Index; DLP: Dose Length Product; μ: average DLP value; Q3: 75th percentile. Table 4: The dosimetric data by acquisition and for a complete act according to the stage explored are presented in table 4.
Dosimetric Evaluation
The 75th percentile values of the CTDI and DLP obtained were compared to diagnostic reference levels (DRLs). The proportions of examinations that did not comply with the recommendations are presented in the following table, according to the stage explored (Table 5).
| Index | Skull | Thorax | TAP | TA | AP | Total |
|---|---|---|---|---|---|---|
| CTDI (%) | 99.2 | 7.9 | 6.5 | 2.9 | - | 59.7 |
| DLP (%) | 97.9 | 21.1 | 0.6 | - | - | 58.4 |
Table 5: Assessment of noncomplying doses with Recommendations (>DRL) according to the stage explored.
Influencing Physical and Technical Factors
The average values of the dosimetric index according to the physical condition of each patient and the stage explored are presented in Table 6.
| Physical Condition | Skull | Thorax | TA | AP | TAP | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| CTDI | LDP | CTDI | LDP | CTDI | LDP | CTDI | LDP | CTDI | LDP | |
| S | 57.6 | 1065 | 3.6 | 139.1 | 5.8 | 93.2 | 4.7 | 210.5 | 8.4 | 426.2 |
| N | 57.6 | 1155.5 | 4.8 | 203.1 | 5.4 | 97.6 | 6.1 | 283.1 | 7.4 | 309.5 |
| O | 58 | 1140 | 4.9 | 195 | 5.7 | 90.1 | 72 | 339.1 | 6.8 | 343.8 |
| Ob | 58.3 | 1152.7 | 7.2 | 300 | 5.5 | 90.3 | 8.6 | 413.4 | 8.6 | 500.2 |
| P value | 6.10-1 | 3.10-1 | 8.10-3 | 2.102 | 9.10-1 | 4.101 | 6.10-5 | 5.10-6 | 5.10-5 | 2.10-3 |
Table 6: Averages of CTDI and DLP by physical condition and the stage explored.
S: Skinny; N: normal; O: overweight; Ob: obese. Table 6: Averages of CTDI and DLP by physical condition and the stage explored.
The average values of the CTDI and DLP for brain scans performed without injection of iodinated contrast material (56.9 and 1086.2 respectively) and with injection of iodinated contrast material (58.3 and 1167.6) showed no statistically significant association (P value 3.10-4 and 2.10-4).
Discussion
Characteristics of the Population
Our study was conducted in the medical imaging department of the renowned hospital of Benin. The CT scan activity was preponderant compared to the three CT scan units active throughout the country during the study period. Ideally, a much larger number of CT units would have been included [9]. Despite the existence of a law governing radiation protection and a national radiation protection agency, the absence of a regulatory framework for patient protection justifies the use of SFR (French Radiological Society) reference systems. Although the IAEA’s efforts bear fruit with the creation of a radiation protection agency, the scarcity of resources means that the international conventions that are necessary in the absence of a national framework must be implemented [7].
The usefulness of computed tomography scan in the medical management of patients of all ages is undeniable. Its use continues to grow despite its highly irradiating nature, thus posing a radiation protection problem. The sample of our study was made up of the CT scans performed on adults at the CNHU-HKM of Cotonou, with a total of 1046 out of the 1150 accounting for 91.0%. This could be explained by the increasing availability and accessibility of CT scan in our country.
A predominance of cranio-encephalic CT scans was noted with 58.2% of examinations performed. In the literature, most of the CT studies performed in adults were carried out over a period of more than five (05) years, and/ or only one anatomical stage was explored, unlike in ours. However, Konrad HS, et al. [10] reported that the modalities frequently performed in his study were abdomino-pelvic scans, followed by cerebral and thoracic scans.
The average age in our study was 53.7+/-16.5 years old [19-96 years old], which is higher than the one reported by Konrad HS, et al. [10] in the USA in 2019 (44 years old) and Paul NZ, et al. [9] (45.95 and 44.99 years old) obtained from two different centers in Côte d’Ivoire in 2015. This would be explained by the fact that the examinations are often performed in active subjects. Male dominance was observed with a sex ratio of 1.02, contrary to Paul NZ, et al. [9] in Côte d’Ivoire in 2017 and Konrad HS, et al. in the United States in 2019 [11], who reported female dominance with sex ratios of 0.98 and 0.93, respectively.
Distribution and Justification of CT Scans Performed.
In our study, 38.6% of the scans were performed in overweight patients, followed by 23.0% in obese subjects. In the Konrad HS, et al. study [10], 35.1% of patients were overweight and 35.9% were obese. Search for stroke lesions (72.2%) and suspicion of a pulmonary embolism (52.6%) were the main indications for brain and chest scans respectively. The characterization of an abdominal mass (40.4%) and the extension assessment of a primary tumor (81.9%) were more frequent for abdomino-pelvic and thoraco-abdomino-pelvic CT scans, respectively. Konrad HS, et al. [10] found that in adults, the majority of patients had the extension of a malignant tumour (18.3%), followed by abdominal pain (17.2%). In fact, abdomino-pelvic scans and TAP scans accounted for most of the examinations performed in his study. Specialist physicians were the greatest prescribers in our study with 51.8% of brain scans and 72.6% of thoracic angioscans, so almost all of the examinations performed were well justified.
Dosimetric Data
The 75th percentile CTDI values by acquisition for cranio-encephalic examinations were 58.3 mGy and 1221.4 mGy.cm for DLP. Our values superimposed with those in the literature, mainly Paul NZ, et al. [9] who reported 75th percentile values of CTDI and DLP on cranio-encephalic CT for one acquisition, being 63.6 mGy and 1144.8 mGy.cm on HMA. In contrast, Garba I, et al. [11] found 77 mGy and 985 mGy.cm, respectively. All these values were higher than those used in Western countries for the comparison, thus confirming the non-compliance with the CT scans performed. The doses were higher than those established in the Irish survey of Foley SJ, et al. [12] in 2010 and comparable to those of Treier [13] in Switzerland in 2010 and Palorini F, et al. in Italy in 2013 [14]. Qurashi AA, et al. [15] reported in his study in Saudi Arabia in 2014 that the 75th percentile of the CTDI and DLP in his study was 18 mGy and 630 mGy. cm for thoracic CT scans, 18 mGy and 480 mGy.cm for angio thoracic CT scans, 15 mGy and 800 mGy.cm for abdomino-pelvic CT scans, and 16 mGy and 1040 mGy.cm for thoraco-abdomino- pelvic CT scans. These values were higher than those of our study. The increased doses could be due to differences in the design of CT scan radiation dose protocols and guidelines, as well as lack of awareness among radiologists and handlers.
In our study, regardless of the stage explored, the average value of the DLP for a complete examination was lower than those found in the literature. Indeed, the values obtained by Paul NZ, et al. [9] in their study were respectively 1968 and 2257.8 mGy.cm. They were close to those reported by Bindman RS, et al. [16] in the United States in 2015 (2130 mGy.cm) and Palorini F, et al. [14] (1233 mGy.cm). Our results suggest that the increase in the number of phases of the different types of tests is the main factor affecting the total dose delivered to the patient.
The average effective dose for a full procedure in our study for the brain scan was 3.2 mSv. However, the values obtained in adults for a cranio-encephalic examination in the Paul NZ, et al. study [9] were 4.13 and 4.74 mSv respectively. These values are higher than ours. The 75th percentile of the same parameter in our study was 4.2 mSv for cranio- encephalic CT scan, 7.1 for thoracic CT scan, 6.4 for thoracic angio scan, 28.7 for abdomino-pelvic CT and 27.5 mSv for thoraco-abdomino-pelvic CTscan, respectively. On the other hand, Bindman RS, et al. [16] found significantly higher values than in ours, with 8, 29, 32, and 43 mSv for brain, thoracic, abdominal-pelvic and thoraco-abdominal-pelvic scans, respectively. This difference could be explained, on the one hand, by the duration of the study and, on the other hand, by the number of examinations which was higher in his study.
Influencing Factors
A variation in doses is observed when comparing dosimetric index values as a function of body mass index, making it possible to hypothesize that the physical condition of each individual is a factor influencing radiation exposure doses. Konrad HS, et al. [10] concurs, reporting in their study that overweight and obese patients (69.6%) received significantly higher doses. The injection of iodinated contrast material during a CT scan would also be a factor of variation in radiation doses as reported by Kostas P, et al. [17] in his in 2017. However Aschoff AJ, et al. [18] in 2017 reported the important role played by iodinated contrast material in reducing radiation doses.
Conclusion
At the end of this work, it appears that the majority of the examinations carried out were justified. The values of the 75th percentile of the dosimetric index (CTDI, DLP) were higher than the diagnostic reference levels established by the Nuclear Safety Authority, and other factors such as body mass index and injection of iodinated contrast material were noted as factors of variation in radiation doses.
References
-
Coeytaux K, Bey E, Christensen D, Glassman ES, Murdock B, et al. (2015) Reported radiation overexposure accidents worldwide, 1980-2013: A systematic review. PLoS One 10(3): 0118709.
-
Paolicchi F, Miniati F, Bastiani L, Faggioni L, Ciaramella A, et al. (2016) Assessment of radiation protection awareness and knowledge about radiological examination doses among Italian radiographers. Insights Imaging 7(2): 233-242.
-
Cordoliani YS, Boyer B (2004) Chapter XI: Doses delivered to the patient in computed tomography (scanner). Radiol leaf 44(2): 139-145.
-
Aubert B, Lefaure C (1998) Can we optimize the radiation protection of workers in the medical field?. J Radiol 79: 307-312.
-
Coradin D (2016) The main principles of radiation protection. The Rev the Nurse 65 (220): 49-50.
-
(2016) Summaries of the JRANF 2016 conferences: conferences 16 & 17. JAIM 8(2): 46-56.
-
Zogo PO, Mokubangele CM, Moifo B, Fotsin JG (2012) Patient dose assessment in pediatric computed tomography in two university hospitals in Yaoundé Cameroon. Radioprotection 47(4): 533-542.
-
Law n° 2017-29 of March 15, 2018 on radiological safety and nuclear security in the Republic of Benin.
-
Paul NZ, Judicael AN, Ali C, Eric S, Patricia CC, et al. (2017) Comparison of doses delivered to patients during cranio- encephalic computed tomography scans in two imaging centers in Abidjan. 9(4): 165-168.
-
Konrad HS, Cerhan JR (2019) Cumulative Doses of Ionizing Radiation from Computed Tomography: A Population-Based Study. Mayo Clin Proc 94(10): 2011- 2021.
-
Garba I, Engel Hills P, Davidson F, Tabari AM (2015) Computed tomography dose index for head CT in northern Nigeria. Radiat Prot Dosimetry 165(1-4): 98- 101.
-
Foley SJ, Mcentee MF, Rainford LA (2012) Establishment of CT diagnostic reference levels in Ireland. Br J Radiol 85(1018): 1390-1397.
-
Treier R, Aroua A, Verdun FR, Samara E, Stuessi A, et al. (2010) Patient doses in CT examinations in Switzerland: Implementation of national diagnostic reference levels. Radiat Prot Dosimetry 142(2-4): 244-254.
-
Palorini F, Origgi D, Granata C, Matranga D, Salerno S (2014) Adult exposures from MDCT including multiphase studies: First Italian nationwide survey. Eur Radiol 24(2): 469-483.
-
Qurashi AA, Rainford LA, Foley SJ (2015) Establishment of diagnostic reference levels for CT trunk examinations in the western region of Saudi Arabia. Radiat Prot Dosimetry 167(4): 569-575.
-
Bindman RS, Moghadassi M, Wilson N, Nelson TR, Boone JM, et al. (2015) Radiation doses in consecutive CT examinations from five university of California medical centers. Radiology 277(1): 134-141.
-
Kostas P, Tzedakis A, Spanakis K, Papadakis AE, Hatzidakis A, et al. (2018) The effect of iodine uptake on radiation dose absorbed by patient tissues in contrast enhanced CT imaging: Implications for CT dosimetry. Eur Radiol 28(1): 151-158.
-
Aschoff AJ, Catalano C, Kirchin MA, Krix M, Albrecht T (2017) Low radiation dose in computed tomography: The role of iodine. Br J Radiol 90(1076): 20170079.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO