The Presentation of Clinical Results of Radiolabelling of 99mtc- MIBI Complex Using Ultrasound Technique for Myocardial Perfusion Scanning (MPS)
The initial objective and opinion of this study is introducing the clinical results of the 99mTc-MIBI complex radiolabelling utilizing ultrasound method as an approach for labeling MIBI kits with 99mTc instead of applying a boiling water bath as a usual and standard method. The results provided in this research applying radio-HPLC and ITLC, indicate that radio-labeling of MIBI vial with 99mTc can be provided with high effectiveness and appropriate acceptance applying ultrasound method as a novel approach. The imaging research applying SPECT indicated that the 99mTc-MIBI complex samples that were made ready applying ultrasound irradiation approach indicate very similar biodistribution in the heart, thyroid, lung, liver, gallbladder, kidneys, stomach, GI and bladder of the volunteer patients. Non-habitual aggregation of 99mTc-MIBI samples were not observed in our approach. This research indicated that sonication approach can be proposed for providing 99mTc-MIBI radiocomplex samples. The reaction time to provide radio-complex can be considerably decreased compared to the boiling water bath approach. This main development may decrease potential risk to the patient to inhibit any delay in emergency situations like acute therapy, especially for myocardial infarction patients in clinical practice.
Background
Myocardial perfusion single-photon emission computed tomography (MPS) is one of the most significant and usually handled non-invasive cardiac imaging tests. MPS has a significant role in diagnosing cardiovascular disease, establishing prognosis, evaluating the efficiency of therapy, and evaluating myocardial viability. The success of this imaging modality has, in large section, been regarding developed technology which continues to advance and develop the field. These involve the progressive advancement of single-photon emission-computed tomography (SPECT) technologies, novel radiopharmaceuticals, and novel software [1]. Thalium-201 (in the early 1970s and kept in usual utilization until the mid-1980s) and technetium-99m (99mTC) sestamibi and tetrofosmin are commonly applied radiopharmaceuticals [2]. 99mTc-labeled radiopharmaceuticals were improved and, for the most section, replaced thallium to assess the myocardial perfusion abnormalities [3]. Technetium, the 43rd element in the periodic table, belongs to the group of transient metals. Owing to its electron configuration of 4d5 5s2, technetium prepares a handful of situations for complex formation with many different ligands, and its oxidation state (OS) can alter from +1 up to +7. OS is regarded to be a major parameter identifying the chemical feature of complexes. Technetium can form chemical bonds including both sigma and pi electrons, and the sigma bonds can be the colligative and coordinative kinds when spin compensation and electron pair donation take place, respectively. Moreover, the structure of technetium complexes can be signified by the coordination number (N), which can change from 4 to 7, permitting tetrahedral (N=4), tetragonal pyramidal (N=5), octahedral (N=6), capped octahedral (N=7) or pentagonal bipyramidal (N=7) geometry. The third parameter for characterization of technetium complexes is the electric charge (Z) of the whole molecule that might prepare an anionic (Z=–1), neutral (Z=0) or cationic (Z=+1) character [4]. (201)Thallium (TL), (99m) Tc-tetrofosmin (TF), and 99mTc- MIBI is widely applied as myocardial perfusion agents [5]. A handful of technetium 99m-labeled myocardial perfusion agents were under survey to identify their utility in evaluating regional myocardial blood flow and cellular viability in recent years.
Technetium 99m-2-methoxyisobutyl isonitrile (99mTc- MIBI), one of the most significant agents is a lipophilic cation largely sequestered in the mitochondria by the large negative transmembrane potential. Experimental research indicated that 99mTc-MIBI complex is taken up in the myocardium in proportion to blood flow, but as other diffusible radionuclides underestimates flow at high flow rates. The research revealed that this agent uptake after reperfusion, preceded by changing coronary occlusion periods, reflects the degree of myocardial salvage and viability. Research indicated that this complex has good features to handle myocardial perfusion scans [6, 7, 8, 9, 10]. In the last decade, 99mTc-labelled lipophilic cations emerged as appropriate tools to trace specific cellular processes and functions in various malignant tumors, involving breast cancer. Among these agents, the 99mTc- MIBI complex is the most highly assessed tracer and might serve as a paradigm for this class compound class [11]. 99mTc- Sestamibi moreover is applied in Parathyroid Scintigraphy for the Detection and Localization of Parathyroid Adenomas in Patients with Hyperparathyroidism [12] which indicated to be suitable to diagnose lung cancer [13].
Reagents of kit for 99mTc-MIBI complex are as follows: [Tetrakis (2-methoxy-2-methylpropyl-1-isocyanide) copper (1+)] tetrafluoroborate (MIBI); which facilitates labeling by ligand exchange at elevated temperature, Stannous chloride dihydrate: SnCl2.2H2O; which is used as a reducing agent, L-cysteine hydrochloride monohydrate, Sodium citrate dihydrate, D-mannitol, Hydrochloric acid (concentrated, 1N, 0.2N), Sodium hydroxide: NaOH (1N), Water for injection and nitrogen gas. The chemical compositions of the kits are included into: MIBI: 1.0 mg, Stannous chloride dihydrate: 0.075 mg, L-cysteine hydrochloride monohydrate: 1.0 mg, Sodium citrate dihydrate: 2.6 mg and D-mannitol: 20 mg. The labeling features are as follows: MIBI: 0.2 mg/mL, L-cysteine hydrochloride: 0.2 mg, Sodium citrate: 0.52 mg/mL, D-mannitol: 4.0 mg/mL, pH: 5.0-6.0, Radiochemical purity: >90%, free pertechnetate (TcO4–):<5%, 99mTc reduced/ hydrolysed: <5%. Providing MIBI kit utilizing sodium pertechnetate (Na+ 99mTcO4−) was performed due to the instructions provided by producer. The lyophilized products were provided applying the fresh Na+-99mTcO4- solution (740–3700 MBq =20–100 mCi)) from generators eluted in sterile conditions. In 99Mo/99mTc generators, regarding the imperfections in producing the generator or possible occurrence of mechanical defects, 99Mo may leak from the generator due to the elution process [14, 15, 16]. To resolve the contents of vial, the protected vial should be strenuously shaken due to safety conditions. Then, the vials were heated on a boiling water bath for 10 minutes.
After heating, the vial is placed into the lead shield and cooled at room temperature for approximately 15 min [17]. This complex can be applied within 6 h after preparation. The 99mTc-MIBI kit has the +1 charge. The labeling time of MIBI kit with technetium is prolonged applying common and usual approaches like boiling water bath. One of the approaches introduced to replace boiling water bath technique for labeling the MIBI kit with technetium is the microwave oven heating technique. A study indicates that the microwave oven heating approach prepares a reproducible heating technique for labeling 99mTc-sestamibi. By a labeling efficiency over 96.4% after 13 sec of heating, this method simplified and shortened the work included in providing 99mTc- MIBI complex. It is reliable and well suited for emergency conditions when the agent requires being available almost immediately [15].
The microwave heating method has technical precautions which should be regarded in applying this approach to provide 99mTc-MIBI complex. Despite, the benefits of this approach, these precautions are regarded disadvantages for this approach. These precautions involve the optimum heating time and wattage for the successful labeling of 99mTc-MIBI with a particular microwave oven, which must be experimentally identified, the metal cap of the vial requires to be covered with Styrofoam to avoid electrical sparking and a vacuum situation should be obtained before the labeled vial is heated with a microwave oven, any residual gas left in the head space of vial could cause an ejection of the rubber stopper due to the excess steam pressure built up the vial [17]. Despite above factors, the labeled vial should always be heated in the same position inside the microwave oven, microwave ovens with digital control panel are more suitable for setting short heating time (i.e. 10s) since they can be correctly set at the needed heating period and the loss or variation of microwave power output and frequency related to extended the utilization of the microwave oven must be assessed on a long-term basis and finally any technical error in setting the microwave heating time below or beyond the predetermined time which may result in the 99mTc-MIBI solution being rendered unsuitable for clinical utilization [18].
Due to mentioned factors, this approach is not customarily actually applied in nuclear medicine. In the early 1990’s, Green chemistry is defined as the use of a set of principles which decreases or deletes the utilization of hazardous substances in the design, manufacture and application of chemical products [19]. One of the methods mentioned as the green value in chemical reactions is ultrasound irradiation [20]. Comparing to traditional approaches, ultrasound irradiation is more comfortable and simply monitored. Many chemical reactions were done in higher yield, shorter reaction time, and milder condition under ultrasound irradiation [21]. Doroudi A, et al. explained labelining of MIBI kits with 99mTc applying ultrasound irradiation approach [17]. Regarding the study, (37MBq) 99mTc-MIBI complex samples were provided utilizing ultrasound irradiation technique or boiled water bath approach as a standard method. Qualitative and quantitative research was done.
The accumulation of 99mTc-MIBI complexes provided by two above noted modalities were approximately 3 ±0.1 % in the rats’ heart. The ultrasound irradiation technique is proposed to provide 99mTc-MIBI complex in effectively value [17]. The initial objective and opinion of this study is the presentation of clinical results of radiolabelling of 99mTc- MIBI complex applying ultrasound technique as an approach for labeling MIBI kits with 99mTc instead of utilizing a boiling water bath as a common and standard method and indication of bio-distribution of 99mTc-MIBI complex samples which are labeled by ultrasound irradiation method compared to boiling water bath method in the human heart.
Methods
The whole chemical materials which are utilized in this research were purchased from Broker, Merck, and Sigma- Aldrich companies. The chemicals and solvents were among the highest purity or analytical grade and were applied without more purification. Radioisotope Division of AEOI provided the freeze-dried MIBI kits and 99Mo/99mTc generators. 99mTc as Na+ TcO4- is received by 99Mo/99mTc generator by using sodium chloride 0.9%. Providing 99mTc- MIBI complex samples were done by manufacturer’s instructions as a standard approach or by freshly advanced method. The whole materials utilized in this research were located in the appropriate environment and standard situations. 0.9% NaCl was applied to identify 99mTcO4–, and methanol, for identifying decreased 99mTc.
The whole reactions were controlled by analytical RP- HPLC on a JASCO 880-PU intelligent pump HPLC system (Tokyo, Japan) equipped to a multiwavelength detector and a flow-through Raytest-Gabi γ-ray detector. CC 250/4.6 Nucleosil 120-5 C-18 column from Teknokroma was applied for HPLC. All research utilizing 99mTc were done in laboratories confirmed for radioactivity utilization. Suitable shielding and radiation safety methods were investigated at each step by trained personnel. AEOI provided MIBI compound used for preparing lyophilized MIBI kits. MIBI kits were provided applying almost the same composition as that of Cardiolite (DuPont) kit. 19.5 mg of anhydrous SnCl2 was dissolved in 3.0 mL of 37% HCl to provide a solution designated as solution C. 10 mg of [Cu(MIBI)4]BF4 was dissolved with stirring in 8 mL of water. Furthermore, 10 mg of L-cysteine hydrochloride monohydrate, 25 mg of sodium citrate, and 220 mg of mannitol were added and dissolved with shaking. After purging with oxygen-free N2 for 15 min, 0.1 mL of solution C was added. The final solution was balanced to pH 5.4-5.9 with 1 M NaOH. The final volume was balanced to 10 mL with sterile water for injection (SWFI). 1-mL portions of the final solution were then dispensed through a 0.22-μm Millipore filter into 10-mL borosilicate vials.
The contents of vials were then lyophilized at 0°C for 30 h and kept in a vacuum. 99mTc as 99mTcO4– was provided from an in-house 99Mo/99mTc generator applying 0.9% NaCl. The commercial MIBI kits (AEOI, Tehran, Iran) were utilized. 20 MIBI kits were selected from various batches. The vials were randomly divided into two equal groups. 740 (For 10 patients), 1480 (For 4 patients), 2220 (For 2 patients), 2960 (For 2 patients), and 3700 MBq (For 2 patients) 20, 40, 60, 80, and 100 mCi of newly eluted 99mTcO4– in isotonic normal saline (Up to 2 cc) was added to MIBI vials, shielded vials were shaken for 30 s, and the mixture were heated on a boiling water bath for 10 min, due to manufacturer’s instructions as a standard approach or the vials were sonicated in Ultrasonic bath with a volume of 6 liters with heater and timer model E60H (Elma , Made in Germany) at 65°C for 1 min (as a new developed method).
Radiopharmaceutical analyses were done by ITLC and RP- HPLC. ITLC was done with Whatman no. 3 filter paper and two various solvent systems. Samples involving labeled MIBI (2 μL) were used at a distance of approximately 1 cm from the bottom of ITLC strips, were permitted to dry at room temperature, and were then located in air-tight containers. When applying 0.9% NaCl as the mobile section, 99mTc- MIBI complex and decreased 99mTc remained at the point of spotting, whereas free 99mTcO4- turned with the solvent front.
By HPLC-grade methanol as the mobile phase, 99mTc- MIBI complex and free 99mTcO4-turned with the solvent front, whereas decreased 99mTc kept at the point of spotting. The strips were cut to 1/4 and 3/4 pieces and counted for 2 min under a single-head camera equipped by a low-energy all-propose collimator applying an energy peak centered at 140 keV. The content of reduced 99mTc was identified as the percent ratio of the activity of lower 1/4 piece from the run with methanol to the total activity, and the content of free 99mTcO4- as the percent ratio of the activity of the upper 1/4 piece from the run with 0.9% NaCl to the total activity; the content of complex was identified from the difference. For radionuclide analysis of 99mTc-MIBI complex by HPLC, a 10 μL portion of the test solution was injected into C18 reversed-phase column; 0.1% trifluoroacetic acid/water (solvent A) and acetonitrile (solvent B) were applied as the mobile phase with the following gradient: 0 min, 95% A 95%-5% B; 5 min, 95% A-5% B; 25 min, 0% A-100% B; 30 min, 0% A, 100% B; flow rate 1 mL min-. Only 99mTc-MIBI and free 99mTcO4- are determined by RP-HPLC analysis.
The dose calibrator was controlled daily by estimating the activity of a standard source involving a long-lived radionuclide like 137Cs or 57Co. Among the patients who had referred to Golestan Hospital for myocardial perfusion scanning, the 20 of patients (8 men and 12 women; age range= 30-72, median= 52.45 years) were introduced to department of the nuclear medicine and molecular imaging of the hospital. These 20 patients did not have any liver disease or kidney failure. Every patient gave written consent after catching a full explanation of method and the objective of this research. Twenty patients were involved 8 men and 12 women (mean age=52.45 year and age range=30 to 72 year) participated in this method. These twenty volunteer patients were divided into two groups (every group consisting of ten people): group A (involving 3 men and 7 women with an age range of 36 to 67 years and a mean age of 51.7 years) and group B (involving 5 men and 5 women with an age range of 30 to 72 years and an average age of 50.3 years). Thallium-201, 99mTc-MIBI and 99mTc-tetrofosmin can be applied to handle perfusion imaging. Our objective in this research is the 99mTc-MIBI complex. 99mTc-MIBI complex samples provided by ultrasound method were injected into group A subjects intravenously and group B received 99mTc-MIBI vials provided by boiling water bath approach (intravenous injection). For a 1-day MPI protocol, the injected activity must be divided into either a third or a quarter for the first research and either two- thirds or three-quarters for the second one.
For a 2-day MPI protocol the injected actions are commonly at the similar level. In this research, myocardial perfusion-SPECT was handled utilizing a rest-stress protocol which is done two isolated days for all volunteer patients. Due to the mentioned protocol, on the first day (stress test), 740 to 1110 MBq of 99mTc-MIBI complex samples were intravenously injected for patients and on the second day (Rest Test), the same doses were injected in the similar way. Stress test in present research was done due to the situation of volunteer patients applying dipyridamole. Dipyridamole is a phosphodiesterase enzyme inhibitor. In indirect mode, it increases myocardial perfusion by preventing the degradation of cyclic adenosine monophosphate and with blocking the cellular reuptake of endogenous adenosine. At last, circulating adenosine concentration increases by 3- to 4-fold. Furthermore, Adenosine acts on a receptor that up- regulates producing cyclic adenosine monophosphate. Cyclic adenosine monophosphate relaxes vascular smooth muscle, inducing vasodilation and increasing myocardial perfusion by 3.8- to 7-fold.
Peak vasodilation after dipyridamole administration takes place on average 6.5 minutes after beginning the infusion. The hyperemic impact of dipyridamole can take for more than 50 minutes, with the half-life of dipyridamole being 30 to 45 minutes. The circulating adenosine might also act on the A, A and A receptors that has the potential to induce some complications explained more below. It is metabolized in the liver to the glucuronic acid conjugate and excreted in bile. Regarding proposed guidelines, patients were made not to eat anything for at least 3 hours before the stress test. Since methylxanthines are competitive preventers of adenosine receptors, the patients were avoid from using any product involving methylxanthines, involving caffeinated beverages or caffeinated foods (e.g coffee, tea, soft drinks, chocolate, etc.), Drugs involving caffeine, theobromine and theophylline for at least 12 hours before the stress test. The present protocol for a dipyridamole nuclear stress test was performed due to the standard guidelines 1. Blood pressure and 12-lead electrocardiogram controlling was done each minute via the stress test, up to 3 to 5 minutes after the test or when the patient is stable.
2. Dipyridamole was intravenously administered over 4 minutes at a standardized dose of 0.56 mg/kg.
3. The radioactive tracers were injected 3 to 5 minutes after the whole infusion of dipyridamole.
4. Single-photon emission calculated tomography was done from 15 to 45 minutes after inducing of dipyridamole- mediated stress, making images of blood flow via the patient’s heart.
5. Dipyridamole injection was not discontinued and aminophylline was not needed, because none of the patients had the following:
- Severe hypotension (systolic blood pressure of less than 80 mmHg)
- Symptomatic, persistent second-degree or complete heart block
- Other significant cardiac arrhythmia
- Wheezing,
- Severe chest pain associated to an ST depression or signs of poor blood perfusion (e.g., cold skin, pallor or cyanosis).
Next day, the rest test was done by the similar approach, except in the rest section, myocardial perfusion imaging was done 1 hour after handling 99mTc-MIBI complex samples. Every phase scans (stress and rest) were provided from one to two hours after the complex samples were injected into the patients. The patients were in a supine situation with the arms which was raised above the head and were supported for imaging applying a single-head gamma-camera with SPECT (ECAM scintron all Body, 2001, Siemens, USA). Comparing the rest and stress research was handled by the patient in the same situation in this research as a significant point. Moreover, the female patients were imaged without putting on bras. Moreover, we utilized a chest band for male patients to decrease movement.
Explanation of Image Acquisition in This Study
Gamma camera system: Myocardial perfusion imaging was done applying a single-head gamma camera. Low-energy, high-resolution (LEHR) collimators were applied, and in general, these kinds of collimators are recommended for 99mTc studies. Energy window for 99mTc was 20% at 140 keV.
Orbit: Scintigraphy imaging was provided on 180° rotation orbits applying a single-head gamma camera. Single-detector systems were utilized. In these systems, rotation from 45° right anterior oblique (RAO) to 45° left posterior oblique (LPO) was utilized. Pixel size is 6.4±0.4 mm for a 64×64 image matrix. Zoom was done as necessary for cameras with a large field of view (×1.5). This provides a good balance between image resolution and image noise. Since Non-circular orbits minimize the distance between the patient and the camera via the scan, we applied non-circular (elliptical) rotation.
Number of projections: Due to the 18° rotation, 64 views were applied.
Centre of rotation: Centre of rotation (COR) calibration was done due to the manufacturer’s recommendations. The validity of COR correction was periodically tested by estimating full-width at half-maximum (FWHM) spatial resolution from a 180° SPECT study of a point or line source of 99mTc . After reconstructing with a ramp filter, SPECT resolution was estimated. To quantify the spatial resolution reliably, a large matrix size and a zoom factor was used.
The Parameters Required to Provide Scans of the Heart Myocardial and the Whole Body
Myocardial imaging: matrix (64 × 64), zoom × 1.5 and energy window (140 keV), counterclockwise spin, angle start (45º), 100 kilo count in the first frame (first show with counting), rotation direction from RAO to LPO. Filter return design, butterworth filter (interruption frequency 0.4 cycles/ pixel and force 5). Rehabilitation scans were shown on short axis, vertical long axis and horizontal long axis. The general time needed was near 15 minutes.
The image of the whole body: The whole body scan was accessed near 1-2 hours after injection of the complex at a rate of 12 cm/min and a matrix size of 1024 25×256. To provide the image, a 20% the reception window was applied approximately 140 keV reaching the maximum of photo.
To explain and describe MIBI scans, two indices were applied at rest phase. The first index: By dividing the value of complex absorbed in the heart into its counts to whole body utilizing the software available in the nuclear medicine department of the hospital, the heart uptake to the whole body uptake was computed for every person. Hence, applying whole body scan, the region of interest (ROI) was made in all directions the heart uptake and next the latter ROI was designed around the whole body uptake in the anterior sight. The cumulation of 99mTc-MIBI complex in the cardiac to allover of total body was measured (Figure 1).
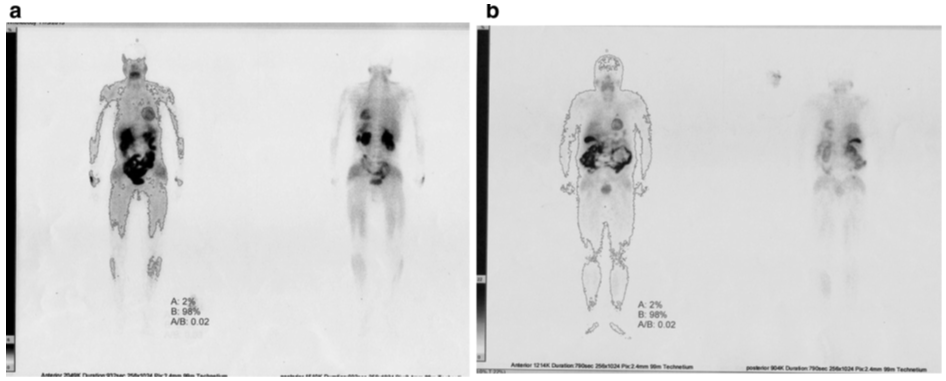
Figure 1: Entirety body radioisotope images patients were done the rest step after the 555-740 MBq (15-20 mCi) 99mTc-MIBI intravenously handled. Applying accessible commercial software, the accumulation proportion of radiotracer in the patient’s heart to complete body was calculated by isolating the action of heart to add up to body counts. 99mTc-MIBI uptakes within the heart to the whole body were roughly 2%. The 99mTc-MIBI complex tests were given here (a) ultrasound irradiation, (b) boiled water bath conditions.
No context deduction utilized. To understand and show the uptake of complex in the thyroid, lung, liver, gallbladder, stomach, colon, kidneys and bladder, visual scoring (0, *, , *) was used. Scores indicate equal absorption of the complex with the heart, scores * reveal greater absorption from the heart, scores * show less absorption from the heart, and finally 0 reveals no absorption (Table 1).
| Age | Gender | Group | Heart signal (%) | Bladder | Kidneys | Liver | Gallbladder | Stomach | Thyroid | Lung | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 46 | Female | A | 2 | *** | ** | ** | *** | 0 | 0 | 0 | |
| 47 | Female | A | 3 | ** | *** | ** | ** | 0 | * | 0 | |
| 46 | Female | A | 2 | *** | ** | * | *** | * | * | 0 | |
| 40 | Female | A | 1 | ** | *** | ** | *** | 0 | ** | 0 | |
| 36 | Female | A | 2 | *** | *** | ** | ** | 0 | ** | 0 | |
| 66 | Male | A | 2 | ** | ** | ** | *** | 0 | * | 0 | |
| 51 | Female | A | 3 | * | * | * | * | 0 | * | * | |
| 63 | Male | A | 2 | ** | *** | * | *** | 0 | 0 | * | |
| 67 | Female | A | 1 | *** | ** | * | *** | 0 | 0 | 0 | |
| 55 | Male | A | 4 | *** | *** | ** | * | 0 | 0 | * | |
| 47 | Female | B | 2 | *** | *** | * | *** | 0 | 0 | 0 | |
| 38 | Male | B | 3 | *** | *** | * | *** | 0 | * | * | |
| 72 | Male | B | 2 | *** | ** | * | *** | 0 | 0 | 0 | |
| 61 | Female | B | 1 | *** | *** | ** | *** | 0 | ** | 0 | |
| 65 | Male | B | 2 | *** | *** | *** | * | 0 | * | 0 | |
| 43 | Female | B | 2 | *** | *** | *** | * | 0 | * | * | |
| 54 | Male | B | 1 | *** | *** | ** | *** | 0 | 0 | 0 | |
| 65 | Female | B | 2 | *** | *** | *** | ** | 0 | ** | 0 | |
| 57 | Male | B | 2 | *** | *** | ** | *** | 0 | * | 0 | |
| 30 | Female | B | 2 | *** | *** | *** | * | 0 | ** | 0 |
Table 1: Patient specifications in both groups A and B were assessed in the rest phase after IV injection of 555-740 MBq (15-20 m
The scintigraphic scans were expounded by three experienced and independent Doctors of nuclear medicine, and the terminal point of views of all three of these doctors was the same. Watchers were uninformed of the making ready method of complex samples.
Results
99mTcO4 and decreased 99mTc are two major impurities made due to the labeling of MIBI kit with 99mTc. MIBI- 99mTc complex, 99mTcO4 and reduced 99mTc are simply determined and estimated quantitatively by exploration and analysis of instant thin layer chromatography (ITLC). The decreased 99mTc impurity cannot be diagnosed applying R-HPLC approach. ITLC analysis indicates that the average efficiency of 99mTc-MIBI complex samples that provided applying a boiling water bath as a conventional method was 94±1.8 % (n=20) and the mean efficiency of the labeled vials through the ultrasound approach as a proposed method was 92.5±3 % (n=20). Radio-HPLC analysis prepared from 99mTc-MIBI complex samples and 99mTcO_4^- Figure 2 indicated that the reactions were resulted in a single result and their retention times were provided to be 21.09 and 3.48 min for 99mTc-MIBI complex sample and 99mTcO_4^- respectively.
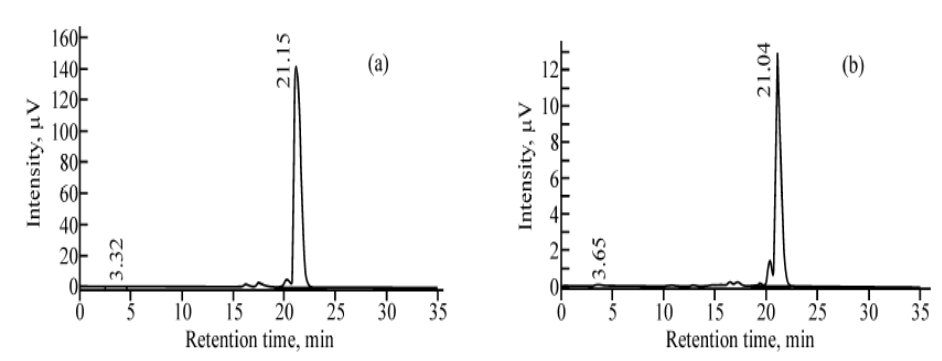
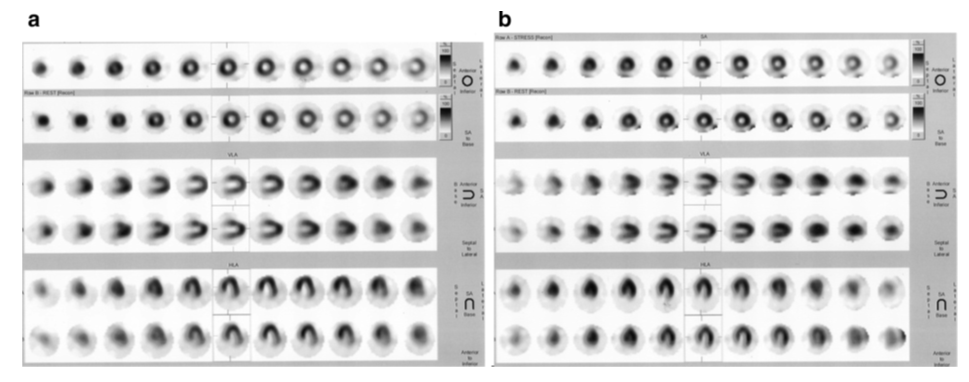
Figure 3: SPECT perfusion scans of the same patients were prepared with 99mTc-MIBI radiotracer tests. A 2-day stress/rest myocardial perfusion filtering convention was handled. The short-axis (beat 2 columns), vertical long-axis (center 2 lines) and even long-axis (foot 2 columns) cuts were revealed at push and rest. The images in to begin with push of brief pivot, vertical long pivot and flat long pivot have a place to the stretch stage of myocardial perfusion imaging. The camera rotation around the patient’s chest from 45°C right front angled (RAO) to 45°C cleared out back angled (LPO). The filters were given 1-2 h after the 555-740 MBq (15–20 mCi) 99mTc-sestamibi radiotracer tests organization intravenously, (a) radiopharmaceutical test arranged through sonication strategy, (b) 99mTc-MIBI complex test reconstituted by means of boiling water shower strategy.
These results and explanations indicate that the radio- labeling of 99mTc-MIBI complex samples applying the sonication irradiation approach is quite successful and high efficiency. For intravenous injection of 99mTc-MIBI complex samples to patients, the yield of 99mTc-MIBI complex samples must be more than 90%. All sick people who referred to Department of Nuclear Medicine of Hospital for myocardial perfusion scanning, had acceptable and favorable situations.
The patient volunteers were assessed for 2 months after investigation. During this time, none of the patients reported any side effects from injecting 99mTc-MIBI complex samples like nausea, vomiting, diarrhea, bronchospasm, hypotension, hypertension, tachycardia, bradycardia, fever, chills did not have muscle cramps and allergic reactions. The scans provided for every patient indicate a proper and considerable absorption of Tc-MIBI complex samples in the heart. The standard of scans was the same in both groups A and B. For these reasons, it was proven to us that myocardial perfusion scan investigations were done for patients in group A, as in the other group (Figure 3).
The imaging of total body at rest step, 1-2 hours after 99mTc-MIBI complex injection was intravenously done. The biodistribution of radio-tracer samples was handled to evaluate the distribution of 99mTc-MIBI complex samples in patient volunteers. The radiolabelling methods did not result in a significant difference in the model of biodistribution of complex samples. Outcome indicated that the technique of the reconstruction of radiotracer samples could not cause to make changes to the characteristics of radiotracer samples in bioanalysis research. The result of all research indicated that the features of all radiotracer samples which were prepared through ultrasound irradiation were completely alike to the features of 99mTc-MIBI complex samples were reconstituted through the boiling water bath technique. The accumulation of radiopharmaceuticals reconstituted through both sonication method and boiling water bath technique was almost 2% in the hearts of volunteers. The bio-distribution of radiopharmaceuticals in other body parts was same (Table 1). We did not observe any unanticipated impacts of radiopharmaceuticals on sick volunteers who gone for MPS to the nuclear medicine department of Hospital.
Discussion
To make the utilization of proper scanning specifications of 99mTc Hexakis (2-methoxyisobutyl isonitrile) Tc (I) (Tc- MIBI) is a MPS factor with lipophilic cationic characteristics made. 99mTc-sestamibi is a lipophilic set with a positive charge which is in complete clinical utilization [22]. A handful of elements influence the effectiveness of MIBI labeling with 99mTc radioisotope. They involve the formulation of MIBI kit and its framework, the period of 99mTc-MIBI complex heating, leakage of 99Mo and aluminum ions with the newly eluted 99mTcO4- solution from the 99Mo/99mTc generator, and the ratio of 99Tc to 99mTc. Since 99mTcO4 present in the elution solution cannot straightly react with MIBI to make desirable 99mTc-MIBI complex, a decreasing agent like SnCl2 is involved in the formulation of radiopharmaceutical kits. The ligand must be capable of coordination to 99mTc. The coordination bond is not strong as covalent or ionic bond [21].To ensure the positive charge of complex, a technetium atom in a low oxidation state (+1) is reacted to monodentate isonitrile ligand to provide [Tc (-C=NR) 6] + with a hexacoordinated (octahedral) structure. Every carbon atom bound to the technetium possesses a non- paired electron (overlapping with the lone pair of adjacent nitrogen); hence, the technetium-sestamibi molecules are paramagnetic. Since isonitriles are volatile, not very stable Compounds, MIBI is available in stabilized form as copper tetrafluoroborate adduct, [Cu (MIBI) 4] BF4 which must be decomposed through labelling [23]. 99mTc-MIBI is taken up by the cells of the myocardium in passive diffusion [24], and then seems in the cytosol which is localized in mitrochondria. The uptake is proportional to the myocardial perfusion, and washout is rather slow (involving significant redistribution).
At stress, more than 3% of the injected dose is accumulated in the myocardium, while nonbound part is deleted through the hepatobiliary route. The proper situations to provide 99mTc-MIBI complex samples under ultrasound irradiation method were reported [17]. In new advanced approach, which locally induced heating related to ultrasound irradiation without heating to 65°C was not effective to provide the radiotracer in enough yield. Isonitrile as an electron donor group in sestamibi is coordinated to the technetium. The feature of this type of bonding is not strong as covalent bonding. Thus, elevated temperature above 65°C for more than 1 min could affect the feature of bonding or degrade the framework of 99mTc-MIBI complex under ultrasound irradiation situation. For this cause, yield of 99mTc-MIBI complex samples was considerably reduced. The past evaluation showed that the volume of freshly eluted 99mTc pertechnetate sodium, temperature and the period of ultrasound irradiation, due to the power of ultrasound instrument facility were the most significant factors to provide 99mTc-MIBI complex samples with enough yields.
The radio-HPLC and TLC analysis research have indicated successful reconstitution sestamibi kits by novel advanced modality. 99mTc-sestamibi is a lipophilic, monovalent cation which localizes in myocardial cells by easy diffusion without active transport. It was suggested that sestamibi molecule binds to a small molecular weight cytosolic protein [25]. Unlike thallium 201, it does not redistribute during the time. Hence, isolated injections have to be intravenously administrated to patient for stress and resting studies. The survey of the patients did not indicate significant differences in biodistribution of radiotracer samples in stress and rest phases that were provided due to ultrasound or boiled water bath techniques in present method. Visual analysis of images indicated a good image quality in every item. The consequence of our survey has indicated that providing 99mTc-MIBI complex samples by ultrasound irradiation method is reliable and reproducible approach to simplify reconstitution 99mTc-sestamibi kits. Providing 99mTc-MIBI
complex by novel advanced approach has under here benefits. The time labeling of sestamibi by pertechnetate sodium by ultrasound irradiation method versus water bath approach was considerably decreased. 99mTc-MIBI complex samples can be provided in enough amounts with good yields.
The samples geometry in ultrasound device was not significant element. No potential sparking risk is present for metal cap presence of the vial inside the ultrasound apparatus. In addition to above elements, the potential risk of absorbed ionization irradiation to nuclear medicine department personnel can be significantly reduced. The proposed method to provide 99mTc-MIBI complex could be done in any nuclear medicine centers which allowed a fast and reliable approach to make 99mTc-MIBI complex available for either routine or emergency utilization. To access it, it is required to set out this method in nuclear medicine departments to understand the proper situations from the case of temperature and the period of ultrasound irradiation due to instrument power.
Conclusion
This study’s results indicated that sonication irradiation approach can be proposed to provide 99mTc-MIBI radio- complex samples. The reaction time to provide radio- complex could be significantly decreased compared to boiling water bath approach. This main advancement may be reduced potential risk to the patient to inhibit any delay in the emergency conditions like acute therapy particularly for myocardial infarction patients in clinical practice. Green chemistry is an alternative approach for MIBI kit radiolabelling with 99mTc radioactive isotope.
References
-
Russe RR, Zaret BL (2006) Nuclear cardiology: Present and future. Curr Probl Cardiol 31(9): 557-629.
-
Fathala A (2011) Myocardial perfusion scintigraphy: techniques, interpretation, indications and reporting. Ann Saudi Med 31(6): 625-634.
-
Husain SS (2007) Myocardial perfusion imaging protocols: is there an ideal protocol? J Nucl Med Technol 35(1): 3-9.
-
Srivastava SC, Richards P (1983) Technetium- 99m labeled compounds, Radiotracers for Medical Applications (Rayudu, G.V.S., Ed.) CRC Press Inc Boca Raton FL pp: 107-185.
-
Fukushima K, Momose M, Kondo C, Kusakabe K, Kasanuki H (2007) Myocardial kinetics of (201)Thallium, (99m) Tc-tetrofosmin, and (99m)Tc-sestamibi in an acute ischemia-reperfusion model using isolated rat heart. Ann Nucl Med 21(5): 267-273.
-
Beller GA, Watson DD (1991) Physiological basis of myocardial perfusion imaging with the technetium 99m agents. Semin Nucl Med 21(3): 170-172.
-
Taillerfer R, Lambert R, Essiambre R, Phaneuf DC, Leveille J (1992) Comparison between thallium-201, technetium- 99m-sestamibi and technetium-99m-teboroxime planar myocardial perfusion imaging in detection of coronary artery disease. J Nucl Med 33(6): 1091-1098.
-
Manka Waluch A, Palmedo H, Reinhardt MJ, Joe A, Manka C, et al. (2006) Myocardial uptake characteristics of three 99mTc-labeled tracers for myocardial perfusion imaging one hour after rest injection. Ann Nucl Med 20(10): 663- 670.
-
Faerd Esfahani A, Fallahi B, Mohaghegh A, Assadi M, Beiki D, et al. (2010) The value of myocardial perfusion imaging with Tc-99m Mibi for the prediction of perfusion improvement after percutaneous transluminal coronary angioplasty. Iran J Nucl Med 18(1): 7-13.
-
Piwnica Worns D, Kronauge JF, Holman BL, Davison A, Jones AG (1989) Comparative myocardial uptake characteristics of hexakis (alkylisonitrile) technetium (I) complexes, effect of lipophilicity. Invest Radiol 24(1): 25-29.
-
Vecchio SD, Salvatore M (2004) 99mTc-MIBI in the evaluation of breast cancer biology. Eur J Nucl Med Mol Imaging 31: 88-96.
-
Aslan N, Ilgan S, Urhan M, Karacalioglu AO, Arslan I, et al. (1999) The role of technetium-99m-sestamibi parathyroid scintigraphy in the detection and localization of parathyroid adenomas in patients with hyperparathyroidism: comparison with technetium– thallium subtraction scan and ultrasonography. Turk J Endocrinol Metab 3(2): 47-52.
-
Tanaka S, Asao T, Ubukata M, Sugiyama H, Yajima Y, et al. (1997) Effectiveness of Tc-99m MIBI scintigraphy in diagnosing lung cancer. Surg Today 27(7): 623-626.
-
Williams CC, Kereiakes JG, Grossman LW (1981) The accuracy of 99Molybdenum assays in 99mTechnecum solutions. Radiology 138(2): 445‐448.
-
Da Silva Cdoa, Ribeiro BS, Souza WO, Araújo Fd, Lucena EA, et al. (2007) Application of bioassay techniques to evaluate 99Mo incorporation in nuclear medicine patients. Int Nuclear Atlantic Conf.
-
Fatima N, Zaman M, Niayz K, Reza H, Iqbal J, et al. (2008) Effective method to minimize molybdenum content of 99Mo-99mTc Generator eluate. Pak J Radiol 18(1): 20- 21.
-
Doroudi A, Saadati SM, Hassanpour H, Ahmadi F, Erfani M, et al. (2013) Preparation of 99mTc-MIBI complex under ultrasound irradiation. J Radioanal Nucl Chem 298(2): 1185-1190.
-
Hung Jc, Wilson ME, Brown ML, Gibbons RJ (1991) Rapid preparation and quality control method for technetium- 99m-2-methoxy isobutyl isonitrile (technetium-99m- sestamibi). J Nucl Med 32(11): 2162-2168.
-
US EPA website, EPA’s Green Chemistry Program.
-
Singh AK, Shukla SK, Quraishi MA (2011) Ultrasound mediated green synthesis of hexa-hydro triazines. J Mater Environ Sci 2(4): 403-406.
-
Hassanpour SH, Dehghani MA, Elhamasl R, Lalehzari R (2019) Effect of eluting the 99Mo/99mTc Generator More than Once in 24 h on the Efficiency of the 99mTc-MIBI Complex. Radiochemistry 61(1):73-80.
-
Wackers FJ, Berman DS, Maddahi J, Watson DD, Beller GA, et al. (1989) Technetium-99m hexakis 2-methoxyisobutyl isonitrile: Human biodistribution, dosimetry, safety and preliminary comparison to thallium-201 for myocardial perfusion imaging. J Nucl Med 30(3): 301-311.
-
Proulx A, Ballinger, Gulenchyn KY (1989) Routine determination of radiochemical purity of 99mTc-MIBI. Int J Rad Appl Instrum A 40(1): 95-97.
-
Savi A, Gerundini P, Zoli P, Maffioli L, Compierchio A, et al. (1989) Biodistribution of 99mTc methoxy-isobutyl- isonitrile (MIBI) in humans. Eur J Nucl Med 15: 597-600.
-
Mousa SA, Williams SJ (1986) Myocardial uptake and retention of Tc-99m hexakis-aliphatic isonitriles: evidence for specificity. J Nucl Med 27: 995.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO