Papillary Thyroid Carcinoma Revealed by Cranial Metastasis: Two Cases and Review of Literature
Differentiated thyroid carcinoma (DTC) is the most common pathological type of thyroid carcinoma, which includes papillary and follicular subtypes. DTC is usually indolent, characterized by a good prognosis, and long-term survival. Distant metastatic disease from thyroid carcinoma is becoming a rare problem. Total thyroidectomy itself has become less associated with morbidity than it once was. We describe two patients with papillary thyroid carcinoma metastatic to the skull who was seen recently. The management of this disease entity is discussed.
Introduction
Papillary thyroid carcinoma has a good prognosis and is mainly lymphatic in distribution. Blood-bone metastases are exceptional. The skull is a common site for metastases, accounting for 15% to 25% of all cancer patients [1]. The most common primary malignancy in breast cancer, followed by lung cancer, prostate cancer and malignant lymphoma, but thyroid cancers are extremely rare [1, 2], with only a small number of cases found in the literature. We report here two cases of papillary thyroid carcinoma revealed by cranial metastases.
Patients and Observations
Observation 1
The patient is 63 years old and had no previous history. She had presented for 20 years with an anterior cervical swelling progressively increasing in volume without any associated signs and not causing any consultation until 2 years ago.
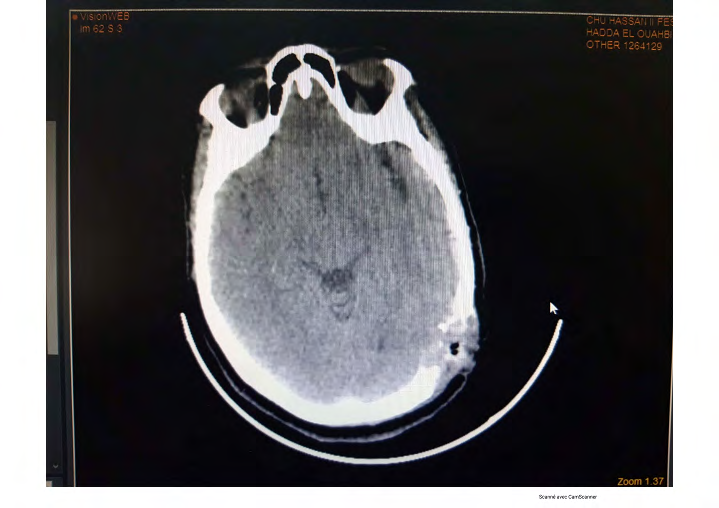
The patient presented with a large swelling of the scalp (left parietal region) rapidly increasing in volume, fistulated to the skin and bleeding spontaneously. A biopsy was performed at this level, the anatomopathological result was in favour of a metastasis of a vesicular carcinoma of the thyroid. Imaging (CT-scan) showed a 74x68x82mm expansive right thyroid tumour mass that plunged into the thoracic cavity and a 52x33mm osteolytic tissue mass in the left parietal vault with no obvious signs of cerebral parenchymal invasion and no other suspicious abnormalities elsewhere. Subsequently, the patient underwent total thyroidectomy, the pathological findings of which were consistent with an 8cm vesicular papillary thyroid carcinoma with the presence of vascular emboli without capsular invasion. The patient was put on suppressive Levothyroxine (Figure 1).

Observation 2
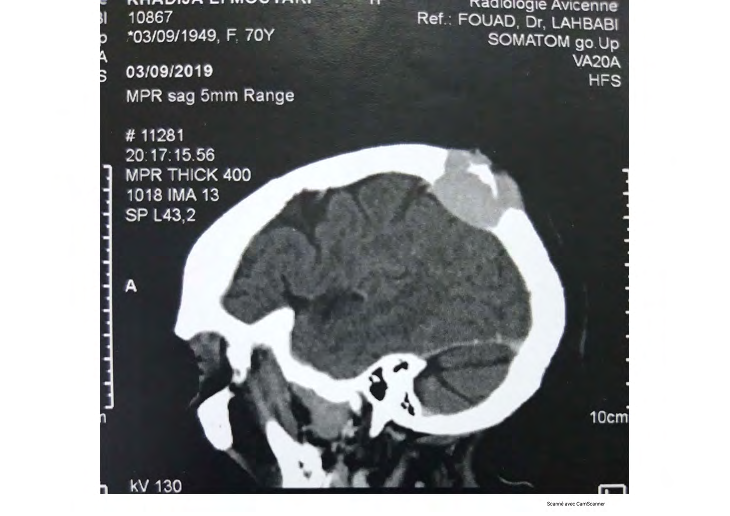
The patient is 68 years old, hysterectomized and hypertensive and on Amlodipine. The history of the disease dates back to 4 months with the appearance of a lesion of the scalp (left parietal region) whose removal with the anatomopathological study was in favour of a metastasis of a moderately differentiated carcinoma of thyroid follicular origin. Cervical examination revealed a stage Ia goitre in the right thyroid lobe with a firm nodule mobile in both planes without palpable cervical adenopathy. Cervical ultrasound
a b
showed a multi-nodular goitre classified as EU-TIRADS V. The CT scan showed a round, heterogeneous right lobar thyroid nodule without extra-thyroidal extension and a left parietal condensing bone lesion with a metastatic appearance. Subsequently, the patient underwent a total thyroidectomy, the anatomopathological study of which was in favour of a solid and vesicular variant papillary thyroid carcinoma of 3.1 cm with the presence of vascular emboli without capsular invasion. The patient was put on suppressive Levothyroxine (Figure 2).
Discussion
Vesicular or follicular carcinoma and papillary thyroid carcinoma are generally referred to as differentiated thyroid carcinoma, which is slow-growing and associated with a good prognosis. However, in the presence of distant metastasis, the prognosis is often poor [3]. Compared to papillary thyroid carcinoma (PTC), follicular thyroid carcinoma (FTC)] occurs in older patients and is frequently associated with distant metastasis and a higher mortality rate [4].
The incidence of developing distant metastases ranges from 1% to 9%, while distant metastases after initial treatment occur in approximately 7% to 23% of patients [5]. The most common site of distant metastases in DTC is the lung (49%) and the bone (24%); multiple sites are involved in about 20% of cases [6]. Indeed, bone is the most common site for FTC and the second most common site for PTC [7]. Bone metastases from FTC most commonly involve long bones such as the femur and flat bones, particularly the pelvis and sternum. The bones most often involved in PTC metastases are the ribs, vertebrae and sternum, while skull metastases from both FTC and PTC are extremely rare, accounting for 2.5% of all bone metastases, with the majority of skull metastases from thyroid cancers arising from FTC followed by PTC [4, 8, 9]. Being a rare location, cranial metastases are most often occipital in location and present as a soft, painless mass. Features of cranial metastases usually include a palpable scalp tumour, although unusual presentations of exophthalmos, disturbed consciousness, hemiparesis and headaches have also been reported. These lesions are osteolytic on radiography and CT and are highly vascular on angiographic evaluation [10, 11].
In differentiated thyroid carcinoma, distant metastases, especially cranial metastases, are not a common mode of disease manifestation. The largest series of cranial metastases from thyroid carcinoma described a frequency of only 2.5% in 473 patients [10]. In this series, the meantime from diagnosis of thyroid tumour to the discovery of cranial metastases was 23.3 years. The prognosis for metastases is generally poor and the 10-year survival with bone metastases from differentiated thyroid cancer is 27% [12]. However, the mean survival reported for patients with cranial metastases in the case series of Negamine et al, is only 4.5 years, suggesting that these patient subgroups tend to worsen [10]. Radioactive iodine therapy is essential to treat such metastatic disease. Indeed, lung metastases usually respond to radioiodine therapy. However, bone metastases rarely respond to radioiodine therapy and are associated with a poor prognosis [12]. Due to the low remission rate in radioiodine therapy and the poor prognosis in patients with bone metastases, the surgical approach should be considered as one of the treatments of choice for bone metastases, if possible. Curative resection of solitary bone metastases is associated with improved survival, particularly in younger patients [4, 13].
External radiotherapy should be given for unresectable or residual tumours [8, 14]. Kotecha, et al. reported that Gamma Knife Surgery (GKS) is an effective treatment modality for patients with metastases to the vault or skull base [1]. Patients with larger lesions near vital structures or in a previously irradiated field may benefit from fractionated stereotactic radiation [2]. Measurement of circulating TG to predict DTC recurrence during follow-up may be useful [14]. Despite synthetic therapy, outcomes for patients with cranial metastases as DTC are relatively poor, Nagamine, et al. reported that the mean survival time was 4.5 years, ranging from 5 months to 17 years in a series of 12 patients [8]. Li X, et al. reviewed previous reports and calculated that the overall survival of patients undergoing definitive treatment ranged from 14 months to 3.5 years from the time of discovery of the skull metastasis, with the survival of untreated patients being even shorter [15].
Conclusion
Indeed, both the skull base and the vault can be invaded by thyroid carcinoma but it is difficult to make a correct preoperative diagnosis because of its atypical clinical manifestations and imaging findings.
Although cranial metastases are a rare secondary location of vesicular thyroid carcinoma, these two observations represent an important contribution to this topic and remind us of the possibility of this disease and the considerations of differential diagnosis when faced with a cranial lesion.
References
-
Kotecha R, Angelov L, Barnett GH, Reddy CA, Suh JH, et al. (2014) Calvarial and skull base metastases: expanding the clinical utility of Gamma Knife surgery. J Neurosurg 121(S): 91-101.
-
Mitsuya K, Nakasu Y, Horiguchi S, Harada H, Nishimura T, et al. (2011) Metastatic skull tumours: MRI features and a new conventional classification. J Neurooncol 104(1): 239-245.
-
Cobin RH, Gharib H, Bergman DA, Clark OH, Cooper DS, et al. (2001) Thyroid carcinoma task force. AACE/AAES medical/surgical guidelines for clinical practice: Management of Thyroid Carcinoma American Association of Clinical Endocrinologists American College of Endocrinilogy. Endocr Pract 7: 202-220.
-
Zettinig G, Fueger BJ, Passler C, Kaserer K, Pirich C, et al. (2002) Long-term follow-up of patients with bone metastases from differentiated thyroid carcinoma- surgery or conventional therapy?. Clin Endocrinol (Oxf) 56(3): 377-382.
-
Sampson E, Brierley JD, Le LW, Rotstein L, Tsang RW (2007) Clinical management and outcome of papillary and follicular (differentiated) thyroid cancer presenting with distant metastasis at diagnosis. Cancer 110: 1451- 1456.
-
Chiofalo MG, Setola SV, Gennaro FD, Fulciniti F, Catapano G, et al. (2015) Follicular thyroid carcinoma with skull metastases. Endocrine Journal 62(4): 363-369.
-
Khan SH, Hassan MU, Bhau RS (2015) Iodine-131 avid distant metastasis in differentiated thyroid cancer: An initial institutional experience from the northern part of India. Indian J Nucl Med 30(3): 227-232.
-
Nagamine Y, Suzuki J, Katakura R, Yoshimoto T, Matoba N, et al. (1985) Skull metastasis of thyroid carcinoma. Study of 12 cases J Neurosurg 63(4): 526-531.
-
Atkinson AL, Rosenthal A, Nardiello D (2010) Follicular Thyroid Carcinoma Presenting as a Palpable Head Mass: A Case Report. Case Rep Oncol 3(2): 106-109.
-
Nagamine Y, Suzuki J, Katakura R, Yoshimoto T, Matoba N, et al. (1985) Skull metastasis of thyroid carcinoma. Study of 12 cases J Neurosurg 63: 526-531.
-
Akdemir I, Erol FS, Akpolat N, Ozveren MF, Akfirat M, et al. (2005) Skull metastasis from thyroid follicular carcinoma with difficult diagnosis of the primary lesion. Neurol Med Chir (Tokyo) 45(4): 205-208.
-
Schlumberger M, Tubiana M, De Vathaire F, Hill C, Gardet P, et al. (1986) Long-term results of treatment of 283 patients with lung and bone metastases from differentiated thyroid carcinoma. J Clin Endocrinol Metab 63(4): 960-967.
-
Bernier MO, Leenhardt L, Hoang C, Aurengo A, Mary JY, et al. (2001) Survival and therapeutic modalities in patients with bone metastases ofdifferentiated thyroid carcinomas. J Clin Endocrinol Metab 86(4): 1568-1573.
-
Matsuno A, Katakami H, Okazaki R, Yamada S, Sasaki M, et al. (2010) Skull base metastasis from follicular thyroid carcinoma -two case reports- Neurol Med Chir (Tokyo) 50: 421-425.
-
Li X, Zhao G, Zhang Y, Ding K, Cao H, et al. (2013) Skull metastasis revealing a papillary thyroid carcinoma. Chin J Cancer Res 25(5): 603-607.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO