A Large Bladder Sliding Hernia with Resulting Acute Renal Failure: Case Report and Literature Review
A sliding hernia is a rare type of inguinal hernia in which the hernia sac is partially formed by a wall of a viscus organ. Sliding hernias that involve the bladder may result in irritative and obstructive urinary symptoms. Rarely, these patients with acute renal failure. We present a case report of a patient with a sliding bladder hernia who presented with urinary incontinence and acute renal failure.
Introduction
A sliding hernia is a rare type of inguinal hernia in which the hernia sac is partially formed by a wall of a viscus organ. Sliding hernias that involve the bladder may present with either irritative or obstructive urinary symptoms. Ureteral obstruction and renal failure are rare complications of sliding hernias involving the bladder. We present a case of a41-year-old male who presented to the emergency room with complaints of urinary incontinence and an enlarged scrotum. He was found to be in urinary retention with resulting acute renal failure secondary to a sliding inguinal hernia involving his entire bladder and bilateral ureters.
Case
A 41-year-old man with uncontrolled hypertension presented to the emergency department for evaluation of worsening urinary symptoms. He reported a three-week history of urinary incontinence that was not associated with stress nor urge. He reported a sensation of incomplete emptying that started 2-days prior to presentation. The patient denieda history of hematuria, dysuria and kidney stones. Additionally, he denied fever, chills, weakness and abdominal pain. During a physical examination, he was noted to have an extremely enlarged scrotum that was not erythematous, indurated or tender to palpation. Patient reported a gradual sincrease in the size of his scrotum over the past 25 years (Figure 1).

Figure 1: He was evaluated further with labs and imaging. His labs were significant for an elevated creatinine of 5.17. His basic metabolic panel and complete blood count was otherwise unremarkable. His urine analysis was positive only for small blood. He was initially imaged with a retroperitoneal and scrotal ultrasound which demonstrated moderate, bilateral hydrouretero- nephrosis and a right inguinal hernia containing a large fluid-filled urinary bladder (Figure 2).
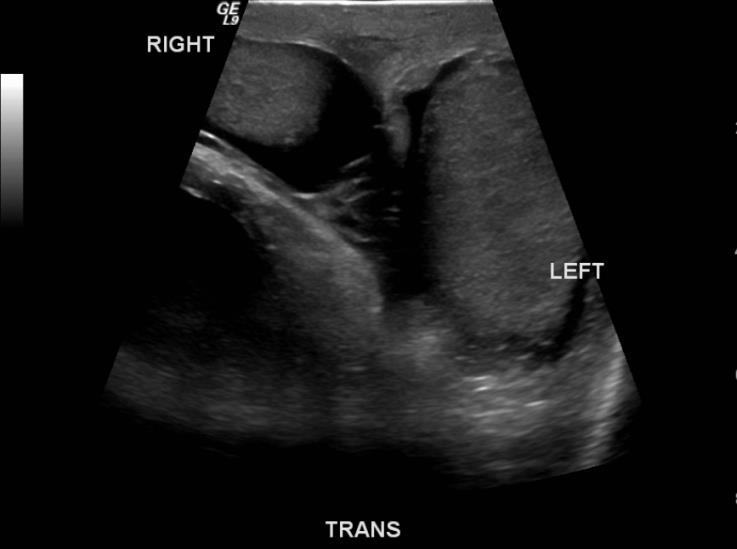
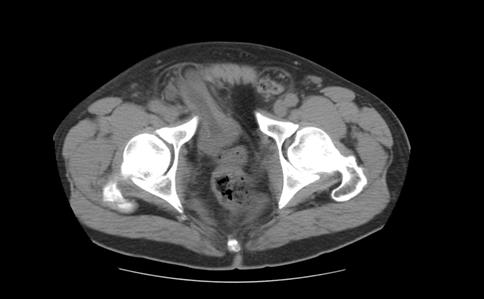
Figure 2: After his imaging was reviewed, a foley catheter was placed with return of 2 liters of urine. He re- examined following foley catheter placement and his scrotum had decreased in size. Additionally, he was noted to have increased urine output in foley when direct pressure was applied to scrotum. ACT scan was the performed which revealed a large sliding inguinal hernia 8with 90% of the bladder and bilateral ureters herniating into the scrotum (Figure 3).

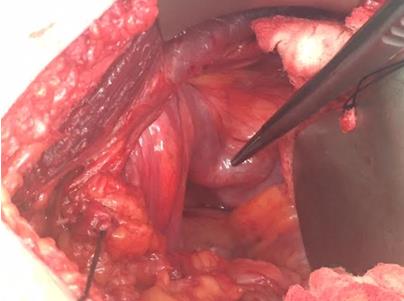
Figure 3: The patient was admitted and monitored for post obstructive diuresis. He received intravenous fluid resuscitation and by hospital day-two his serum creatinine had normalized. On hospital day-three, he was taken to the Operating Room for an inguinal hernia repair and reduction of bladder hernia. At the time of surgery, it was observed that the majority of the patients’ bladder (including the trigone, ureters and dome) was herniating into his right hemi-scrotum.
Discussion
As many as 4% of inguinal hernias involve the bladder [1, 2, 3]. The incidence increases to about 10% in men over 50 [4]. Identification of urinary bladder herniation usually occurs at the time of hernia repair. Herniation of the entire bladder into the scrotum is rare. Incarceration of the bladder occurs infrequently; however, strangulation with resulting necrosis has been reported [5]. Bladder herniation is more common in males versus females (70% and 30% respectively) [1]. Small bladder hernias may be asymptomatic. On the other hand, a patient who has a large bladder sliding hernia may present with either obstructive or irritative voiding symptoms. These symptoms include double-phase micturition, frequency, urgency, nocturia, and hematuria. Rarely, patients may also present with hydronephrosis and renal failure, acute or chronic, secondary to obstruction [6, 7, 8, 9]. Our case is an example of a large bladder containing hernia with resulting bilateral hydronephrosis and renal failure. In addition to hydronephrosis and renal failure, vesico- ureteric reflux, sepsis, cystolithiasis, and bladder strangulation with resulting ischemia are possible complications of inguinal bladder herniation [4, 9, 10, 11, 12]. Pre-operative imaging may be employed if there is suspicion of a bladder hernia based on history and physical exam. Imaging studies may include retrograde and voiding cystourethrograms [4]. Other diagnostic studies such as computed tomography, cystoscopy, and ultrasounds can also be considered. Most bladder hernias are diagnosed intra-operatively at the time of herniorrhaphy. A bladder hernia should either be reduced completely or a partial cystectomy is performed to remove the herniated portion of the bladder [13]. Other indication for partial cystectomy is the presence of bladder ischemia. The hernia should then be repaired in the usual fashion.
Conclusion
The urinary bladder is involved in about 4% of inguinal hernias. However, herniation of the entire bladder and ureters into the scrotum occurs rarely. One should consider a sliding bladder hernia in a patient with a history of an inguinal hernia with obstructive or irritative voiding symptoms. Although bladder involvement is usually diagnosed intraoperatively, preoperative diagnostic studies may be ordered if one has a high suspicion of bladder herniation. Surgical reduction or resection of the bladder should be performed prior to the herniorrhaphy.
References
-
Watson LF (1948) Hernia. St Louis, CV Mosby Co.
-
Koontz AR (1955) Sliding hernia of diverticulum of bladder. Arch Surg 70(3): 436-438.
-
MMadden JL, Hakim S, Agorogiannis AB (1971) The anatomy and repair of inguinal hernias. Surg Clin North Am 51(6): 1269-1292.
-
Gomella LG, Spires SM, Burton JM, Ram MD, Flanigan RC (1985) the Surgical Implications of Herniation of the Urinary Bladder. Arch Surg 120 (8): 964-967.
-
Bell ED, Witherington R (1980) Bladder hernias. Urology 15(2): 127-130.
-
Iason AH (1944) Repair of urinary bladder herniation. Am J Surg 63(1): 69-77.
-
Bisharat M, Donnell MEO, Thompson T, Mac Kenzie N, Kirkpatrick D, et al. (2009) Complications of inguinoscrotal bladder hernias: a case series. Hernia 13(1): 81-84.
-
Bjurlin MA, De Laurentis DA, Jordan MD, Richter HM III (2010) Clinical and radiologic findings of a sliding inguinoscrotal hernia containing the urinary bladder. Hernia 14 (6): 635-638.
-
Laniewski PJ, Watters GR, Tomlinson P (1996) Herniation of the bladder trigone into an inguinal hernia causing acute urinary obstruction and acute renal failure. J Urol 156(45): 1438-1439.
-
Vindlacheruvu RR, Zayyan K, Burgess NA, Wharton SB, Dunn DC (1996) Extensive bladder infarction in a strangulated inguinal hernia. Br J Urol 77(6): 926- 927.
-
Casas JD, Mariscal A, Barluenga E (1998) Scrotal cystocele: US and CT findings in two cases. Comput Med Imaging Graph 22(1): 53-56.
-
Thompson JE Jr, Taylor JB, Nazarian N, Bennion RS (1986) Massive inguinal scrotal bladder hernias: a review of the literature with 2 new cases. J Urol 136(6): 1299-1301.
-
Karatzas A, Gregory C, Michael S, Christos S, Evangelos A, et al. (2013) a giant inguino-scrotal bladder hernia as a cause of chronic renal failure: a rare case. International journal of surgery case reports 4(3): 345-347.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review