Malignant Phyllodes Tumour in a 42 Year Old Mother
One among every nine women is diagnosed with breast cancer and it is the second main cause of death by cancer in women. Ductal carcinoma is the most common histopathological type of breast cancer. Phyllodes tumours are rare fibro epithelial lesions and constitute to about 0.3–0.9% among female breast tumours and occur in the 4th decade of life. Here we present a 42 year old mother who came to our ER with complaints of right sided breast lump and mastalgia for 6 months. She was diagnosed to have angiosarcoma through FNAC. She was admitted in our hospital for further evaluation and management. The tumour was staged as T3 N1 M0. The patient was taken up for modified radical mastectomy of the right breast with latissimusdorsi flap reconstruction. Histopathology reports suggested poorly differentiated sarcoma in a background of malignant phyllodes tumour. 3 out of 13 nodes were positive for nodal involvement.
Background
One among every nine women is diagnosed with breast cancer. It has the second highest mortality rates. Ductal carcinoma is the most common histopathological type of breast cancer. Phyllodes tumours are rare fibro epithelial lesions and constitute to about 0.3–0.9% among female breast tumours. They mostly occur in the 4th decade of life [1]. In 1774, Phyllodes tumour was described as a type of fibro adenoma, followed by chelius in 1827. Johannes Muller [1838] coined the term cystosarcomaphyllodes because of the tumours macroscopic appearance, leaf like pattern [2]. Later in 1931, the first case of malignant phyllodes tumour was reported by Lee B, et al. [3]. Malignant potential of the tumour was reported by Cooper, et al. in 1943 [4]. In 1981 the World Health Organization [5] adopted the term phyllodestumour and was sub classified based on various histological features. The classification was benign, borderline, or malignant and the histological features were tumour margins, stromal over growth, tumour necrosis, cellular atypia, and number of mitosis per high power field. The majority of phyllodestumours are benign [35% to 64%]. This tumour has an unpredictable course that is not all of malignant forms are metastasizing and some of the benign ones can also metastasize [1].
A 42 year old mother presented to our emergency department with complaints of right sided breast lump associated with mastalgia for the past 6 months. She was evaluated in a different hospital and was diagnosed to have angiosarcoma through FNAC. She was admitted in our hospital for further evaluation and management. The patient’s detailed history was impeccable except for having undergone fertility treatment for 5 years following which a girl baby was born of caesarean section [5 years old now] and was breast fed for 1 year. On examination (Figure 1) the patient had a 15x11x11 cm mass in the right breast with one palpable ipsilateral lymph lode. There was a scar in the lower outer quadrant which was in favour of FNAC site scar. The tumour was not fixed to the chest wall and there was no skin ulceration or other skin changes.

Investigations
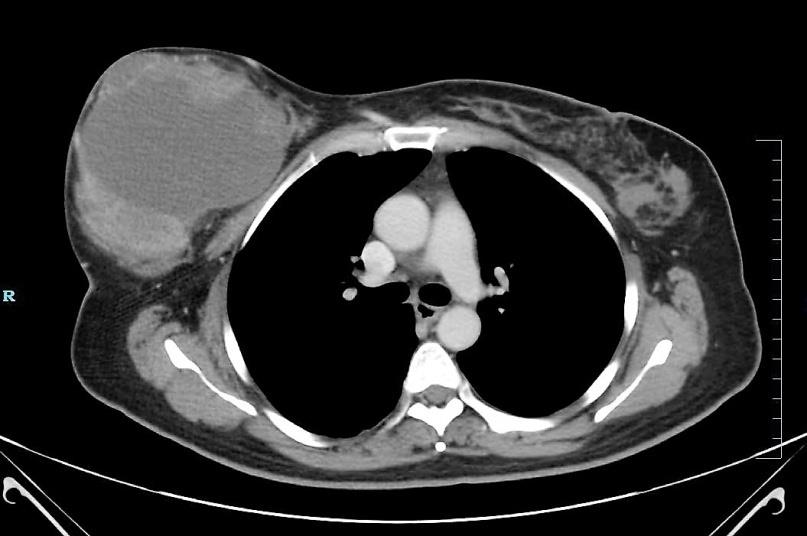
A USG mammogram, CT thorax (Figure 2) and USG abdomen with pelvis were done to stage the tumour. Subsequently the tumour was staged as T3 N1 M0.
Routine blood investigations revealed elevated platelets and a low haemoglobin, which was corrected with blood transfusion.
Treatment
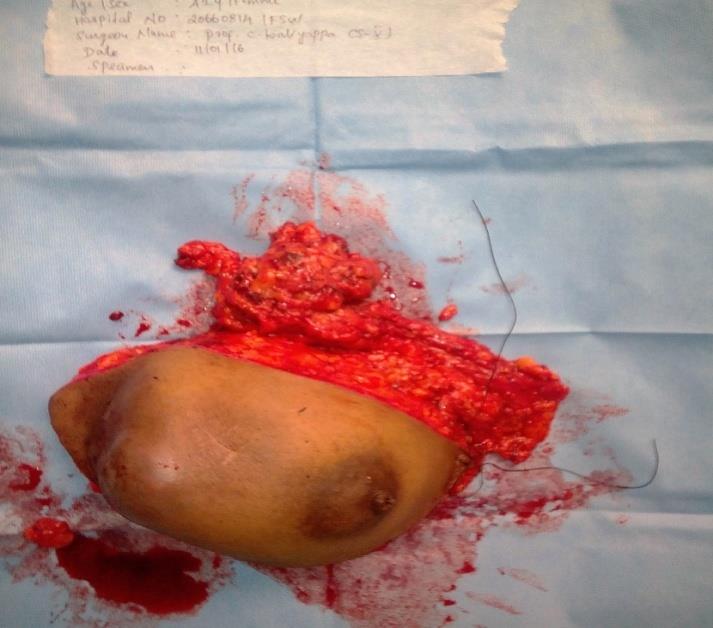
The patient was later taken up for modified radical mastectomy of the right breast with latissimusdorsi flap reconstruction (Figure 3). Intra operative and post- operative periods were uneventful. Drains were removed on POD 5 and sutures were removed on POD 11 and 12.

Outcome and Follow-Up
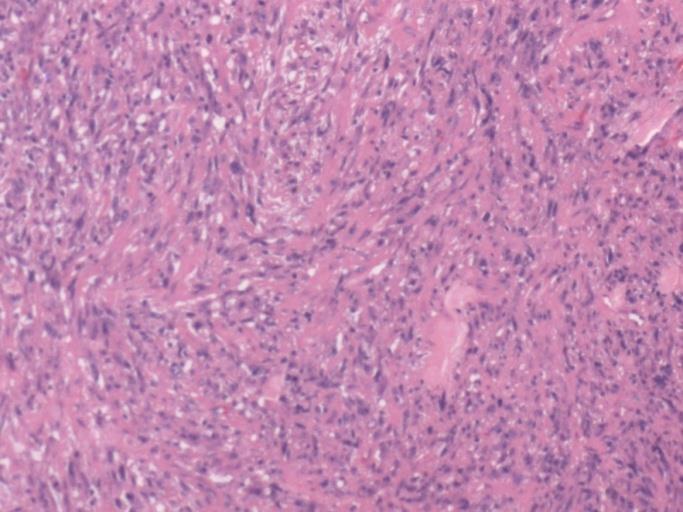
Histopathology reports suggested poorly differentiated sarcoma in a background of malignant phyllodes tumour – high grade. 3 out of 13 nodes were positive for nodal involvement. Tumour was seen to invade the dermis of the skin and there was no evidence of lymph vascular invasion (Figure 4 & 5).
Discussion
Cystosarcomaphyllodes are rare fibro epithelial lesion. They are often confused with sarcomas [6]. The incidence of these tumours is about 2.1 per million and constitutes for about 0.3 to 0.5 % of all female breast tumours. The peak age in women is between 45 and 49 years [1] Malignant phyllodes is observed in <1% amongst breast cancer [7]. These tumours are more common among Latin American white and Asian populations [8]. So far 10 cases have been reported on a rare combination of phyllodes tumour coexisting with breast carcinoma [9]. Primary breast sarcomas arise from mesenchymal tissue of the mammary gland and the incidence is calculated to be 45 per 10 million women. These tumours generally have high recurrence rates and poor prognosis. Phyllodes tumours are composed of connective tissue stroma and epithelial elements. Pathological presentation ranges from grade I to malignant phyllodes tumours [grade III] where the stromal component clearly exhibits a sarcoma pattern. The exact etiology of phyllodes tumour is still unclear. However, some studies have suggested that, in fibro adenomas, there is a monoclonal proliferation due to a somatic mutation. This clonal analysis is well supported with the tumours natural propensity to local recurrence [10]. There’s yet another theory that says growth factor produced by the breast epithelium may cause stromal induction leading to phyllodes tumours. [7]Apart from these, tumour growth can be stimulated by Trauma, lactation, pregnancy and increased oestrogen activity. Some studies have also stated that endothelin-1, a stimulator of breast fibroblast growth, may be involved [8]. Some studies have also shown that an upregulation of several angiogenesis-related genes including VEGFA, Angiopoietin-2, VCAM1, PDGFRA, and PTTG1 play a major role in this tumours aetiology [7]. The pathogenesis of phyllodes tumour is that it arises from outside of the ducts and lobules and occurs mostly in the breast’s connective tissue unlike breast carcinoma otherwise called stroma which surround the ducts and lobules along with vessels and lymphatics [8, 11] Pătraşcu et al. [1] in 2009 have suggested that phyllodes tumour is unilateral, more common over the right breast and <1% of the tumours are bilateral [1]. These tumours are typically painless rapidly growing tumours [12]. Diagnosis by FNAC can be difficult as both phyllodestumours and fibro adenomas belong to a spectrum of fibro epithelial lesions. The value of FNAC in the diagnosis of phyllodestumour remains controversial, with an overall accuracy of about 63%. Core tissue biopsy is an attractive alternative to FNAC because of the extra architectural information provided by histology compared with cytology. It is suggested that the sensitivity of core needle biopsy is 99% [13]. On the other hand Sato et al in 2016 suggested that sensitivity of core needle biopsy for diagnosis of phyllodes tumour is 63% and imaging was 65%. Hence it was suggested that a therefore complete surgical excision is usually required for final assessment [9]. Surgical management is the mainstay but the type of surgery has been a source of debate over the years. Studies have shown no differences between breast conserving surgery and mastectomy, but there is a higher incidence of local recurrence with breast conserving surgery [8]. But a simple mastectomy or a lumpectomy with negative margins is sufficient to avoid recurrence [6] Axillary lymphatic clearance should be avoided as phyllodes rarely metastasize to lymph nodes [9] Malignant phyllodes tumours spread haematogenous, hence Axillary dissection is required, when histology shows malignant cells [8] Immediate breast reconstruction can be performed but the challenge is when tumours grow larger than 10 cm, making it difficult for surgeons to get a clear negative margin [8]. Malignant phyllodestumours can grow rapidly and show metastasis if inadequately treated. In contrast, benign phyllodestumours on clinical, radiological, and cytological examination are often indistinguishable from fibro adenomas and can be cured by local surgery. With the non-operative management of fibro adenomas widely adopted, the importance of phyllodestumours today lies in the need to differentiate them from other benign breast lesions. Treatment can be either wide local excision or mastectomy provided negative margins are ensured [8]. Stromal overgrowth, surgical margin status, tumour necrosis, and histologic subtype are reported to be the predictors for local or distant recurrence after primary surgery [14].
Learning Points/Take Home Messages
- Diseases can present in a wide range of signs and symptoms.
- Malignant transformation of phyllodes is possible and it has to be a part of the differential diagnosis.
- Surgery is the mainstay of management in such cases.
References
-
Pătraşcu A, Popescu CF, Pleşea IE, Bădulescu A, Tănase F, et al. (2009) Clinical and cytopathological aspects in phyllodes tumors of the breast. 50(4):605– 611.
-
Muller J (1838) Ueber den feinern Bau und die Formen der krankhaften Geschwülste. berlin 54-60.
-
Lee B, Pack G (1931) Giant intracanalicular fibroadenomyxoma of the breast. Am J Cancer 15: 2583-2609.
-
Mishra SP, Tiwary SK, Mishra M, Khanna AK (2013) Phyllodes Tumor of Breast : A Review Article Phyllodes Tumor of Breast : A Review Article.
-
(1981) World Health Organization. Histologic typing of breast tumours In: breast tumours.
-
Verma V, Muttineni S, Kulkarni RR, Silva-lopez E, West WW, et al. (2015) Enormous, rapidly growing breast mass. BMC Cancer 15: 4-7.
-
Gatalica Z, Vranic S, Ghazalpour A, Xiu J, Mcgill J, et al. (2015) Multiplatform molecular profiling identifies potentially targetable biomarkers in malignant phyllodes tumors of the breast. Oncotarget. 7(2): 1701-1716.
-
Mishra SP, Tiwary SK, Mishra M, Khanna AK (2013) Phyllodes Tumor of Breast : A Review Article.
-
Sato T, Muto I, Sakai T (2016) Case Report - Open Access International Journal of Surgery Case Reports Coexistence of malignant phyllodes tumor and her2- positive locally advanced breast cancer in distinct breasts : A case report CASE REPORT - OPEN ACCESS. Int J Surg Case Rep Surgical Associates Ltd 19: 163- 167.
-
Majeski J, Stroud J (2012) Malignant Phyllodes Tumors of the Breast : A Study in Clinical Practice. 97(2): 95-98.
-
Ünal B, Erdoğan G, Karaveli FŞ (2015) Step by step approach to rare breast lesions containing spindle cells. Springerplus.
-
Sbeih MA, Engdahl R, Landa M, Ojutiku O, Morrison N, et al. (2015) Case Report A giant phyllodes tumor causing ulceration and severe breast dis fi gurement : case report and review of giant phyllodes. 1-4.
-
Rakha EA, Aleskandarany MA, Lee AHS, Ellis IO (2016) An approach to the diagnosis of spindle cell lesions of the breast. 68(1): 33-44.
-
Lee CM, Macdonald OK, Tward JD, Chappel CD, Gaffney DK (2006) Malignant Phyllodes Tumor of the Female Breast. Cancer 107(9): 2127-2133.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review