Left Side Spigelian Hernia Containing Tuberculous Ovary with Abscess Formation - Case Report
Spigelian hernia is a rare entity, representing about 0.12% of all abdominal wall hernias. The causes of Spigelian hernias are, involving both congenital and acquired factors and up to 50% of these hernias occur in patients with a history of previous abdominal surgery, it is slightly more common in females, usually on left side and the median age of presentation is 50 years. The most common content of the Spigelian hernia sac is the greater omentum; but, an involvement of other organs has been reported. A few cases of spigelian hernia containing ovary have been reported in the literatures. Isolated tuberculous salpingo- oophoritis is rare female genital tract tuberculosis. Her we presented a 51 years old female with Left side Spigelian hernia containing tuberculous ovary with abscess formation. Up to our Knowledge; there was no reported case of spigelian hernia that contained a tuberculous ovary; thus, our patient may be the first case in this topic.
Introduction
Spigelian hernia is a rare entity, representing about 0.12% of all abdominal wall hernias. The majority of Spigelian hernias occur in the area of Spigelian line just distal to the umbilicus where the posterior sheath is deficient [1]. The causes of Spigelian hernias are, involving both congenital and acquired factors and up to
50% of these hernias occur in patients with a history of previous abdominal surgery, it is slightly more common in females, usually on left side and the median age of presentation is 50 years [2]. The most common content of the Spigelian hernia sac is the greater omentum; but, an involvement of other organs has been reported, including the small intestine, colon, stomach, gallbladder, Meckel's diverticulum, appendix, ovaries and/ or fallopian tube [3]. Here, we report a case of Spigelian hernia containing tuberculous ovary with abscess formation.
Case Presentation
A 51 years old female presented to our emergency department with 7 days history of left iliac fossa pain increasing in severity over the last 2 days associated with anorexia. Her surgical history was involved a three previous elective Cesarean sections. She had received the Bacille Calmette-Guerin (BCG) vaccination at birth and there was no history of contact with tuberculosis. Have no history of trauma and the medical history were not significant. On examination; her body temperature was 38°C, the pulse rate was 110 beat/minutes and the blood pressure was 110/60 mmHg. No visible or palpable mass was detected on abdominal examination, but there was severe tenderness in the left iliac fossa even on superficial palpation, her bowel sound was normal, and the blood investigations revealed leukocytosis. Her abdominal ultrasound reveals a small complex mass with fluid collection within few centimeters below and to the left of the umbilicus just beneath the external oblique aponeurosis, the left ovary was difficult to visualize. Her abdominal CT scan revealed a left side Spigelian hernia located about 4 cm distal to the umbilicus, just lateral to the rectus muscle, containing swollen, edematous left ovary that trapped beneath the intact external oblique aponeurosis with fluid collection (Figure 1).
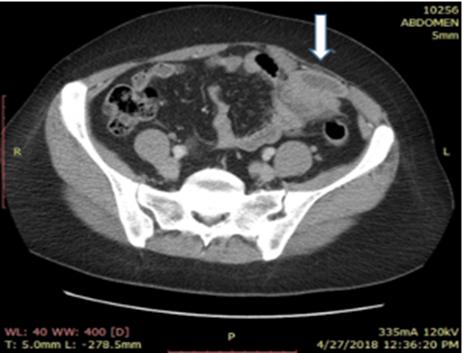
Figure1: Left side Spigelian hernia containing an incarcerated left ovary with fluid collection (white arrow).
Operative Technique
A transverse abdominal incision has been made over the point of maximum tenderness that marked previously before general anesthesia; a slight localized bulging in the area of the junction between the external Apo neurosis and external rectus sheath had been identified. A transverse incision was made over this bulge, identification of a sloughed ovarian tissue with severe infection and pus formation, after suctioning of the pus and removal of all sloughed ovarian tissues, the narrow orifice of the Spigelian hernia had been identified that still containing a strangulated, adherent distal parts of the fallopian tube. A small elliptical incision was made around the hernia orifice to enter safely to the abdominal cavity (Figure 2).
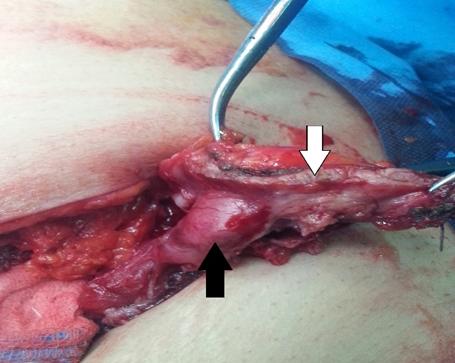
Complete excision of the herniated left fallopian tube was done, and the elliptical incision that extended over the lateral aspect of the transverses abdominis muscle and the medial aspect of the rectus abdominis muscle was closed directly with simple anatomical repair without tension, then the other layers of the wound were closed, and the patient transferred to the surgical ward after recovery from anesthesia and discharged from hospital after 5 days with normal general condition without any complications.
The excised specimen consisted of an irregular mass (8x6x4cm) with fallopian tube. Microscopic examination of this specimen revealed features consistent with the diagnosis of TB salpingo – oophoritis; a chronically inflamed granulation tissue with multiple caseating epithelioid granulomas and several Langhan’s gaint cells.
Discussion
It is difficult to diagnose Spigelian hernia clinically due to its rarity and the absence of classic symptoms and there are various differential diagnoses to be considered like abdominal wall hematoma, abscess, and neoplasms, the performance of a diagnostic imaging can help differentiate these conditions. Abdomen and pelvis CT; demonstrates a sensitivity of 100% and positive predictive value of 100%. It is more reliable at identifying incarcerated or strangulated spigelian hernia than ultrasound [4]. Isolated TB salpingo- oopheritis is a rare female genital tract tuberculosis [5]. In our reported case; the only abnormal findings in the CT abdomen and pelvis are the presence of left side spigelian hernia containing abnormal left adnexia with abscess formation which proved postoperatively by histopathological examination as a TB salpingo- oopheritis. A few cases of spigelian hernia containing ovary have been reported in the literatures [6, 7, 8]. Up to our Knowledge; there was no reported case of spigelian hernia that contained a TB ovary, Thus; our patient may be the first case in this topic.
Conclusion
Spigelian hernia is a rare abdominal wall hernia, carry a high risk for strangulation. Clinical diagnosis is challenging and CT scan is the diagnostic study of choice
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgement: None.
References
-
Sharma A, Soni V, Baijal M, Chowbey P, Mittal T, et al. (2008) Diagnosis and management of Spigelian hernia: A review of literature and our experience. Journal of Minimal Access Surgery 4(4): 95-98.
-
Baucom C, Nguyen QD, Hidalgo M, Slakey D (2009) minimally invasive Spigelian hernia repair. JSLS 13(2): 263-268.
-
Strambi S, Pucci V, Liserre J, Spinelli G, Palombo C, et al. (2014) Spigelian Hernia in a 14-Year-Old Girl: A Case Report and Review of the Literature. European Journal of Pediatric Surgery Reports 2(1): 58-62.
-
Light D, Chattopadhyay D, Bawa S (2013) Radiological and clinical examination in the diagnosis of Spigelian hernias. The Annals of the Royal College of Surgeons of England 95(2): 98-100.
-
Rabesalama S, Mandeville K, Raherison R, Rakoto- Ratsimba H (2011) Isolated ovarian tuberculosis mimicking ovarian carcinoma: Case report and literature review. African Journal of Infectious Diseases 5(1): 7-10.
-
Walton JM, Bass JA (1995) Spigelian hernias in infants: report of two cases. Can J Surg 38(1): 95-97.
-
Hill CS, Chahil B, Marlow B (2012) Ovarian Spigelian hernia: A radiological diagnosis. Radiography 18(2): 137-139.
-
Khadka P, Dhakal SKS (2017) Case report of ovary and fallopian tube as content of a Spigelian hernia – A rare entity. International Journal of Surgery Case Reports 31: 206-208.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review