Effect of Hirudotherapy in Bakers Cyst
Bakers cyst is also known as popliteal cyst. There is collection of fluid behind the knee joint & is due to swelling of popliteal bursa. This type of the abnormality usually does not show any symptoms. However in chronic cases with secondary trauma or wear & tear, there may be swelling, pain, tenderness & the affected knee may get stiff. In allopathic medicine the treatment given is purely supportive care and if it does not suffice then aspiration is done. In some cases steroid injection or sclerotherapy is given & if it fails or show recurrence, then surgical removal is the treatment of choice. Keeping the side effects, short falls, recurrence & cost effect in view Hirudotherapy has been used for the treatment of bakers cyst. Here 5 leeches were applied locally at the popliteal fossa preferably on the swelling. The procedure was done every after 10 days & total number of therapies given were five. It was observed that the cysts was completely resolved in all of the patients and did not show any recurrence even after follow up for 2 year.
Introduction
Baker’s cyst was first described by William Morrant Baker [1] & was first described in 1840 by Adams as popliteal cyst [2]. It represents fluid collection & destruction of the gastroenemius-semimembranous bursa which usually communicates with the knee joints in adults and the cyst most often contains upto 40ml of fluid [3].This cyst is clinical found in the chronic osteoarthritis patients and in patients with degenerative joint diseases. The risk factor can be osteoarthritis, meniscal tear; Rhematoid artheritis [4, 5, 6]. The Baker’s cyst is diagnosed clinically & can be confirmed radiologically by ultrasound or MRI (Magnetic resonance imaging). The differential diagnoses of acute calf pain include DVT, Baker’s cyst, muscular injury, tumour, infection, arterial aneurysm, and Achilles tendon pathology [7]. Emphasis is often placed on DVT owing to the risk of pulmonary embolism. Ultrasonography has largely replaced arthrography for the initial assessment of Baker’s cyst [8]. In ultrasonography, Baker’s cysts are demonstrated as consisting of three parts: the base, the superficial part, and the neck in between. The neck lies between the medial head of gastrocnemius and the semimembranosus tendon. Baker’s cysts can be complicated by dissection, which usually occurs in a distal direction [9]. Cysts can rupture and their fluid content can track into the fascial planes between the soleus and gastrocnemius muscles.
This can cause inflammatory changes within the subcutaneous fat and muscles. The clinical appearance of the leg can be very similar to those with acute thrombophlebitis. Therefore, ruptured Baker’s cyst is also referred to as 'pseudo thrombophlebitis'.
Materials and Methods
Around 20% of people have Baker’s cyst [5, 10]. Baker’s cyst occurs most commonly between 35 to 70 year of age [6]. 4.5%Incidence is found in patients undergoing radiological investigation like MRI for some other problem [11].It has been reported that in 94% of patients baker’s cyst has been associated with one or more disorders related to knee joint and the local compression of sciatic nerve due to proximal dissection of cyst [12, 13]. A study reveals that 40% of patients with osteoarthritis had baker’s cyst detected by ultrasonography. In rheumatoid arthritis, up to 48% of patents have been shown to have baker’s cyst [14]. Bilateral cyst where seen in 16% of the patients. Distribution of Patients According To Mizaj (Temperament) The present study is single group open clinical study. Seven patients were selected from general OPD of Regional Research Institute of Unani Medicine, University of Kashmir, Srinagar & screened before undergoing the scientific study. The local part (Popliteal fossa) was prepared by initially washing with plain water & then full antiseptic measures were taken to avoid any sort of infection. The patients were given Hirudotherapy every after ten days for a period of fifty days. The leeches were put locally on the swelling (Baker’s Cyst) & allowed to suck till they fill up their belly & fall down of their own.
Five leech were applied on day one & at every follow up. The part were allowed to bleed for about 1 to 2 hours & then antiseptic bandaging were done.
Incidence
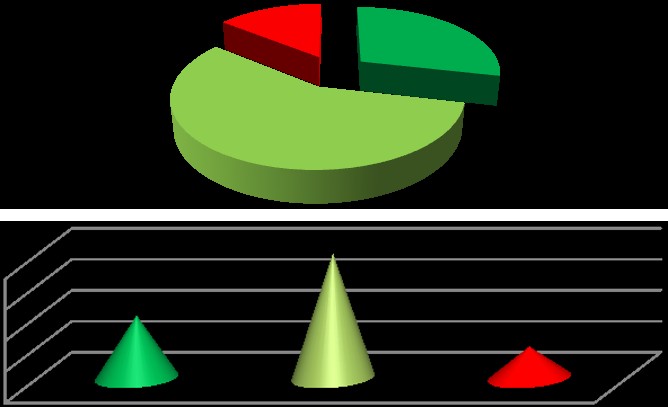
| S.No. | Mizaj (Temperament) | Number of Patients |
|---|---|---|
| 1 | Damwi (Sanguineous) | 1 |
| 2 | Safrawi (Bilious) | 2 |
| 3 | Balghami (Phlegmatic) | 4 |
| 4 | Saudawi (Black Bile) | 0 |
| Total | 07 |
Percentage of Patients according to Temperament (Mizaj)
Saudawi (Black Bile)
0% Damwi (Sanguineous
) 14%
Number of Patients according to Temperament
(Mizaj)
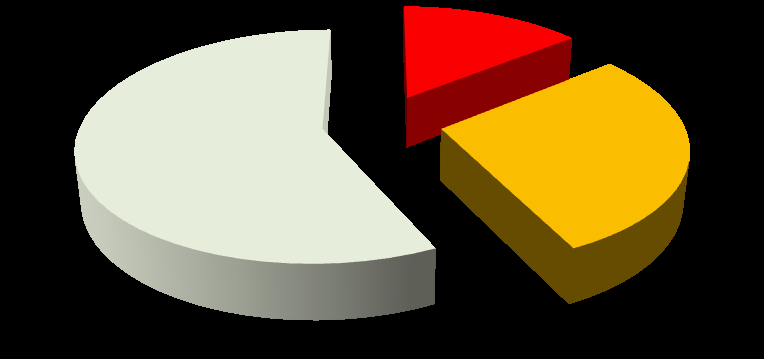
| S.No. | Socio-economic Status | Number of Patients |
|---|---|---|
| 1 | Higher income group | 2 |
| 2 | Middle income group | 4 |
| 3 | Lower income group | 1 |
| Total | 07 |
Percentage of Patients according to Socio-
Lower income
economic Group
group Higher income
group %
Number of Patients according to Socio-
economic Group
Higher income group
Middle income group
Lower income group
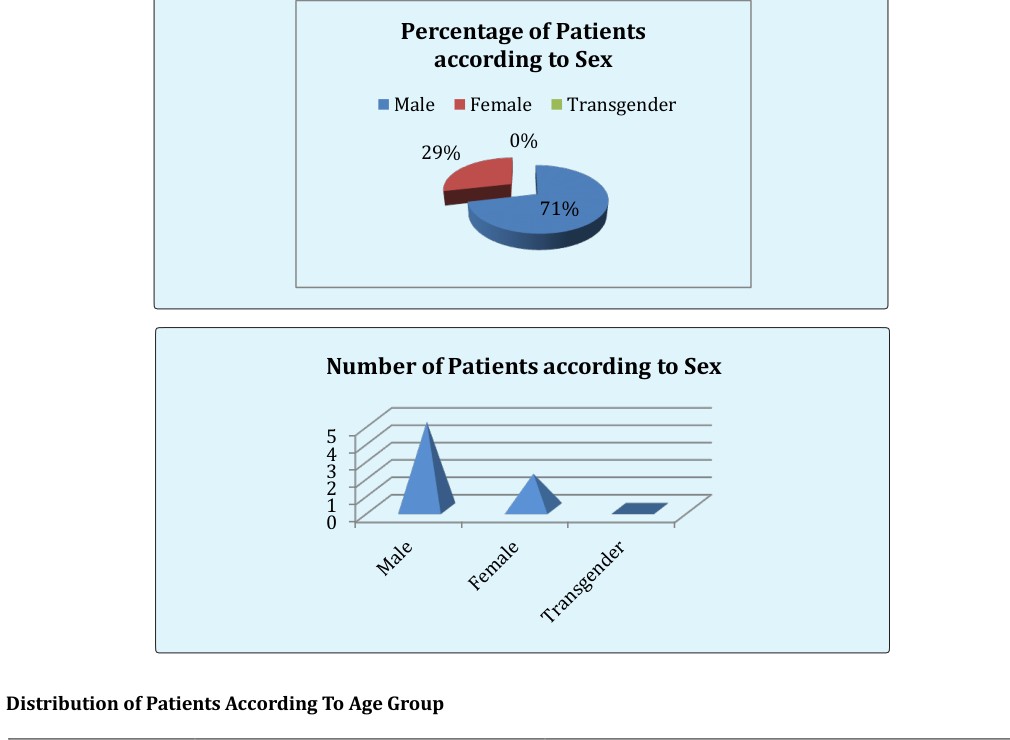
Distribution of Patients According To Sex
| S.No. | Sex | Number of Patients |
|---|---|---|
| 1 | Male | 5 |
| 2 | Female | 2 |
| 3 | Transgender | 0 |
| Total | 07 |
| S.No. | Age Group | Number of Patients |
|---|---|---|
| 1 | 40-45 | 1 |
| 2 | 46-50 | 1 |
| 3 | 51-55 | 3 |
| 4 | 56-60 | 2 |
| 5 | 61-65 | 0 |
| Total | 07 |
Percentage of Patients according to Age Group
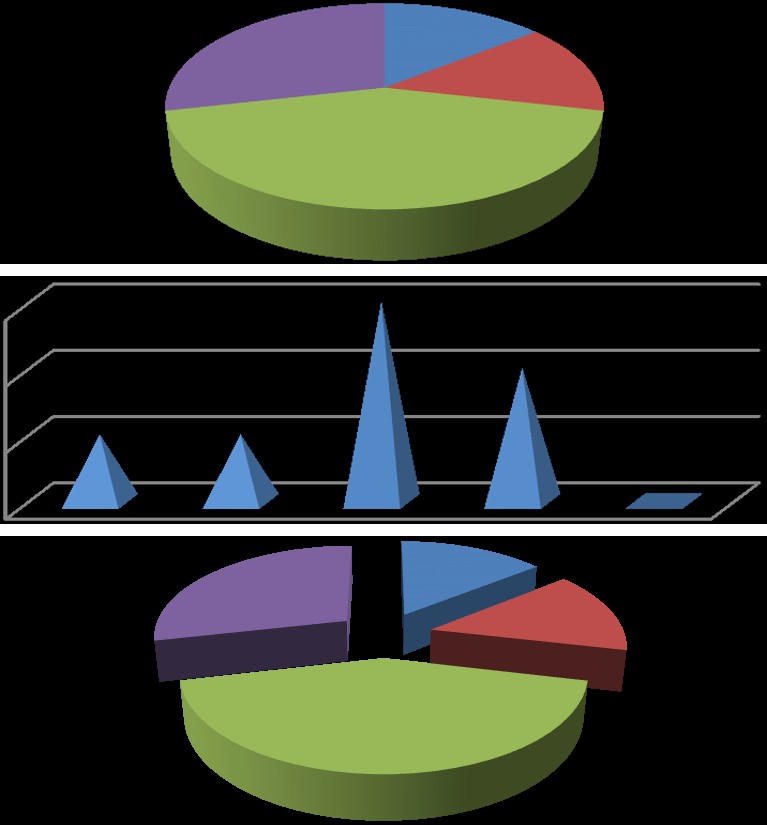
Number of Patients according to Age Group
40-45 46-50 51-55 56-60 61-65 Distribution of Patients According To B.M.I.
| S.No. | Classification | B.M.I. Range | Number of Patients |
|---|---|---|---|
| 1 | Normal weight | 18.5–24.9 | 1 |
| 2 | Over weight | 25.0–29.9 | 1 |
| 3 | Obese | 30.0–34.9 | 3 |
| 4 | Extreme Obesity | 35.0–39.9 | 2 |
| TOTAL | 07 |
Percentage of Patients according to B.M.I.
Extreme
Obesity
Normal weigh
t 14% Over weight
Number of Patients according to B.M.I.
Normal
weight Over weight Obese Extreme
Obesity
Discussion
Baker’s cyst usually arise due to chronic osteoarthritis, Rheumatoid atheritis or due to menescial taer. Baker’s cyst is now a days the commonest menifertation and mostly become symptomatic when associated with some associated ailments like deep venous thrombosis, chronic OA with osteophyte formation, thrombophlebitis, local trauma. In case there is increased accumulation of fluid in the cyst, there may be local pain with swelling and if the cyst ruptures it causes bruising below the Medial malleolus of the ankle known as crescent sign.
In children the Baker’s cyst may not be due to any underlying joint disease. The baker’s cyst arise between the medial head of the gastrocnemius and the semimembranosus muscles. They are posterior to the
Statical Analysis
Statically the effect of Hirudotherapy in Bakers Cyst is Proven by before and After the Hirudotherapy and investigation (USG).
| S.No. | Quantity of Fluid in Bakers Cyst | Size of Bakers Cyst | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before Treatment | After Treatment | Before Treatment | After Treatment | |||||||||||
| 1 | 40 ml | Nil | 46 X 34 X 37 mm | 0 | ||||||||||
| 2 | 38 ml | Nil | 44 X 33 X 36 mm | 0 | ||||||||||
| 3 | 34 ml | 3 ml | 40 X 31 X 29 mm | 4 X 6 X 3 mm | ||||||||||
| 4 | 39 ml | 5 ml | 45 X 34 X 36 mm | 6 X 7 X 5 mm | ||||||||||
| 5 | 31 ml | Nil | 38 X 29 X 24 mm | 0 | ||||||||||
| 6 | 26 ml | 6 ml | 40 X 31 X 29 mm | 7 X 7 X 6 mm | ||||||||||
| 7 | 29 ml | Nil | 37 X 26 X 23 mm | 0 |
| Minimum | 26.00 | 0.0000 |
|---|---|---|
| 25% Percentile | 28.25 | 0.0000 |
| Median | 32.50 | 1.500 |
| 75% Percentile | 38.25 | 5.250 |
| Maximum | 39.00 | 6.000 |
| Mean | 32.83 | 2.333 |
| Std. Deviation | 5.115 | 2.733 |
| Std. Error | 2.088 | 1.116 |
| Lower 95% CI | 27.47 | -0.5343 |
| Upper 95% CI | 38.20 | 5.201 |
| P value | < 0.0001 | |
| Are means signif. different? (P < 0.05) | Yes | |
| One- or two-tailed P value? | Two-tailed | |
| t, df | t=12.40 df=5 |
| P value | < 0.0001 |
|---|---|
| Are means signif. different? (P < 0.05) | Yes |
| One- or two-tailed P value? | Two-tailed |
| t, df | t=22.70 df=6 |
| Number of pairs | 7 |
| Mean of differences | 39.00 |
| 95% confidence interval | 34.80 to 43.20 |
| R squared | 0.9885 |
From the above analysis, it is quite evident and clear that there is strong statistical significant difference in respect of fluid quantity and the length of cyst before and after the treatment given to patients.
Conclusion
Baker’s cyst is common clinical entity which is easily diagnosed clinically and can be well confirmed radiologically by ultrasonography and MRI. The cystic leasion exteds between the tendons of semimembranosus and the medical head of gastrocnemius remain the key to the diagnosis. From this entirely new study it has been observed that Hirudotherapy played and significant role in the treatment of baker’s cyst by way of draining the local joint inflammation due to natural anti-inflammatory and natural steroids present in the leech saliva. It is also presumed that the bioactive substances present in the leech saliva regulate the vascular blood flow smoothly without any occlusion due to Hirudin, Calin, Hirustasin, & Bdellins like substances present in leech saliva. The bioactive substances like Hyaluronidas in presumed to be responsible for resolution of the morbid material (Galeez Aklat) at the joint space and hereby Hirudotherapy plays a paramount role in the treatment of baker’s cyst.
References
-
Langsfeld M, Matteson B, Johnson W, Wascher D, Goodnough J, et al. (1997) Baker's cysts mimicking the symptoms of deep vein thrombosis: diagnosis with venous duplex scanning. J Vasc Surg 25(4): 658- 662.
-
Curl WW (1996) Popliteal cysts: historical background and current knowledge. J Am Acad Orthop Surg 4(3): 129-133.
-
Bui-Mansfield LT, Youngberg RA. Baker cyst. Available from: http://www.emedicine. com/radio/topic72.htm
-
Hubbard, MJ, Hildebrand, BA, Battafarano, MM, Battafarano DF (2018) Common Soft Tissue Musculoskeletal Pain Disorders. Primary care 45 (2): 289-303.
-
Herman AM, Marzo JM (2014) Popliteal cysts: a current review. Orthopedics 37(8): 678-684.
-
Foris, LA; Bhimji, SS (2018) Cyst Baker. PMID 28613525 (https://www.ncbi.nlm.nih.gov/pubmed/2861 3525).
-
Kane D, Balint PV, Gibney R, Bresnihan B, Sturrock RD (2004) Differential diagnosis of calf pain with musculoskeletal ultrasound imaging. Ann Rheum Dis 63(1): 11-14.
-
Gompels BM, Darlington LG(1982) Evaluation of popliteal cysts and painful calves with ultrasonography: comparison with arthrography. Ann Rheum Dis 41(4): 355-359.
-
Torreggiani WC, Al-Ismail K, Munk PL, Roche C, Keogh C, et al. (2002)The imaging spectrum of Baker's (popliteal) cysts. Clin Radiol 57(8): 681-691.
-
Ferri Fred F (2015) Ferri's Clinical Advisor 2016 E- Book: 5 Books in 1 Elsevier Health Sciences.pp: 200. ISBN 9780323378222.
-
Fielding JR, Franklin PD, Kustan J(1991) Popliteal cysts: a reassessment using magnetic resonance imaging. Skeletal Radiol 20(6): 433-435.
-
Robertson CM, Robertson RF, Strazerri JC (2003) Proximal dissection of a popliteal cyst with sciatic nerve compression. Orthopedics 26(12): 1231-1232.
-
Sansone V, de Ponti A, Paluello GM, del Maschio A (1995) Popliteal cysts and associated disorders of the knee. Critical review with MR imaging. Int Orthop 19(5): 275-259.
-
Andonopoulos AP, Yarmenitis S, Sfountouris H, Siamplis D, Zervas C, et al. (1995) Baker's cyst in rheumatoid arthritis: an ultrasonographic study with a high resolution technique. Clin Exp Rheumatol 13(5): 633-636.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review