Gastric Gastro Intestinal Stromal Tumour
Laparoscopic surgery was performed on 46-year-old women with a Gastric gastro intestinal stromal tumour (GIST). Laparoscopic gastric surgeries (LGS) may be an appropriate new, minimally-invasive operation for gastric myogenic tumours. Laparoscopic surgery can be applied to the traditional surgical principles with equal efficacy in selected patients.
Introduction
Leiomyomas constitute 2.5% of all resected neoplasms of the stomach. They are usually asymptomatic, but may present as mucosal ulceration. Leiomyomas (GIST) are the most common benign tumours of the stomach found at autopsy. They can on occasion enlarge and undergo central necrosis, which may result in massive upper gastrointestinal bleeding.
Case History
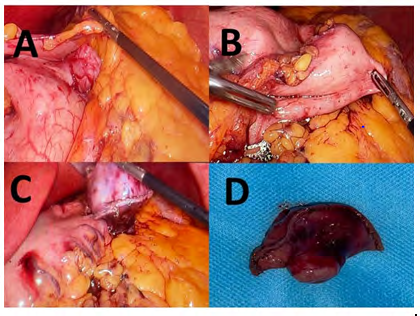
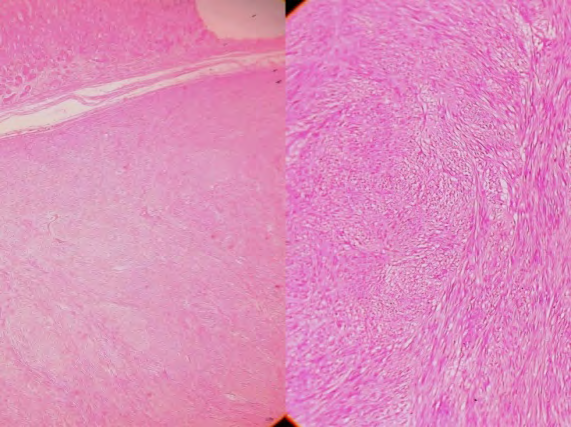
A 46-year-old female was admitted for upper abdominal pain, post prandial fullness and occasional vomiting for 2 weeks. She was given a course of Proton pump inhibitors which did not improve her symptoms. All routine blood investigations were normal. Ultrasound of the abdomen was normal. Contrast enhanced computed tomography (CECT) of the abdomen showed a well-defined exophytic heterogeneously enhancing soft tissue density lesion from the posterior wall body of stomach of size 3.4 x 2 cms extending to the level the tail of pancreas (Figure 1). Esophagogastroduodenoscopy was normal and there was only an extraneous impression. A provisional diagnosis of leiomyoma arising from stomach wall was made. A supraumbilical 10mm, Three5 mm ports and one 12mm ports were made (Figure 2) At laparoscopy the tumour was visualised after opening the gastrocolic omentum (Figure 3). Short gastric vessels were divided and greater curvature was freed up to OG junction. The mass on the posterior wall of the stomach was resected with 2cm wedge of normal stomach tissue using staplers (Figure 4). The specimen was retrieved through an endo bag. The patient tolerated the procedure well. There was no dye leak at the suture line (gastrograffin study which was performed on post-operative day 2. Pathological examination of the specimen revealed well-differentiated smooth muscle cells without malignant features suggesting a benign leiomyoma (Figure 4). The specimen was tested for IHC markers CD-117 which was positive.


Discussion
Sarcomatous tumors of the gastro intestinal tract occur commonly at 50 years of age. Syndromes associated with gastro intestinal stromal tumours (GIST) include Carney triad, Neurofibromatosis -1, Von Hippel Lindau [1] Gastric leiomyoma mostly presents as small solitary tumours that are asymptomatic [2, 3]. Clinical symptoms are vague abdominal pain and bleeding (malena or frank hematemesis). They are smooth and well circumscribed with occasional ulceration of the mucosa. The presenting symptoms, if any, are postprandial fullness and gastrointestinal bleeding. If a pedunculated mass is present in the antral region, then it can present as gastro duodenal intussusception. Complications associated with this disease are intra peritoneal discharge secondary to mucosal ulceration, gastric volvulus, gastric tumoral torsion and haemorrhage. GISTs are usually diagnosed as an incidental finding at gastroscopy or barium upper gastrointestinal series. Modalities used for evaluation are upper endoscopy [4] with finding of smooth appearing round submucosal tumor occasionally containing area of central ulceration. Endoscopic ultrasound (EUS) directed fine needle aspiration also help is tissue diagnosis of GIST. Microscopically, it presents as crossed groups of extensive fusiform smooth muscle cells, with eosinophilic cytoplasm, no myofibrilla and rare mitotic action, which characterize its favourable character [5]. Differentiation of benign leiomyomas from the malignant leiomyosarcomas is also important. Other than this immunohistochemistry markers are C-Kit proto-oncogene (CD-117) which is expressed in 95 % of these tumors. CD -34 with positive in 60 % of GIST.
Recommended treatment is wedge resection for tumors smaller than 4 cm in diameter. Resection with wide margins is required for tumors larger than 4 cm. The suitable most treatment for GIST is surgical resection. It can be performed by open method or laparoscopically. First laparoscopic resection was performed in 1992. The conventional resection was laparotomy and resection. However, pedunculated GIST can be resected with endoscopic polypectomy or enucleation [6, 7]. Methods which can be used for resection are laparoscopic wedge resection of gastric wall with the use of endo-stapling guns (per-operative ultrasound guidance or endoscopy can be used for confirmation), laparoscopic intra-gastric resection with endo-cutter (for tumors not suitable for wedge resection), laparoscopic gastrostomy and resection under endoscopic guidance. Or a combination of all approaches [8]. Laparoscopic transgastric resection of a gastric submucosal tumor near esophagogastric junction with concomitant sleeve gastrectomy has been documented by Alshlwi, et al. [9] for a patient with morbid obesity. Berindoague in a series of laparoscopic resections for GIST showed a 9% conversion rate (due to large tumour size),delayed gastric emptying in 3 patients and an average hospital stay of 6 days [10] Gastric tumors with primary endoluminal components necessitate the use of intraoperative endoscopy for localization during laparoscopy. If most of the tumour is located endoluminally or it is close to the gastroesophageal junction, laparoscopic transgastric approach will aid resection. This technique requires placement of laparoscopic trocars through the gastric wall with insufflation of the gastric lumen. The tumor can be enucleated and primary closure of the mucosa is performed.
The location of the tumor is another important factor in deciding on the most appropriate minimally invasive surgical approach. Ngyuen in his series had surgical approaches that included thoracoscopic enucleation, laparoscopic enucleation, transgastric enucleation, and laparoscopic gastric wedge resection. There was one conversion and the mean length of hospital stay was 2.6 ± 2.0 days [11]. The minimal access choice, depend on the site of the tumour. Right thoracoscopy works for tumors located in the oesophagus, as it can then be easily mobilized and enucleated. Laparoscopic
enucleation is preferred to wedge resection for tumours near the OG junction, pylorus and the lesser curvature to prevent narrowing of the lumen. A combined laparoscopic and thoracoscopic oesophago gastrectomy approach is suitable for large tumours (>4 cm), or if the tumour involves the mucosa layer. Laparoscopic distal gastrectomy is the preferred choice for large tumours located close to the pylorus. A Roux-en-Y reconstruction should be done if post- operative endoscopy shows a narrowed lumen. Laparoscopic wedge resection is done for tumours close to the antrum avoiding inadvertent narrowing of the gastric lumen (require placement of either a bougie or an endoscope).
Wu, et al. compared 15 patients of laparoscopy-assisted versus 13 patients who underwent open resection of gastrointestinal stromal tumours and found no significant differences between the 2 groups with regard to operative time or complications but the former was associated with less postoperative pain and faster recovery [12]. Matthews, et al. also documented less hospital stay [13]. In a case- control study, Lee found that laparoscopic surgery can be performed safely with improved recovery, regardless of the tumour size or location [14].
Conclusion
Gastric GISTs are amenable to minimal access procedures that involve laparoscopy alone or a combination of laparoscopy with endoscopic intragastric resections. The results in trained hands are comparable to open resection, with the main benefit being a decreased hospital stay.
References
-
Branham MT, Pellicer M, Campoy E, Palma M, Correa A, et al. (2014) Epigenetic alterations in a gastric leiomyoma. Case Rep Gastrointest Med 2014: 371638.
-
Marshall SF (1975) Symposium of surgery of digestive tract. Gastric tumors other than carcinoma. Surg Clin North Am 35: 693-697.
-
Townsend CM, Daniel Beauchamp R, Mark Evers B, Mattox KL (2017) Sabiston textbook of surgery. 20th (Edn.), WB Saunders, Elsevier-Health Sciences Division, Philadelphia.
-
Nonaka S, Oda I, Saito Y (2019) Diagnosis and treatment of superficial gastric neoplasms. In Clinical Gastrointestinal Endoscopy pp: 349-366
-
Lin Y, Chiu N, Li A, Liu C, Chou Y, et al. (2017) Unusual gastric tumors and tumor-like lesions: Radiological with pathological correlation and literature review. World J Gastroenterol 23(14): 2493-2504.
-
Gurbuz AT, Peetz ME (1997) Brief clinical report. Surg Endosc 11**:** 285-286.
-
Osama S (2019) Oncology and Cancer Case Reports Gastric Leiomyoma and its Management: A Rare Occurrence. Oncol Cancer Case Rep 5: 2.
-
Taniguchi E, Kamiike W, Yamanishi H, Ito T, Nezu R, et al. (1997) Laparoscopic intragastric surgery for gastric leiomyoma. SurgEndosc 11(3)**:** 287-289.
-
Alshlwi S, Elbahrawy A, Alamri H, Najmeh S, Aggarwal R, et al. (2017) Laparoscopic transgastric resection of a gastric submucosal tumor near esophagogastric junction with concomitant sleeve gastrectomy: a video case report. Obes surg 27(2): 552-553
-
Berindoague R, Targarona EM, Feliu X, Artigas V, Balagué C, et al. (2006) Laparoscopic resection of clinically suspected gastric stromal tumors. Surg Innov 13(4): 231-237.
-
Nguyen NT, Shapiro C, Massomi H, Laugenour K, Elliott C, et al. (2011) Laparoscopic enucleation or wedge resection of benign gastric pathology: analysis of 44 consecutive cases. Am Surg 77(10): 1390-1394.
-
Wu JM, Yang CY, Wang MY (2010) Gasless laparoscopy assisted versus open resection for gastrointestinal stromal tumors of the upper stomach: preliminary results. J Laparoendosc Adv Surg Tech A 20(9): 725-729.
-
Matthews BD, Walsh RM, Kercher KW (2002) Laparoscopic vs open resection of gastric stromal tumors. Surg Endose 16(5): 803-807.
-
Lee HH, Hur H, Jung H, Park CH, Jeon HM, et al. (2010) Laparoscopic wedge resection for gastric submucosal tumors: a size-location matched case-control study. J Am Coll Surg.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review