Juvenile Giant Fibroadenoma Vs Phyllodes Tumor Know the Difference in a 14 Years Old Woman Case Report
Fibroadenoma is the most common benign fibroepithelial lesion of the breast in young women, accounting for around 90% of solid lesions of the gland in adolescence. However, juvenile giant fibroadenoma is a rare breast condition that occurs in women under 18 years of age. Due to the similarity of the characteristics of juvenile giant fibroadenoma and phyllodes tumor, both lesions characterized by rapid growth, it is important to establish the differential diagnosis of both pathologies when one of them is suspected, in order to guarantee the most appropriate therapeutic attitude to follow. A 14-year-old woman with no family or personal history of interest, who consulted due to a clinical picture characterized by breast asymmetry secondary to progressive growth of the left breast of 5 months of evolution. An ultrasound-guided core needle biopsy was performed that reported giant juvenile fibroadenoma. Lumpectomy was performed. Histopathological diagnosis compatible with juvenile giant fibroadenoma of the left breast. Based on our case and on the reviewed bibliography, we recommend an early differential diagnosis, as well as an accurate one, and surgical treatment of cases of juvenile giant fibroadenoma. The surgical tactics and technique depend on the age at the time of diagnosis, the clinical and imaging characteristics of the mammary gland and the tumor, as well as the wishes of the patient in question.
Introduction
Fibroadenoma is the most common benign fibroepithelial lesion of the breast in young women, accounting for around 90% of solid lesions of the gland in adolescence. However, juvenile giant fibroadenoma (JFAG) is a rare condition of the mammary gland, presented in women under 18 years of age, characterized by size ≥5 cm, weight ≥500 g, or occupancy of ≥80% of the mammary gland, with an incidence of 0.5-2% of all fibroadenomas [1, 2].
In contrast, phyllodes tumor (PT) is a rare fibroepithelial neoplasm, generally benign, which constitutes 1%
of primary breast tumors, which presents a biphasic structure with an epithelial and stromal component, being classified by the WHO according to its characteristics histological (degree of stromal cellularity, atypia, mitotic index, infiltrative behavior of the edges and the presence of heterologous components) in: benign, intermediate and malignant, where each of these groups will have a different behavior in terms of prognosis, recurrences and the therapeutic attitude [1, 3].
Due to the similarity of the clinical characteristics of JFAG and PT, in addition to the evolution characterized by their rapid growth, it is important to establish the differential diagnosis of both pathologies when one of them is suspected, in order to guarantee the best therapeutic attitude. Next, we present our clinical case.
Case Presentation
A 14-year-old woman with no family or personal history of interest, who consulted due to a clinical picture characterized by breast asymmetry secondary to progressive growth of the left breast of 5 months evolution, which is why she performed a breast ultrasound study and in view of the findings, is referred to our center.
Clinical Findings
Female in good general condition. Asymmetrical breasts at the expense of a left mammary nodule that covers the entire breast, regular edges, hard consistency, mobile, painless, approximately 20 cm in diameter, not attached to deep planes (Figure 1); Right breast with solid nodular lesions, regular edges, hard consistency, mobile, painless, approximately 2 cm in diameter, located towards R10 and at the retroareolar level, intact bilateral nipple-areola complexes without secretions. Rest of physical examination without alterations (Figure 1).

Timeline
The patient comes for evaluation at the beginning of September 2021, performs a control ultrasound approximately 2 weeks after the first study, reflecting a considerable increase in the size of the lesion in a short period of time (approximately 10 cm). The biopsy is performed on 09/21/2021, obtaining results a week later. Surgery is scheduled, being carried out in mid-November 2021, due to institutional problems.
Diagnostic Evaluation
A breast ultrasound (US) was performed (08/26/2021) which reflected asymmetric breasts, appreciating the larger volume on the left, with a predominantly fibroglandular pattern, occupying the four quadrants, approximately 20 cm in size, corresponding to PT vs. JFAG; while on the right, solid nodules measuring 17.1 x 8.5 mm were observed towards the upper outer quadrant and 11.5 x 4.5 mm at the retroareolar level.
An ultrasound study was repeated on 09/09/2021, which reported asymmetric breasts, dominating the left breast in size at the expense of LOE, covering almost the entire breast, eco-mixed, with significant vascularization on color Doppler, lobulated, defined, approximate size 15, 4 x 28.8 cm, cataloging a BIRADS IV-B, while in the right breast was found an oval lesion with defined borders, lobulated, hypoechoic, solid, measuring 18.5 x 10.7 mm in R10 and a hypoechoic area at the retroareolar level of 22.3 x 15mm. The patient was scheduled for an ultrasound-guided core needle biopsy (CNB) of the left breast lesion, reported on the histopathological study as a JFAG of the left breast.
Therapeutic Intervention
The patient was scheduled for lumpectomy of the left breast and deferred excisional biopsy of the nodules of the contralateral breast with ultrasound-guided marking with preoperative methylene blue for exact location of the lesions, through an arcuate incision following the areola bilaterally (Figure 2) was obtained as an operative finding in the left breast: a solid tumor with a fibrous appearance of approximately 30 cm in diameter with abundant vascularization of approximately 1 kg (Figure 3); while in the right breast a solid nodular lesion of approximately 2.5 cm in diameter, fibrous appearance, was obtained at the retroareolar level, and a solid nodular lesion of approximately 3 cm in diameter, fibrous appearance, at the R10 level. A Jackson Pratt drain directed to the resection bed was used in the left breast, while a Penrose drain was used in the right breast (Figures 2 & 3).


Follow-Up and Results
Patient whose post-surgical evolution was favorable, being discharged after 24 hours of hospital observation. We’re not complications in her evolution and the right and left drains were removed on the fifth and tenth postoperative day, respectively. The histopathological diagnosis reported juvenile fibroadenoma of the left breast measuring 14 x 12.5 x 6.4 cm, with a smooth external surface, with vascular areas and scant adhering adipose content of 800 g (Figure 4), in addition to diffuse fibrosis of the right mammary nodules, with milk ducts and lobules of normal histological appearance (Figure 4).
Discussion
JFAG is a rare subtype of fibroadenoma that accounts for 0.5-2% of all fibroadenomas. Most authors accept this characteristic clinical form due to the presentation before the age of 20 of a generally single tumor with a diameter between 10 cm and 20 cm, of rapid growth that sometimes presents with vascular stasis and skin alterations, which leads clinically to think of a PT or sometimes in a sarcoma. The malignancy of the JFAG is rare, less than 0.2%, however, due to its characteristics, it causes a significant state of anxiety in the patient, not only due to the fear that it is a more serious pathology, but also due to the change in the physical appearance produced in these young women [2].
PT also grows rapidly, usually acquiring a large size, with characteristics similar to fibroadenoma. It constitutes 1% of primary breast tumors. In 1838, Johannes Müller, described this tumor under the name of “cystosarcoma phyllodes”, due to its fleshy appearance and its leaf-shaped projections. Subsequently, Lee, in 1931, described a case of metastatic behavior, which currently it has the ability to metastasize in up to 9% of reported cases. The average age of presentation is 40-45 years, however, it is the most frequent malignant breast tumor in adolescents [1, 3, 4] hence the importance of establishing a differential diagnosis from the beginning.
Multiple studies have reported an initial histopathological diagnosis of fibroadenomas in patients under 18 years of age and, after definitive resection, a diagnosis of malignant PT was obtained [4, 5, 6, 7]. For this reason, in lesions with particular behaviors (such as considerable increase in size in short periods of time, multilobulated lesions or with increased vascularity) we consider that an intraoperative biopsy should be performed in order to avoid false negatives, which was not performed in our case due to the lack of an pathological anatomy service in our institution.
JFAG is the main cause of unilateral macromastia and breast asymmetry in adolescents. On physical examination, it manifests as hard or elastic nodules, well defined, highly mobile, not fixed to the skin or to deep planes, and generally not painful. Traditionally, the etiology has been related to increased estrogen levels or increased hormone receptors [8, 9]. On the other hand, PTs appear as rounded tumors, generally single, well circumscribed and lobulated, of variable sizes, from a few centimeters to well-defined, painless, mobile lesions that occupy the entire breast [1, 4, 5, 6, 7].
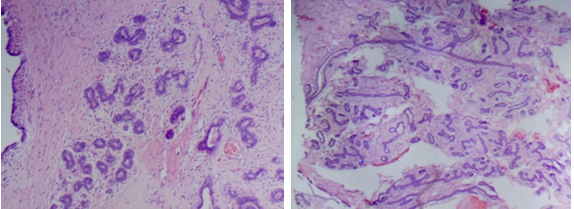
The microscopic appearance of the fibroadenoma is quite typical: proliferation of the double canalicular epithelium is observed, which is elongated and deformed by the simultaneous growth of the loose connective component, designing stellar, linear or arciform figures. On the other hand, PTs are mixed (stromal and epithelial), with an intracanalicular growth pattern reminiscent of fibroadenoma, but with a spindle-shaped and more cellular mesenchymal component, which forms lobulated leaf- like masses (foliaceous) and are covered by bistratified epithelium with a basal layer of myoepithelial cells and an external luminal layer, being classified depending on their stromal cellularity, mitotic activity, and cellular atypia into benign, borderline, and malignant (cystosarcoma phyllodes) [1, 2, 3, 4, 5, 6, 7].
Ultrasound is the first diagnostic test performed, appearing as a solid, ovoid or polylobulated, hypoechoic, homogeneous, regular nodule with well-defined borders. With a good clinical examination and ultrasound, the diagnosis can be made in most cases. CNB is indicated in cases of discrepancy between clinical manifestations and imaging studies, in patients belonging to risk groups or those with a surgical indication who reject intervention, especially to confirm the benignity of the lesion and rule out associated pathologies [10]. Generally, fibroadenomas do not require surgical treatment, however, surgery constitutes the angular treatment in both pathologies (JFAG and PT), due to the local alteration that it causes and the cancerophobia that occurs in patients [11].
Current recommendations for the diagnosis of JFAG do not provide homogeneous information on its management, and there are various surgical options. The chosen technique should preserve healthy breast tissue and the nipple-areola complex when possible. In general, the procedure of choice will be lumpectomy without reconstruction with deferred biopsy, which usually presents good aesthetic results with practically no post-surgical complications [3, 12, 13, 14, 15] which was performed in our case (Figure 5).

Conclusion
Preservation of healthy developing breast tissue is of the utmost importance to achieve good cosmetic results. In addition, despite the large size of the JFAG, healthy tissue that is usually underestimated tends to occupy the space left by the tumor, reducing the need for reconstruction, since, if performed immediately, the risk of presenting worse cosmetic results is considerably elderly.
Based on the consulted bibliography and our experience, an early and precise differential diagnosis, with surgical removal of the JFAG, would be the most appropriate management of these patients. The surgical tactics and technique depend on the age at the time of diagnosis, the clinical and imaging characteristics of the mammary gland and the tumor, and even the wishes of the patient.
Ethical Considerations
The authors declare that they have followed the protocols and guidelines of their work center, maintaining the confidentiality of the patient’s data. In the same way, informed consent has been obtained from the legal representative of the patient for the publication of the clinical case.
Availity of Data
The data of this clinical case are found in the “Dr. Ángel Larralde” General National Hospital, located in the city of Naguanagua, Carabobo state, Venezuela.
Conflict of Interests
The authors declare that they have no conflict of interest.
Authors Contribution
JP and AJBE developed the idea; JP conducted the literature search and drafted the manuscript. AJBE
documented the process. AJBE, MC, AFBS and CG made corrections to the initial manuscript and carried out the final revision, contributing with their experience and the incorporation of intellectual analysis. All the authors carried out a bibliographic review and contributed to the intervention and follow-up of the patient, as well as provided criticism prior to submission and approved the final report.
References
-
Dominguez F, Ballester J, de Castro Gonzalo (2017) Breast Surgery Clinical guidelines of the Spanish Association of Surgeons. In: 2nd (Edn.), Aran, Madrid, Spain, pp: 653.
-
Sanchez M, Crespo J, Vivas C (2021) Juvenile giant fibroadenoma and reconstruction surgery: report of a case and review of the bibliography. Rev Senol Patol Mamar 35(4): 316-319.
-
Chavez M, Ziegler G, Montes J (2021) Phyllodes tumor: report of a case treated with extreme oncoplastic surgery and review of the literature. Rev Senol Patol Mamar, pp: 1-5.
-
Espuelas S, Nicolau P, Fabrego B, Alcantara R, Vazquez I, et al. (2020) Multidisciplinary approach to a malignant phyllodes tumor of the breast in a 16-year-old woman. Rev Senol Patol Mamar 33(2): 72-75.
-
Makar G, Makar M, Ghobrial J, Bush K, Gruner RA, et al. (2020) Malignant Phyllodes Tumor in an Adolescent Female: A Rare Case Report and Review of the Literature. Case Rep Oncol Med pp: 1989452.
-
Faridi S, Siddiqui B, Ahmad S, Aslam M (2018) Progression of Fibroadenoma to Malignant Phyllodes Tumour in a 14-Year Female. J Coll Physicians Surg Pak 28(1): 69-71.
-
Anand P, Sarin N, Butti A, Singh S (2018) Malignant Phyllodes tumor in a young female: A Case Report. Gulf J Oncolog 1(27): 64-69.
-
Du F, Dong R, Zeng A, Liu Z, Yu N, et al. (2020) Surgical management of giant juvenile fibroadenoma with skin reducing tumor resection and immediate breast reconstruction: A single-center experience. J Surg Oncol 121(3): 441-446.
-
Baral S, Gyawali M, Thapa N, Chhetri R, Dahal P (2020) Giant juvenile fibroadenoma in an adolescent female: A case report. Clin Case Rep 8(12): 3489-3493.
-
Basara AI, Balci P (2021) Fibroadenomas: a multidisciplinary review of the variants. Clin Imaging 71: 83-100.
-
Islam S, Saroop S, Bheem V, Naraynsingh V (2019) Largest giant juvenile fibroadenoma of the breast. BMJ Case Rep 12(1): e227277.
-
Jategaonkar PA, Jetegaonkar SP, Yadav SP (2018) Super- Giant Juvenile Breast Fibroadenoma: World’s First Case. J Coll Physicians Surg Pak 28(3): 257-258.
-
Garza LO, Diaz MV, Paz SM, Rodriguez AJ, Apodaca RI (2018) Fibroadenoma gigante juvenil: reporte de un caso. Ginecol obstet Mex 86(9): 616-620.
-
Celik SU, Besli CD, Yetiskin E, Ergun E, Percinel S (2017) Giant juvenile fibroadenoma of the breast: a clinical case. Juvenile giant fibroadenoma of the breast: presentation of a clinical case. Arch Argent Pediatric 115(6): 428-431.
-
Mohd C, Norjazliney A, Abdul Rashid N (2017) A case report of juvenile giant fibroadenoma of the breast: How common?. Ci Ji Yi Xue Za Zhi 29(3): 177-179.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review