A Case of Brachial Plexus Schwannoma Presenting as a Cystic Neck Swelling
Schwannomas are benign tumours arising from Schwann cells of the neural sheath. They are rarely seen to arise from the brachial plexus. Brachial plexus schwannomas present as a swelling over lateral neck, supraclavicular region or axilla. Symptoms may include pain, sensory changes, weakness etc. Around 5% of these schwannomas may turn malignant. Although rare, cystic neck swellings can be due to cystic degeneration of a schwannoma. A preoperative evaluation is of utmost importance and in cases of neck swellings which are producing symptoms, a pre-operative MRI should be done to reach the diagnosis before taking the patient in the OT. Presented is a case of lateral neck swelling with mild tingling sensation over arm of the same side.
Introduction
Peripheral nerve tumours are rare and mostly benign and can be divided into nerve sheath and non-nerve sheath tumours. Schwannomas are well circumscribed, slow- growing benign tumors that are derived from Schwann cells in the nerve sheath. These mostly occur in the head and neck region (25% of all schwannomas) in the cranial nerves and the sympathetic chain with relative sparing of the brachial plexus (5% of all schwannomas) [1]. The male to female ratio in peripheral schwannomas is 1:1, average age of the cases being 47 years [2]. Most schwannomas are sporadic and some are associated with NF2, schwannomatosis or Carney’s complex etc. Their cut surface shows a tan yellow colour, sometimes with areas of haemorrhage and they often undergo cystic and degenerative change [3]. Microscopically, a surrounding capsule is present and fascicles of Schwann cells that have spindle cell morphology with areas of nuclear palisading forming parallel nuclear arrays or Verocay bodies. Brachial plexus Schwannoma is uncommon and it is even rarer for it to undergo cystic degeneration and present as a cystic lateral neck swelling. We report such a case of a 38 year-old woman who came with a history of a slow growing lateral neck swelling.
A 38 year-old female presented with complaint of a gradually growing swelling over right side of neck since 4 years which was associated with tingling sensation down the right arm. The patient was apparently alright 4 years ago when she first noticed a swelling over the right side of neck. It was insidious in onset and very gradually progressing in size. It was roughly 1cm x 1cm to begin with and gradually grew to a size of 4cm x 4cm now. There were no associated pain or tingling sensation initially; however she has now developed mild tingling sensation down her right arm till the fingertips of thumb and index fingers, especially on applying pressure over the swelling.
There is no history of fever, cough or cold. No history of trauma to the site, no similar swelling anywhere else in the body. She has a past history of tuberculous lymphadenitis wherein her right cervical lymph nodes were enlarged and excised for histopathological confirmation and further treatment (6 months of anti-tubercular treatment was taken). Her family history is unremarkable.
On examination, the patient was averagely built and well- nourished. No lymphadenopathy was noticed on general examination. Oro-dental hygiene was good with no signs of any dental, oral or ear-nose-throat infection. Her vitals and basic blood investigations were within normal range. On inspection, a 4x4 cm spherical, smooth surfaced swelling with no nodularity, no skin changes (except for a small scar from previous lymph node excision) noted in the posterior triangle of the neck on the right side (Figure 1). On palpation the inspectory findings were confirmed, the swelling being tense, cystic, non-tender and smooth surfaced with no nodularity. It was mobile in anteroposterior direction with restricted mobility in the mediolateral direction, indicating some attachment to an underlying structure. Skin could be pinched separately. There was no local rise of temperature. No pulsations were noted and no bruit was heard on auscultation. However, on applying pressure over the swelling, tingling could be felt over the right arm upto the fingertips of her thumb and index fingers.

An ultrasound was done which showed a multi-septate cystic collection. On the basis of past history, examination and sonographic findings, a provisional diagnosis of tuberculous cold abscess was made and hence an MRI or a CT scan was not performed. Decision was taken to excise the swelling.
Intra-operatively, the cyst was noted to arise from a nerve trunk in the brachial plexus (Figure 2). Decision was taken to enucleate the cyst instead of excising it completely to prevent nerve injury. The cyst contained clear, straw- coloured fluid and the cyst wall was sent for histopathological examination. A drain was placed and wound closed in layers. Post-operatively, there was little tingling down the right arm till the fingertips of thumb and index finger as before but no motor deficits.

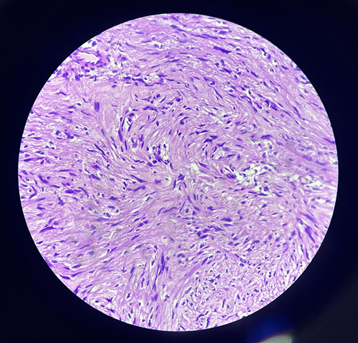
Histopathological examination showed spindle-shaped cells arranged in interlacing fascicles with nuclear palisading suggestive of neurilemmoma (schwannoma) (Figure 3). On follow-up after a week, the drain was removed and on examination there was very mild residual tingling and no motor deficits.
Discussion
Brachial plexus tumours account to <5% tumours in the upper extremity [4]. Of the peripheral nerve tumours, schwannomas are the second commonest after neurofibromas [5]. Although schwannomas are known to undergo cystic degeneration, it is a rare occurrence. Brachial plexus nerve sheath tumours, though uncommon, can be considered as a differential diagnosis in case of lateral neck and supraclavicular swellings [6].
Symptoms arise due to direct nerve invasion, infiltration of surrounding tissue or by local mass effect [7]. For cystic swellings of the neck, a sonography or CT is recommended to confirm the cystic nature of the swelling and to note the vascularity of the tumour [8]. Non- vascular tumours are relatively safe for fine needle aspiration cytology (FNAC) to be done to differentiate between malignant and benign neoplasms. Although, when neurological symptoms are present it is recommended to get an MRI done. In the case reported above, we notice how an MRI could have given the diagnosis pre-operatively and there wouldn’t have been an intra-operative surprise but given her past history of tuberculous lymphadenitis and sonographical evidence of a cystic swelling, it was provisionally diagnosed as a cold abscess and hence an MRI or a CT scan was not done. FNAC and biopsy can cause neurological deficits- transient nerve paresis may occur even when benign tumours are carefully dissected. In case of neurological symptoms or a progressively growing mass with a suspicion of malignancy, it is recommended to excise the tumour completely [9, 10, 11, 12]. Enucleation of schwannomas is almost always possible and should be done to preserve the nerve sheath and prevent neurological deficits. Post-operatively temporary, mild neurological deficits are expected.
Conclusion
Schwannomas are a rare occurrence in the brachial plexus where they may present as a supraclavicular or a lateral neck mass. When there are signs of neurological deficits with a slow growing history of the mass, a schwannoma can be suspected. It may undergo cystic degeneration and present as a multi-septate cystic mass on sonography. An MRI would help reach the diagnosis pre-operatively. It is recommended to enucleate a schwannoma and preserve the nerve sheath to prevent neurological deficits.
Conflict of Interest
None.
References
-
Kumar A, Akhtar S (2011) Schwannoma of brachial plexus. Indian J Surg 73(1): 80-81.
-
Majumder A, Ahuja A, Chauhan DS, Paliwal P, Bhardwaj M (2021) A clinicopathological study of peripheral schwannomas. Med Pharm Rep 94(2): 191-196.
-
Hilton DA, Hanemann CO (2014) Schwannomas and their pathogenesis. Brain Pathol 24(3): 205-220.
-
Donner TR, Voorhies RM, Kline DG (1994) Neural sheath tumors of major nerves. J Neurosurg 81(3): 362-373.
-
Ahn KM, Lee HK, Lee KD (2002) A case of neurilemmoma of the brachial plexus. J Korean Otolaryngol 8: 733-735.
-
Vučemilo L, Lajtman Z, Mihalj J, Plašćak J, Mahović Lakušić D, et al. (2018) Brachial Plexus Schwannoma - Case Report and Literature Review. Acta Clin Croat 57(2): 366-371.
-
Mrugala MM, Batchelor TT, Plotkin SR (2005) Peripheral and cranial nerve sheath tumors. Curr Opin Neurol 18(5): 604-610.
-
Kho JP, Prepageran N (2018) Huge brachial plexus schwannoma, masking as a cystic neck mass. AME Case Rep 2: 41.
-
Huang JH, Zaghloul K, Zager EL (2004) surgical management of brachial plexus region tumors. Surg Neurol 61: 372-378.
-
Kumar A, Akhtar S (2011) Schwannoma of brachial plexus. Indian J Surg 73(1): 80-81.
-
Albert P, Patel J, Badawy K, Weissinger W, Brenner M, et al. (2017) Peripheral Nerve Schwannoma: A Review of Varying Clinical Presentations and Imaging Findings. J Foot Ankle Surg. 56(3): 632-637.
-
Addi Palle LR, Depa VGR, Shah K, Soto CJ, Aychilluhim BA, et al. (2023) Peripheral Schwannoma Presenting as a Retro-Malleolar Mass: A Case Report. Cureus 15(7): e42137.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review