Mandibular First Premolar with Unusual Root and Canal Variation Associated With Condensing Osteitis or Sclerosing Osteitis–A Rarest Case Report
The present article reports existence of severe root dilaceration (80-degree bend) and Vertucci’s type V root canal configuration in the mandibular first premolar which is rarely reported in the dental endodontic literature. In addition to this, development of a localized condensing osteitis involving the same tooth which is rarely reported till date is also presented. Condensing osteitis was accidentally detected following radiographic examination of the first premolar and this clinical condition usually involves the tooth with a long-standing pulpal infection and occurs as a result of body’s defence mechanism against the infection. This radiopaque jaw pathology represents a bone deposition phenomenon rather than a bone destruction, a reactionary process seen following an inflammatory process in the tooth.
Introduction
“Condensing Osteitis” also referred as “Sclerosing Osteitis” is the most common radiopaque lesion of the jaw bone characterised by asymptomatic, uniform localized area of radiopaque foci of dense bone, manifested as a sequela of dental infection and represents a reactive hyperplasia of osteoblasts. This condition can occur as a result of pulpal irritations such as a deep carious lesion or long-standing restorations [1, 2]. Therefore, this radiographic entity is referred as a pathosis-forming response to a chronic low- grade inflammatory stimulus. It is also called by various synonyms as ‘chronic focal sclerosing osteitis’ and ‘sclerosing osteitis.’ The prevalence of this radiopaque lesion is estimated as 4 to 7% in the general population and affecting mostly the mandibular region of about 91% of prevalence compared to just 9% of its occurrence in the maxillary region [1].
Condensing osteitis is most commonly encountered in young individuals with high tissue resistance and in females. Radiographically the size of the lesion usually varies from as small as of 1 mm to as big as of 22 mm. Even the shape of radiopaque mass varies and it exhibits round (32%), U shaped in 4% and irregular in 64% of cases [3]. The classical radiographic feature of this condition includes a uniform radiographic mass which is dense and opaque with well- defined margins seen adjacent to the root apex of the tooth. Loss of lamina dura and widening of periodontal ligament space is usually seen along with tooth having either carious lesions or large restorations, a crown or bridge, root canal therapy and a periodontal disease [4, 5].
Normally the mandibular first premolar has a single root with single canal, however variations in crown morphology as well as in root canal anatomy does exist in different ethnic population [6, 7, 8]. Compared to all other human teeth, mandibular first premolar poses great challenge during root canal treatment and is associated with high flare up and failure rates because of existence of variations in root canal anatomy [9]. Various investigators have given different root canal types based on different evaluation methods employed in their study. Vertucci’s root canal types classification (Table 1 & Figure 1) is one among those most commonly employed during root canal treatment of human teeth [10]. Existence of Vertucci’s type V root canal configuration in mandibular first premolars is rarely reported in the endodontic literature. Therefore, the purpose of this article is to present an occurrence of sclerosing osteitis or condensing osteitis involving the mandibular first premolar having Vertucci’s type V root canal configuration and severe root dilaceration which is not reported so far. Publications of this type of rare case reports give an insight to all dental practitioners including endodontists during root canal therapy involving mandibular first premolars about the existence of rare root canal types in these teeth.
| Types of Root Canal System in Mandibular First Premolar | Description |
|---|---|
| Type I | Single canal extends from pulp chamber to the apex |
| Type II | Two separate canals leave pulp chamber and join short of the apex to form one canal |
| Type III | One canal leaves pulp chamber and divides into two canals in the root, and finally merge into one and exist |
| Type IV | Two separate canals extend from pulp chamber to apex |
| Type V | One canal leaves pulp chamber, divides short of apex into two |
| Type VI | Two canals leave pulp chamber merge in the root and divide again short of apex to exit as two distinct canals |
| Type VII | One canal leaves pulp chamber, divides and then re-join in root and finally divides into two canals short of the apex |
| Type VIII | Three separate canals extend from pulp chamber to the apex |
Table 1: Vertucci’s Classification on Root Canal System Observed in Mandibular First Premolar Tooth [7].
![Figure 1: Schematic picture showing Vertucci’s different root canal system [7].](/fulltextimages/12401/fig_1.png)
Case Report
A 15-year-old female patient reported to a private dental clinic complaining of pain in the right lower back tooth region from past one week. Patient was moderately built and nourished with absence of systemic, metabolic disorders and syndromic diseases. On intra oral examination complete permanent dentition was observed. On further examination, dental caries was observed in the mandibular right first premolar. To assess the status of this tooth and its periapical information, patient was subjected to radiographic examination. On the radiograph, deep dental caries involving pulp tissue was evident in relation to the mandibular right first premolar. When the affected premolar was examined in detail a single wide root canal was observed and at the apical one third of the root it was bifurcated into two canals ending at the apex separately (Figure 2). There was loss of lamina dura and widening of the periodontal ligament space. Attached to the root apex, a radiopaque mass measuring 20 mm in size and was round in shape which was similar to the radiopacity of the adjacent alveolar bone (Figure 1). Apart from this no other peculiar radiographic findings were observed. Based on clinical features and radiographic findings the case was diagnosed as a localized condensing osteitis/sclerosing osteitis with severe root dilaceration involving mandibular first premolar and associated with Vertucci V root canal configuration (1-2) or (one canal leaves pulp chamber, divides short of apex into two). A treatment plan consisting of root canal treatment to the affected first premolar was decided and explained in detail to the patient and patient was scheduled for the appointment. Unfortunately, patient missed further appointments and hence root canal treatment was not completed.
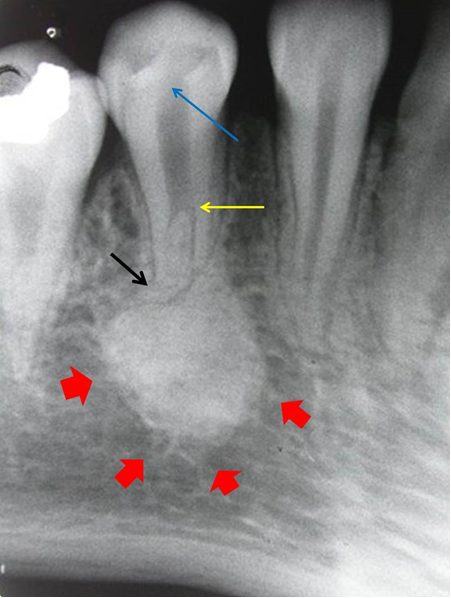
Figure 2: Radiograph showing mandibular right first premolar with carious lesion involving dental pulp (blue arrow), Vertucci’s Type V root canal configuration (1-2) (yellow arrow) and severe root dilaceration of 80-degree bend at the root apex (black arrow). A round shaped radiopaque dense mass measuring 20 mm size can be seen attached to the root apex (red arrows)
Discussion
Yeh HW, et al. [1] evaluated the frequency and distribution of mandibular condensing osteitis lesions among Taiwanese individuals (1098 patients) at the Dental department of Tri-Service General Hospital. They identified 75 lesions in 63 patients. The prevalence found was 5.7%, in that 10.7% cases were associated with teeth that had crowns and or bridges, 21.3% were associated with teeth having caries or restorations, 29.3% were associated with teeth which received root canal treatment, 12% cases of Condensing osteitis were associated with teeth with periodontal diseases and 26.7% cases were located in the tooth extraction area. There was increased predilection of condensing osteitis among females (65.5%) compared to males (34.7%). Only ten cases (13.3%) were detected in the premolar region and about 65 cases (86.7%) were identified in the molar area with the first molar region being the most common site of occurrence with condensing osteitis [1].
In differential diagnosis, all lesions which appear as periapical radiopaque mass should be considered during diagnosis of condensing osteitis [11, 12, 13, 14]. Idiopathic osteosclerosis is one such lesion which appears almost similar to condensing osteitis. Although an idiopathic sclerosis is a periapical radiopaque lesion, but this condition is not related to any pulpal pathology as compared to condensing osteitis which generally develops at the root apex of the tooth with untreated caries, long standing pulpal infection or deep restorations and occlusal trauma [11, 14]. The most commonly involved tooth with condensing osteitis is the permanent mandibular first molar followed by second molar. This can be attributed to the finding that the mandibular first molar is the first tooth which erupts in the oral cavity and hence seen with early involvement of increased caries attack and also due to heavy fillings which finally cause pulpal inflammation and necrosis [2, 3, 4]. A study performed in Taiwanese population showed that among the 187 radiopaque lesions, 53.5% were categorized as idiopathic sclerosis and 46.5% were condensing osteitis [1]. Idiopathic osteosclerosis is a developmental anomaly and presents as a normal anatomic bone variation formed during early bone development. In this condition, the tooth is asymptomatic, intact and vital. Other condition that should be considered in differential diagnosis is the cementoblastoma [12, 13]. This lesion represents an uncommon benign odontogenic neoplasm of the jaw and the typical characteristic feature of this condition is presence of radiopaque mass with a peripheral radiolucent rim when observed on radiographs. This radiolucent rim is not seen either in idiopathic osteosclerosis or condensing osteitis. Other conditions that need to be ruled out in differentiating condensing osteitis are hypercementosis, osteoblastoma and cemento-osseous dysplasia [1, 2].
Occurrence of condensing osteitis is reported less common in the maxilla compared to mandible which may be due to lower cortical thickness and abundant irrigation seen in the maxillary bone. The exact etiology behind the occurrence of condensing osteitis is many and the patho- physiology shows chronic irritation of the root canal in which low-virulence micro-organisms present in the residual necrotic pulp following appropriate endodontic treatment gradually induce the bone immune response. This type of sclerotic bone is most often seen with relatively longstanding or low intensity infections [1, 2, 3, 4]. Radiographically sclerosing osteitis show variations in size from small to large size and with different shapes. In the case presented here, it measured about 20 mm in size with round shape.
Regarding treatment of condensing osteitis, the management includes a thorough root canal treatment, following which the radiopacity gradually subsides or decrease in size. If the root canal therapy is not performed well or incomplete then the lesion will not resolve because study done by Yeh HW, et al. [1] have shown that most cases of condensing osteitis were associated with teeth with inadequate root canal therapy. In addition to this, if the size of the lesion is big, then complete surgical removal of the altered pathological bone along with infected tooth is the recommended treatment of choice. However, it is also stated that in large sized condensing osteitis cases, the radiological appearance remains even after extraction of the involved tooth. In the case presented here, unfortunately follow up records could not be obtained as the patient missed for further appointments.
Another clinically significant information that should be remembered concerning condensing osteitis is with bone biopsies taken which in turn are associated with clinical implications of being invasive procedures, that can lead to vertical and horizontal bone loss. This may require immediate or further surgical procedures for bone regeneration and rehabilitation. Moreover, in the premolar and molar regions of the mandible the risk of nerve damage must be considered when performing a bone biopsy [11].
The root canal system in human teeth is more complex and canals may branch, divide and rejoin taking various pathways to the apex [15, 16, 17, 18, 19]. Vertucci FJ [10] investigated numerous complex canal systems and identified eight pulp canal configurations. Some degree of dental anatomic variations can be observed in different races and ethnic groups with Asian populations exhibiting widest variations in coronal shape, external root form and internal canal space morphology [20, 21, 22, 23, 24, 25, 26].
Mandibular first premolar shows variations in root canal anatomy and configurations including variations in number and shapes [17, 20, 22, 24, 26]. Jain A, et al [9] performed an invitro study among Gujarati, Indian population to investigate the root canal morphology of mandibular first premolars. Authors found about 17.39% of Vertucci’s V canal system among the 138 extracted teeth examined. Dou, et al. [17] studied 178 extracted teeth belonging to Chinese population and found 99.4% of single-rooted first premolars along with type I canal system. Habib AA, et al. [19] conducted a study in Syria by examining 95 extracted first premolars and found about 17.9% of two canals and remaining 82.1% of first premolars with single canals in these teeth. Therefore, it is highly essential to have a thorough knowledge about occurrence of variations in root canal morphology and canal configurations among different population to render appropriate root canal treatment [27, 28]. Root dilacerations are referred to any bend or curve seen in the entire length of the root and most commonly seen at the root apex [26]. Regarding first premolars in the mandible, the occurrence of root dilaceration is a rare entity. In the present case, the mandibular first premolar exhibited severe root dilaceration having a 80-degree bend at the root apex along with Vertucci’s type V canal system.
Conclusion
The root and canal anatomy of the mandibular first premolar most of the time varies and on radiographic examination, various pathologic lesions involving bone which may be either radiopaque or radiolucent are accidentally detected. Therefore, by presenting this interesting case report of a mandibular first premolar having multiple anatomic root canal variations and pathology, author concludes that clinicians should be aware of such uncommon occurrence of localized condensing osteitis and different root canal morphology in order to render appropriate holistic care.
References
-
Yeh HW, Chen CY, Chen PH, Chiang MT, Chiu KC, et al. (2015) Frequency and distribution of mandibular condensing osteitis lesions in a Taiwanese population. J Dent Sci 10: 291-295.
-
Gupta S, Dutta S, Baby A, Langthasa M (2023) Condensing Osteitis – A review and case report. Asian Pac J Health Sci 10(2): 69-72.
-
Alimohammadi M, Hadian H, Mousavi J, Aryana M, Tabatabaei SR (2023) Frequency of condensing osteitis in the apexes of teeth with deep caries and large restorations in panoramic radiographs of patients at Sari dental school. J Maxandaran Uni Med Sci 33(223): 172-178.
-
Pedro R, Jose M, Ana D, Joao R, Eduardo G, et al. (2019) Condensing osteitis in the diagnosis consultation at Egas Moniz University clinic. A nn Med 51(1supply): 129.
-
Hayek E, Maalouf E, Nassar J, AbiLamaa F, Aoun G (2023) Idiopathic osteosclerosis and condensing osteitis in a sample of the Lebanese population: A digital panoramic based study. Med Arch 77(5): 396-399.
-
Nagaveni NB (2023) Prevalence of two rooted mandibular first premolars in Indian population. J Surg Anesth 1(1): 1-3.
-
Nagaveni NB, Ashwini KS (2023) Bifurcated mandibular second premolars: Report of unusual root anomaly (supernumerary root) – A case series. J Dent Oral Health 10: 1-7.
-
Nagaveni NB, Umashankara KV, Radhika NB, Mohan M. (2015) Molarization of the mandibular second premolar in an Indian patient: Report of a rare case. Ann Bioanthropol 3: 33-35.
-
Jain A, Bahuguna R (2011) Root canal morphology of mandibular first premolar in a Gujarati population – an In vitro study. Dent Res J (Isfahan) 8(3): 118-122.
-
Vertucci FJ (1984) Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 58(5): 589-599.
-
Mishra G, Bernisha R , Bhogte SA, Chitra P (2024) Idiopathic Osteosclerosis in Orthodontic Patients: A Report of Two Cases. Cureus.16(2): e53426.
-
Suhasini GP, Wadhwan V, Garg N (2020) Cementoblastoma of a primary molar: A rare pediatric occurrence. J Oral Maxillofac Pathol 24(3): 548-553.
-
Mohammadi F, Aminishakib P, Niknami M, Razi Avarzamani A, Derakhshan S (2018) Benign Cementoblastoma Involving Deciduous and Permanent Mandibular Molars: A Case Report. Iran J Med Sci 43(6): 664-667.
-
Pathak J, Hosalkar RM, Sidana S, Swain N, Patel S (2019) Benign cementoblastoma involving left deciduous first molar: A case report and review of literature. J Oral Maxillofac Pathol 23(3): 422-428.
-
Nagaveni NB, Umashankar KV, Radhika NB (2012) A retrospective analysis of accessory roots in mandibular molars of Indian paediatric patients. Int J Dent Anthropol 20: 38-46.
-
Nagaveni NB, Umashankara KV (2009) Radix entomolaris in permanent mandibular first molars: Case reports and literature review. Gen Dent 57 (3): e24-29.
-
Dou L, Li D, Yang D, Yin Tang, Deqin Yang (2017) Root anatomy and canal morphology of mandibular first premolars in a Chinese population. Scientific Rep 7: 750.
-
Nagaveni NB, Umashankar KV, Radhika NB, Satish TS (2011) Third root (Radix entomolaris) in permanent mandibular first molars in pediatric patients – an endodontic challenge. J Oral Health Commun Dent 5: 49- 51.
-
Habib AA, Kalaji MN, Al Sasad TJ, Al Jawfi KA (2015) Root canal configurations of the first and second mandibular premolars in the population of north Syria. J Taibah Uni Med Sci 10(4): 391-395.
-
Nagaveni NB, Umashankara KV (2012) Radix entomolaris and paramolaris in children – A review of the literature. J Indian Soc Pedod Prev Dent 30(2): 94-102.
-
Velmurugan N, Sandhya R (2009) Root canal morphology of mandibular first premolar in an Indian population: a laboratory study. Int Endod J 42(1): 54-58.
-
Nagaveni NB (2023) Bilateral “molarization” of the mandibular second premolars in association with unusual dental variation – Report of a rarest case. Glob J Res Dent Sci 3(5): 4-6.
-
Rahimi S, Shahi S, Yayari H, Manafi H, Eskandarzadeh N (2007) Root canal configuration of mandibular first and second premolars in an Iranian population. J Dent Res Dent Clin Dent Prospect 1(2): 59-64.
-
Nagaveni NB (2023) A rare combination of tooth agenesis in association with anomalous supernumerary tooth: Report of a rare case. Oral Health Dent 6(1): 18- 21.
-
Sandhya R, Velmurugan N, Kandaswamy D (2010) Assessment of root canal morphology of mandibular first premolars in the Indian population using spiral computed tomography: an invitro study. Indian J Dent Res 21(2): 169-173.
-
Nagaveni NB (2024) Permanent mandibular second premolar with unusual morphology in association with other dental variations – Report of a rarest case. J Dent Res Treat 1(2): 1-8.
-
Evren OK, Altunsoy M, Nur BG, Aglarci OS, Colak M, et al. (2014) A cone-beam computed tomography study of root canal morphology of maxillary and mandibular premolars in a Turkish population. Acta Odontol Scand 72(8): 701-706.
-
Slowey R (1979) Root canal anatomy: road map to successful endodontics. Dent Clin North Am 23: 555- 573.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review