Outcomes of Surgical Revascularization in Trans-Atlantic Society Consensus (TASC II) Type C & D Aortoiliac Occlusive Disease
Introduction: Aortoiliac occlusive disease is a disabling illness. This study was conducted on the patients of Trans-Atlantic Society Consensus (TASC II) type C & D aortoiliac occlusive disease. Open surgical revascularization in the form of aortofemoral and aorto-bifemoral bypass grafting was done and the demography of patients of AIOD, the efficacy and outcomes of open surgical bypass in the patients of TASC II, type C & D aortoiliac occlusive disease was studied. Methods: in this study, total of 52 patients were revascularized and were observed for various parameters thoroughly throughout the course of diagnosis, preoperative, intra-operative and postoperative phase and until 6 months of follow-up. The demographics, clinical characteristics of the patients, co-morbid conditions, type of aorto-iliac occlusive disease (AIOD), the surgical procedure conducted and the outcomes of surgery in terms of limb salvageability, healing of ulcer, relief of claudication and graft patency were observed. Results: 50 (96.16%) out of 52 patients were males, with a mean age of presentation 55.01 + 8.58 years. 47 (90.38%) were smokers, 43 (82.69%) had hypertension, 17 (32.69%) had diabetes, 11 (21.15%) had CAD, 12 (23.07%) had COPD, 22 (42.30%) had type C and 30 (57.69%) patients had type D disease. Aorto-bifemoral bypass grafting was done in 42 (80.76%) . Mean duration of ICU stay was 1.9 days, 6 (11.53%) patients expired postoperatively. The graft patency and limb salvageability were 100% and 96.15% respectively during 1st, 3rd and 6th months of follow-up with complete healing of ulcers in 21 (91.30%) patients by the end of 6 months. Conclusion: Surgical revascularization is an important, high yielding, life changing intervention which serves as a boon for the patients with extensive or advanced aortoiliac disease. The surgery has excellent outcomes in terms of graft patency as well as limb salvageability.
Abbreviations
AIOD: AortoIliac Occlusive Disease; AFBG: Aorto-femoral Bypass grafting; ABFBG: Aorto-bifemoral Bypass, CLTI: Chronic Limb Threatening Ischemia; TASC: Trans- Atlantic Society Consensus; CAS: Carotid Artery Stenosis, RAS: Renal Artery Stenosis.
Introduction
Aortoiliac Occlusive Disease, otherwise known as leriche’ syndrome is a debilitating and painful condition and can result in serious complications like chronic limb ischemia (CLI), gangrene and tissue loss [1, 2, 3, 4, 5]. Which ultimately results in painful loss of limb function and severely affects the quality of life in patients.
Trans-Atlantic Society Consensus (TASC II) Type C and D aortoiliac occlusive disease can still be managed surgically with good long term graft patency, limb salvageability and is associated with increased longevity and quality of life in patients [6]. We performed open surgical bypass in 52 patients with Trans-Atlantic Society Consensus (TASC II) Type C & D aortoiliac occlusive disease and followed them from preoperative period to 6 months post-surgery.
Aims & Objectives
This study aimed to evaluate the demographic and clinical characteristics of the patients with aortoiliac occlusive disease (AIOD), Trans-Atlantic Society Consensus (TASC II) Type C and D disease and the outcomes of the surgical revascularization in terms of Limb salvage, healing of ulcers, relief of intermittent claudication, Graft patency at 1, 3 and 6 months, and patient’s satisfaction.
Methodology
Patients with intermittent claudication, ulceration, paraesthesia, or chronic limb ischemia were evaluated for possible aorto-iliac occlusive disease (AIOD) using CT angiography and USG doppler findings after thorough clinical history, clinical as well as doppler examination. Patients with TASC II type C & D AIOD were selected for further evaluation. Patients underwent thorough clinical examination, cardiac profile, lipid profile, diabetic work-up, blood investigations, pulmonary function test, chest x-rays, and thyroid profile if necessary. Echocardiography and coronary angiography were done in all the patients with suspected ASCVD (Atherosclerotic cardiovascular disease). Patients were advised treatment of comorbid conditions and proper optimization prior to surgery. All 52 patients who were selected out of total 70 patients, were revascularized through appropriate surgical procedure (aorto-femoral/ aorto- bifemoral bypass grafting) using suitable graft material (PTFE or Dacron). If necessary, patients were advised for coronary artery bypass grafting before aortic bypass. Revascularized patients were monitored postoperatively and during follow- up periods at 1, 3 and 6 months for relief of symptoms, healing of ulcer, graft patency, and limb salvageability.
Inclusion and Exclusion Criteria
Inclusion Criteria: All patients > 18 years of age, undergoing surgical revascularization for Trans-Atlantic Society Consensus (TASC II) category C & D Aorto-Iliac Occlusive Disease (AIOD). Exclusion Criteria
- Patients not giving consent for study
- Patients who have undergone revascularization surgery earlier.
- ACSVD/CAD requiring surgical treatment.
- Patient not fit for general anaesthesia.
Preoperative Work Up
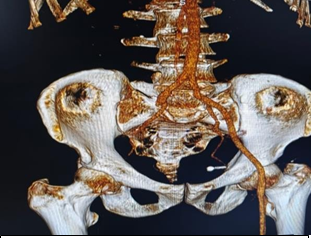
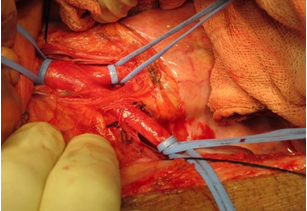
Patients with suspected aortoiliac occlusive disease (AIOD) were examined and diagnosed using CT angiography. Patients with Type C and D lesions on CT angiography were planned for surgical revascularization and were included in the study after taking the informed consent. Blood investigations, including HbA1c and lipid profile, were conducted. Patients with AIOD were also investigated for diseases like coronary artery disease (CAD/CVD), carotid artery stenosis (CAS), renal artery stenosis (RAS), Diabetes Mellitus, Dyslipidaemia, Hypertension, and Chronic Obstructive Pulmonary Disease. Preoperative optimization was done, and cardiac angiography and echocardiography were conducted for patients over 40 years. Patients were advised to quit smoking at least 4 weeks prior to the surgery and undergo chest physiotherapy (Figures 1 & 2).

Surgery details
After completing all the pre-operative work-up, choice of proposed surgical procedure, consent taking, pre- anaesthetic optimization, site marking and taking expected critical events into consideration, we further proceeded with the pre-oxygenation and induction of General Anaesthesia to the patient. The patients were operated in supine position, exposure was invariably done from nipples to mid-distal thighs. All patients were given Injection Piperacillin 4000 mg + Tazobactam 500 mg combination through intravenous route after inducing anaesthesia and before making incision.
A vertical midline incision was made and the bowel was mobilised anti-clockwise. Retroperitoneum was exposed infracolically, duodenum mobilised towards the right and dissection done until aorta, its lumbar branches, both renal arteries, inferior mesenteric artery (IMA) and infrarenal aorta were exposed and clearly identified. Bilateral common iliac arteries (CIA) were exposed and checked for suitability for clamping. Distal abdominal aorta, B/L common iliac arteries (CIAs) were then dissected and looped. A groin incision was given bilaterally or unilaterally depending upon whether it is a unilateral or a bilateral bypass.
Through the groin incision, the ipsilateral common femoral artery (CFA), superficial femoral artery (SFA), profunda femoris artery (PFA) were identified, checked for suitability for clamping and are looped.
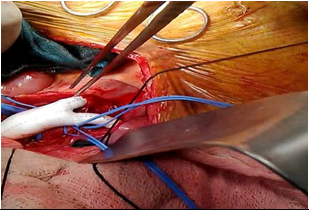
Injection Heparin given as IV bolus in the standard dose of 100 mg/kg body weight and clamp was applied to infrarenal abdominal aorta. Infrarenal abdominal aorta and B/L common iliac arteries (CIAs) were opened one by one and assessed for good antegrade and retrograde flow, if necessary endarterectomy was performed (Figure 3). The graft was put in place and patch plasty of CIA with abdominal aorta was done if required. An end to end or end to side anastomosis could be done between the distal abdominal aorta and the vascular graft depending upon the patency of aortic bifurcation. Aorta and graft were anastomosed and the graft was then carried to B/L groins through retroperitoneal tunnels. The anastomosis was done between distal end of the graft and common femoral artery, unilaterally or bilaterally depending upon whether the surgery being done is a unilateral bypass or a bilateral bypass (Figure 4).
After de-clamping, once again the flow was assessed proximally, distally and within the graft with the help of intra- op microvascular Ultrasound Doppler (Hadeco DVM-4500 bi-directional doppler volume flowmeter). Haemostasis achieved, and single semi-open drain was placed in the pelvic cavity. Abdomen was closed in layers and soon after that, the groin incisions were also closed and sterile dressing was applied.
Post-Operative Care: Broad spectrum antibiotics along with painkillers and supportive medications were given to all patients. All patients were kept on IV bolus weight adjusted doses of unfractionated heparin for 72 hrs and bridged with warfarin until target INR of 2 to 3 was achieved. The patients were extubated only when they were completely awake with good respiratory effort and power. All patients were kept on single antiplatelet drug along with statins. The patients were shifted out of the ICU after removing all invasive lines. Duration of ICU stay was recorded. Complications like wound infection, seroma formation, etc. were recorded.
Follow Up
Follow Up was conducted at 1, 3 & 6 months and the Patients were monitored for following parameters during follow up.
- Peripheral pulses
- Paraesthesia
- Requirement of amputation after revascularization surgery.
- Patient satisfaction based upon our customised Questionnaire.
Observations and Results
Age Distribution
Maximum number of the patients, i.e. 29 patients (55.7%) out of total 52 patients, were in the age group 51- 60, while the age of the patients ranged from 28 years to 76 years. The Mean Age of the patients who underwent surgical revascularization in our study was 55.01+ 8.58 years.
Gender Distribution
Majority of the patients were males (50 patients out of total 52 patients i.e. 96.16%), while two of the patients (3.84%) were females. Co-morbidities: Out of all the studied patients, majority of them (43 out of 52 patients i.e. 82.69%) were hypertensive, 17 patients (32.69%) were found to be diabetic, coronary artery disease and COPD were present in 11 patients (21.15%) and 12 patients (23.07%), respectively. Smoking- Forty-seven (47) patients (90.3%) out of total 52 patients were chronic cigarette/bidi smokers while only five patients (9.61%) were non-smokers. The most common complaint was Intermittent Claudication i.e. in all 52 (100%) patients. Paraesthesia was seen in 41 patients (78.84%), rest pain in 27 patients (51.92%), and Ulceration was present in 25 patients (48.07%). TASC II (Trans-Atlantic Society Consensus) Type of disease- Twenty-two patients (42.30%) had type C disease and 30 patients (57.69%) had type D aortoiliac disease.
Among all the patients, 42 patients (80.76%) had lesions suitable for Aorto-Bifemoral bypass grafting (ABFBG), while Aorto-femoral bypass grafting (AFBG) was done in only 10 patients (19.23%). Graft Material Used: Dacron Vascular graft was the most commonly used graft i.e. in 44 patients (84.60%) while PTFE was used in only 8 patients (15.38%). ICU Stay: The patients were kept in the ICU for minimum of 1 day to maximum for 4 days, the mean duration of ICU stay was 1.9 days. Most of the patients i.e. 24 patients (46.15%) were kept in the ICU for 2 days (Table 1).
| Intra-operative Complication | No. of Patients (%), N= 52 |
|---|---|
| Excessive Bleeding | 2 (3.84%) |
| Bowel Injury | 1 (1.92%) |
| Retroperitoneal Hematoma | 2 (3.84%) |
Table 1: Intra-operative Complications.
Re-Exploration after the first surgery: One of our patients (1.92%) suffered bowel ischemia following surgery for which he was re-operated on the second day and an ileostomy was made after resecting the gangrenous bowel segment. In one of our patients (1.92%), there was graft ex-plantation due to deep wound infection and debridement along with the redo surgery was done (Table 2).
| Wound complication | No. of Patients (%) , N= 52 |
|---|---|
| No complication / Normal healing | 35 (67.30%) |
| Erythema | 5 (9.61%) |
| Serous discharge | 4 (7.69%) |
| Seroma Formation | 3 (5.76%) |
| Deep Wound Infection | 3 (5.76%) |
| Gangrene | 2 (3.84%) |
Table 2: Wound related Complications.
| Post-Operative Complication | No. of Patients (%), N= 52 |
|---|---|
| Cerebrovascular Accident | 1 (1.92%) |
| Acute Kidney Injury | 4 (7.69%) |
| Myocardial Ischemia | 1 (1.92%) |
Table 3: Post-Operative Complication/Outcomes.
Out of all the 52 patients, there were 6 mortalities (11.53%) due to pre-existing comorbidities and/or the complications attributed to the revascularization surgery (Table 3).
Relief of Intermittent Claudication was seen in all 46 (100%) patients. Graft patency - All the Grafts were patent in all the 46 patients during 1month, 3months, and 6 months of follow-up period which was checked by Clinical hand-held doppler Scan (Minidop Hadeco ES 100 VX) i.e. graft patency (100%).
Healing of Ulcer: by the end of 6th month, 21 patients (91.30%) had their ulcers completely healed while 2 patients (8.69%) had satisfactory healing of their ulcers. Limb Salvage:
Among 46 patients eligible to follow up, 2 patients (4.34%) needed amputation, attributed to the already existing small vessel disease or distal obstruction. None were due to graft failure. 44 patients (95.65%) had their limbs salvaged.
Discussion
To the best of our knowledge, this is the first study of its kind from Indian subcontinent, based on Indian population and patient pool. All the 52 patients were thoroughly followed and observed for various parameters starting from the first OPD visit and day of admission. The Aorto-Iliac Occlusive Disease (AIOD) is a disease that generally affects the elderly population with its incidence and prevalence increasing with increasing age. Despite this, the vast majority if the patients of AIOD belong to the age group of 50-60 years. In our study, the mean age of patients with AIOD was 55.01+8.58 years, ranging from 28 years to 76 years, with majority of the patients i.e. 29 patients (55.7%) in the age group 51-60 years. This data was comparable to the study conducted by Shen C, et al. [7] who conducted a retrospective study from January 2016 to November 2019, reported the mean age of the patients undergoing endovascular revascularization for Type C & Type D AIOD was 65.1+10.7 years and the study conducted by Dong X, et al. [8] from January 2011 to December 2020 (mean age 62.2+7 years. AIOD affects both men and women equally. Allen AJ, et al. [9] in their study, found out that the population prevalence of AIOD in women was 40.3% while Diehm C, et al. [10] reported the prevalence of AIOD in women to be 58%. In our study, only two of the patients (3.84%) were females. Smoking by far and large has causal relationship with atherosclerosis and hence with CAD, CAS and PAD. The connection between smoking and PAD has been recognized since 1911, when Norgren L, et al. [11] reported that IC was three-times more common among smokers than among non-smokers.
Berger JS, et al. [12] in their study on “Modifiable risk factor burden and prevalence of peripheral artery disease in different vascular territories”, stated that the smokers had an increased risk of PAD with an odds ratio of 2.06. In our study, 47 patients (90.3%) were either chronic smokers (>10 years) or the chronic smokers who had quit smoking within 1 year of surgery. Both of these kinds of patients were considered as smokers in our study. The number of non-smokers was just 5, (9.61%). The prevalence of hypertension was maximum. Among all the 52 patients, 43 patients (82.69%) were hypertensive, which is consistent with what Olin JW [13] stated in his work, that the prevalence of hypertension in the patients with PAD was 50-92%. In his study, Heidrich H [14] observed that 57.9% of the patients with PAD had Hypertension. This difference could be due to the late presentation of patients to opt for the surgical treatment and the fact that patients who are chosen for surgical management of AIOD, generally have advanced disease. Diabetes mellitus is a rather common comorbid illness in the patients of AIOD. In our study, 17 patients (32.69%) were found to be diabetic. This data is comparable to the study by Senarslan DA, et al. [15] who observed the prevalence of diabetes to be 44.4%. Also, Krankenberg H, et al. [16] observed the prevalence of DM in patients of AIOD in their study, to be 27%. In our study, we observed concurrently existing CAD (not requiring surgical management), in 11 patients (21.15%) of total patients.
Similarly, Senarslan DA, et al. [15] observed the prevalence of CAD to be 38.9% in their study. Liang HL, et al. [17] observed the prevalence of CAD in their Study on Endovascular management of AIOD, to be 33.3%. In our study, we observed the presence of a concurrent pulmonary disease (COPD) in 12 patients (23.07%). This data is comparable to the study conducted by Chen et al. [18] in 2019, in which they found out the presence of COPD in 39% of their patients. Heidrich H [14] in his study about the frequency of non-vascular accompanying diseases in the patients of PAD, found the prevalence of COPD to be 14.5% in the patients of peripheral artery disease. In our study, the presence of intermittent claudication was found to be in all 52 (100%) patients, compared to Gao Z, et al. [19] who demonstrated the presence of Intermittent Claudication (IC) in 82.92% of the patients with PAD. The rest pain in our study was present in 31 patients (59.61%) compared to 86.92% in the study by Gao Z, et al. [19]. The presence of Ulceration and gangrene was found to be in 27 patients (51.93%). Paraesthesia was noted in 42 patients (80.72%). The choice of the surgical procedure whether Aorto-bifemoral bypass surgery or the Aorto-femoral bypass surgery was made based upon the TASC II Type of the lesions in the patients with the help of clinical evaluation and CT angiography findings. As all of our patients were either of TASC Type C disease, 22 patients (42.30%), or TASC Type D disease 30 patients (57.69%), open surgical bypass was done in all these patients given its superior outcomes in these lesions compared to the endovascular procedures.
Most of our patients needed bilateral lower limb revascularization, i.e. 42 patients (80.76%), while the Aorto-unifemoral, also known as Aorto-Femoral Bypass Grafing (AFBG) was done in only 10 patients (19.23%). As per the literature as well, open Bypass is the most common surgical procedure performed in TASC Type C & D diseases. A systematic review by Jongkind V, et al. [20] observed that among 66 studies in their systematic review with 9319 patients of TASC Type C & D AIOD, 5875 patients (63.04%) were revascularized via open surgery.
Intra-operatively, in 2 patients (3.84%), there was excessive haemorrhage, for which the graft revision was done at the aortic end. Retroperitoneal hematoma was seen in 2 patients (3.84%), which was managed by packing and compression. Bowel injury occurred in 1 patient (1.92%) which was missed during the surgery and the patient was re-explored the next day for signs and symptoms of bowel perforation & peritonitis and ileostomy was made. The graft patency was assessed with the help of clinical examination, presence of distal pulses and hand held doppler examination (Minidop Hadeco ES 100VX), as well as Colour doppler sonography at 1, 3 and 6 months and was found to be 100% in all the 46 patients eligible for follow-up. The average graft patency as per literature is about 80-90% in 5 years and 76-85% in 10 years. In a multicentric, retrospective, observational cohort study by Piffaretti G, et al. [21] from January 2015 to December 2017, with over 713 patients, analysed the estimated graft patency rate after one year to be 96% and 94% after two years. In a meta-analysis by Indes J, et al. [22] from 1989 to 2010 with 5358 patients, 57 studies, the primary patency of open surgical bypass after 1 year was found to be 94.8% and was significantly higher than the endovascular bypass surgeries in which the primary graft patency after 1 year was 86%. The limb salvageability in our study was found to be 96.15% as only 2 patients (3.84%) had to go through major amputation after the surgery. This data is consistent with other studies. In a study by Piffaretti G, et al. [21] the limb salvageability by the end on 1 year was found to be 99% and by the end of 2 years, 98%. Another study by Indes J, et al. [22] observed the limb salvageability to be 95.7% after 1 year and 91.5% after 3 years and 91% at 5 years, in the patients who were revascularized using open surgical methods.
Conclusion
AortoIliac Occlusive Disease (AIOD) is a debilitating condition affecting patient’s quality of life and occupational opportunities. It is a component of Atherosclerotic Cardio- vascular disease (ASCVD) and is mainly seen in patients in their 50s and 60s. Treatment is challenging due to various vascular and non- vascular accompanying illnesses which needs to be addressed simultaneously. Surgical revascularization has proven to increase longevity and quality of life for advanced AIOD patients. Regular follow- up and drug therapy adherence are essential for long-term outcomes.
Limitations
Since our study was of a limited duration with a short follow up period, long term graft patency and limb salvageability could not be assessed beyond the period of 6 months.
Conflict of Interest: None.
References
-
Brown KN, Muco E, Gonzalez L (2024) Leriche Syndrome. StatPearls.
-
Frederick M, Newman J, Kohlwes J (2010) Leriche syndrome. J Gen Intern Med 25(10): 1102-1104.
-
Holmes D (2017) Critical limb ischaemia: artery repair. Nature 548(7668): S41.
-
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, et al. (2019) Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. European Journal of Vascular and Endovascular Surgery 58(1): S1-S109.
-
Tewksbury R, Pearch B, Redmond K, Harper J, Klein K, et al. (2014) Outcomes of infrapopliteal endoluminal intervention for transatlantic intersociety consensus C and D lesions in patients with critical limb ischaemia. ANZ J Surg 84(11): 866-870.
-
PAD (2000) Management of Peripheral Arterial Disease. TransAtlantic Inter-Society Consensus (TASC). Section D: chronic critical limb ischaemia. Eur J Vasc Endovasc Surg pp: 144-243.
-
Shen C, Zhang Y, Qu C, Fang J, Liu X, et al. (2020) Outcomes of Total Aortoiliac Revascularization for TASC-II C&D Lesion with Kissing Self-Expanding Covered Stents. Ann Vasc Surg 68: 434-441.
-
Dong X, Peng Z, Ren Y, Chen L, Sun T, et al. (2023) Endovascular treatment of aorto-iliacocclusive disease with TASC II C and D lesions: 10 year’s experience of clinical technique. BMC Cardiovasc Disord 23(1): 71.
-
Allen AJ, Russell D, Lombardi ME, Duchesneau ED, Agala CB, et al. (2022) Gender Disparities in Aortoiliac Revascularization in Patients with Aortoiliac Occlusive Disease. Ann Vasc Surg 86: 199-209.
-
Diehm C, Schuster A, Allenberg JR, Darius H, Haberl R, et al. (2004) High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: cross- sectional study. Atherosclerosis 172(1): 95-105.
-
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. (2007) Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg 45(1): S5-S67.
-
Berger JS, Hochman J, Lobach I, Adelman MA, Riles TS, et al. (2013) Modifiable risk factor burden and the prevalence of peripheral artery disease in different vascular territories. J Vasc Surg 58(3): 673-681.
-
Olin JW (2005) Hypertension and peripheral arterial disease. Vasc Med 10(3): 241-246.
-
Heidrich H (2004) Frequency of non-vascular accompanying diseases in patients with peripheral arterial disease. Vasa 33(3): 155-158.
-
Senarslan DA, Yildırım F, Bayram B, Kurdal AT, Tetik O (2023) Results of endovascular treatments of Trans- Atlantic Inter-Society Consensus C or D aortoiliac occlusive disease involving the aortic bifurcation. SAGE Open Med 11.
-
Krankenberg H, Schlüter M, Schwencke C, Walter D, Pascotto A, et al. (2009) Endovascular reconstruction of the aortic bifurcation in patients with Leriche syndrome. Clinical Research in Cardiology 98(10): 657-664.
-
Liang HL, Li MF, Hsiao CC, Wu CJ, Wu TH (2021) Endovascular management of aorto-iliac occlusive disease (Leriche syndrome). Journal of the Formosan Medical Association 120(7): 1485-1492.
-
Chen TW, Huang CY, Chen PL, Lee CY, Shih CC, et al. (2018) Endovascular and Hybrid Revascularization for Complicated Aorto-Iliac Occlusive Disease: Short-Term Results in Single Institute Experience. Acta Cardiol Sin 34(4): 313-320.
-
Gao Z, Yue Y, Zhang Y, Jiang W, Zhang Y, et al. (2023) Comparison of Clinical Outcomes of Endovascular Therapy and Hybrid Surgery in the Treatment of Trans- Atlantic Inter-Society Consensus II D Aortoiliac Occlusive Disease. Int J Gen Med 16: 2149-2156.
-
Jongkind V, Akkersdijk GJM, Yeung KK, Wisselink W (2010) A systematic review of endovascular treatment of extensive aortoiliac occlusive disease. J Vasc Surg 52(5): 1376-1383.
-
Piffaretti G, Fargion AT, Dorigo W, Pulli R, Gattuso A, et al. (2019) Outcomes From the Multicenter Italian Registry on Primary Endovascular Treatment of Aortoiliac Occlusive Disease. Journal of Endovascular Therapy 26(5): 623-632.
-
Indes JE, Pfaff MJ, Farrokhyar F, Brown H, Hashim P, et al. (2013) Clinical Outcomes of 5358 Patients Undergoing Direct Open Bypass or Endovascular Treatment for Aortoiliac Occlusive Disease: A Systematic Review and Meta-Analysis. Journal of Endovascular Therapy 20(4): 443-455.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review