Morphometric Evaluation of Hard Palate in Indian Male and Female Skulls
Introduction: The palate is an integral part of head that forms the floor of the nasal cavity and the roof of the oral cavity. The knowledge of morphology and morphometry of hard palate is important for anatomists, dentists, anthropologists, and forensic experts. The aim of the present study is to describe the morphology and morphometric variations of the hard palate as seen in Indian male and female skulls. The observations made in the present study were compared with those in earlier studies on skulls belonging to different races. Materials and Methods: The study sample consists of adult Indian human dried skulls. Intact skulls of known sex with obliterated spheno-occipital suture were included in the study. Skulls with obvious pathological malformations were excluded from the study. The measurements of hard palate were taken using digital vernier calipers. The length, width and depth of palate were noted in male and female skulls at different sites and compared. Results: In the present study we found that there are significant differences between male and female palatal dimensions. These can be deployed to compare with other population. The size of palate is larger in males group than females and the average difference in the palatal depth is significantly higher in males than females this simply reflect the greater overall breadth of male skull in any given ethnic group Conclusion: Morphologic and morphometric knowledge of hard palate is advantageous in many fields of medical science. The present study based on Indian population of known gender can be used to compare data with other population.
Introduction
The palate is an integral part of head that forms the floor of the nasal cavity and the roof of the oral cavity. It is divisible into two regions namely the hard palate in front and soft palate behind. The anterior two-third of the palate is formed by the palatal process of the maxillary bones while the posterior one-third is formed by the horizontal process of the palatine bones. The hard palate lies within the alveolar arch and is slightly arched from before backwards and from side to side. Posteriorly, the hard palate ends in a crescentric free margin which presents a middle backward projection, the posterior nasal spine [1]. Developmentally, hard palate consist of two parts namely, primitive palate and permanent or secondary palate. The primitive palate is formed by the fusion of the globular swelling of medial nasal process and maxillary process. In adults, the junction between primitive and permanent palate is represented by incisive fossa which may be altered in condition like cleft palate [2]. The traditional shape categories for palate shape are parabolic, hyperbolic, and elliptical. Human palates differ considerably both in size and curvature. The greatest changes in palate shape take place in very early childhood [3].
The knowledge of morphology of hard palate is important as it plays a major role in the passive articulation of speech. Restricted development of hard palate is one of the causes for a condition known as sleep apnoea syndrome which is characterized by difficulty in breathing while sleeping [4]. The knowledge of palatine index is important because high and narrow palate has been reportedly associated with many syndromes such as Apert syndrome, Turner’s syndrome, Marfan syndrome, Franceschetti-Teacher Collins syndrome.
Morphometry of the palate forms the fundamental basis for the treatment planning of orthodontic conditions such as orthognathic surgeries [5], maxillary dental implants, Hemimaxillectomy, Le Fort fracture management, cleft palate surgery and also useful for preoperative evaluation of patients with uvulopalatopharyngoplasty. Procedures such as nasopharyngoscopy and nasogastric intubation will need a precise knowledge of normal structure and dimensions of these regions for meticulous manipulation and better designing of instruments [6]. The palatine index is essential for fabricating complete maxillary dentures and in the reconstruction of the hard palate as a part of cleft reconstruction procedures. The circumference of upper anterior teeth is significantly affects the position and expression of the lip and the lower part of the face [7]. Since hard palate is preserved even in severe damages to skull it can be used for anthroplogical studies and also useful in sexual dimorphism [8]. Palate shape appears to be a useful indicator of ancestry from the human skull [3, 9, 10].
The aim of the present study is to describe the morphology and morphometric variations of the hard palate as seen in Indian male and female skulls. The observations made in the present study were compared with those in earlier studies on skulls belonging to different races.
Materials and Methods
The study sample consists of adult Indian human dried skulls. They were obtained from the Department of Human Anatomy and Department of Forensic Medicine, Kempegowda Institute of medical sciences Bengaluru. The skulls have been retrieved from bodies donated for purpose of research and teaching. The study does not involve animals or patients. Skulls with intact base, of known sex, with obliterated spheno-occipital suture were included in the study. Skulls with obvious pathological malformations and skulls of pediatric and neonatal age group were excluded from the study. The study has been in accordance to standard ethical protocol.
The measurements of hard palate were taken using digital vernier calipers. The measurements were recorded up to two decimal places. The following measurements were noted in male and female skulls (Figure 1).
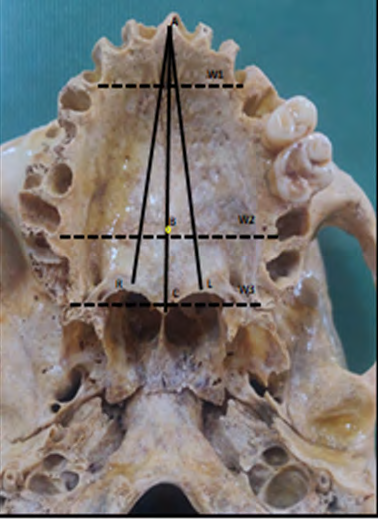
- Length of the hard palate was measured from the Orale to the Staphylion (AC). The orale is the point located between the two medial maxillary incisors on the median plane. Staphylion is the point on the posterior nasal spine where a straight line joining the deepest notches of the posterior margin of the palate cuts the midsagittal plane. The following sub lengths were also noted.
- AB-Maxillary length-from orale to cruciform suture
- BC-Palatine length- from cruciform suture to staphylion
- AR-Mid arch length on right side
- AL-Mid arch length on left side
- The width of the palate was measured from the inner borders of the sockets. The following widths were noted.
- W1-Intercanine distance
- W2-Inter second molar distance
- W3-width at posterior edge of palate
- The depth of hard palate was measured from intersection of transverse and median palatine planes to the plane of the palate curve [11].
Palatine Index: The Palatine index (PI) was calculated by Palatine width/ Palatine length X100.AC and W2 were used for length and width respectively. The PI was classified according to the Hassanali and Mwaniki method. Based on the PI measurements the palates were classified as
- Leptostaphyline is the narrow palate where the PI range was 79% or less.
- Mesostaphyline is the intermediate type where the PI range was 80-84.9%.
- Brachystaphyline is the wider palate where the PI range was 85% or more [12].
The measurements of the palatal arch dimensions were analyzed with statistical package for social science (spss, version 11) for production of means, standard deviation, z test, chi square test for palatine index and the Pearson’s coefficient of correlation between the recorded variable.
Results
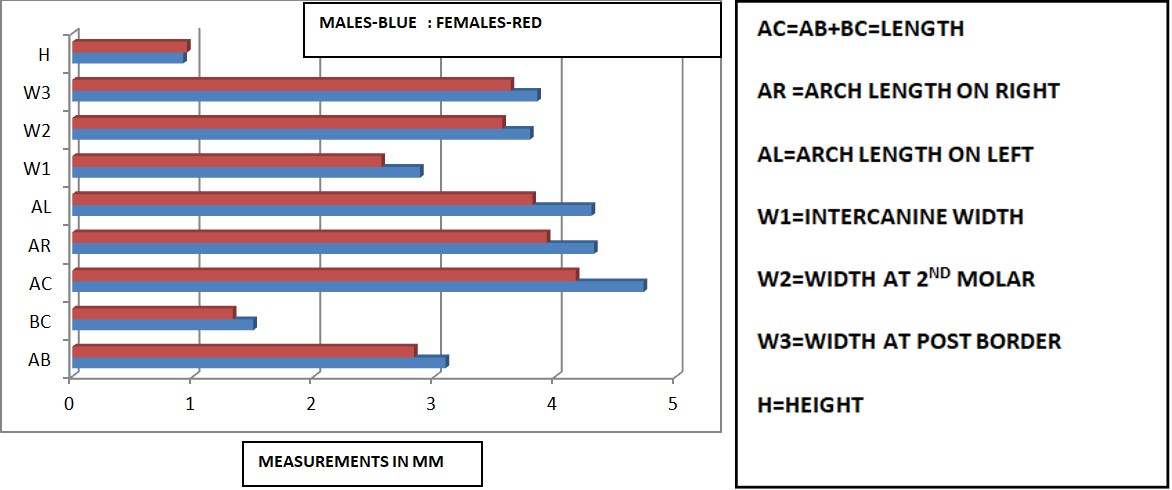
The measurements of the palatal arch dimensions were tabulated and analyzed with statistical package for social science for production of means, standard division, z– test, chi square and the Pearson’s coefficient of correlation between the recorded variable. In the present study a total of 60 adult skulls were analyzed out of which 44 belonged to males and 16 belonged to females. The results in male and female skulls are tabulated in (Tables 1 & 2) and (Figure 2).
We found that there were significant differences between male and female palatal dimensions. The size of palate was significantly longer and wider in males than females .The total length and intercanine width amongst palatal width was significantly higher in males than females(p<0.01) in given ethnic group (Indian). The standard deviation was also significantly higher in males. The arch lengths also slightly deferred on right and left sides being longer on the right side, though no significant differences were noted when sex was taken into consideration. The height also showed much variation in male skulls than in female skulls.
The palatine index was calculated and tabulated in males and in females. In the present study we found that the majority (46.67%) of skulls had narrow palate (Leptostaphyline) followed by brachystaphyline closely with 40%.When sex was taken into consideration males were significantly leptostaphyline while females were predominantly brachystaphyline (p<0.05).
| MALES (n=44) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| AB | BC | AC | AR | AL | W1 | W2 | W3 | H | |
| MEAN | 3.09 | 1.5 | 4.73 | 4.32 | 4.3 | 2.88 | 3.79 | 3.85 | 0.92 |
| MIN | 2.2 | 1.01 | 3.92 | 3.32 | 3.61 | 2.42 | 3.49 | 3.53 | 0.37 |
| MAX | 4.71 | 2.01 | 5.82 | 4.93 | 5.1 | 3.46 | 4.32 | 4.24 | 2.41 |
| SD | 0.53 | 0.32 | 0.56 | 0.42 | 0.43 | 0.25 | 0.21 | 0.21 | 0.55 |
| FEMALES (n=16) | |||||||||
| AB | BC | AC | AR | AL | W1 | W2 | W3 | H | |
| MEAN | 2.83 | 1.33 | 4.17 | 3.93 | 3.81 | 2.56 | 3.56 | 3.63 | 0.95 |
| MIN | 2.41 | 0.91 | 3.52 | 2.86 | 2.72 | 2.12 | 2.81 | 2.81 | 0.62 |
| MAX | 3.28 | 1.82 | 4.67 | 4.41 | 4.62 | 3.3 | 3.92 | 3.98 | 1.4 |
| SD | 0.31 | 0.28 | 0.38 | 0.51 | 0.51 | 0.36 | 0.35 | 0.36 | 0.28 |
| Total (n=60) | |||||||||
| AB | BC | AC | AR | AL | W1 | W2 | W3 | H | |
| MEAN | 2.96 | 1.415 | 4.45 | 4.125 | 4.055 | 2.72 | 3.675 | 3.74 | 0.935 |
| SD | 0.183848 | 0.120208 | 0.39598 | 0.275772 | 0.346482 | 0.226274 | 0.162635 | 0.155563 | 0.021213 |
Table 1: Measurements (in mm) of all variables in male and female skulls.
| Leptostaphyline | Mesostaphyline | Brachystaphyline | |
|---|---|---|---|
| Males | 55.00% | 6.67% | 23% |
| Females | 30% | 20% | 50% |
| Total | 46.67% | 13.33% | 40% |
Table 2: Palatine index in male and female skulls.
Discussion
Hard palate consist of two parts namely, primitive palate and permanent or secondary palate. The development of palate depends on various factors like swallowing movements of the tongue, downward and forward growth of the lower jaw and tongue complex, providing more space above the tongue for the palatal processes, straightening of the cranial base as the result of growth of the neural mass, establishing the mechanical environment for the palatal processes to swing upward. This along with cessation of mesenchyme cell proliferation hours before palatal processes swing increases volume hydration of extracellular matrix and medial edge epithelium covering the free edges of the palatal processes. Finally this epithelium undergoes apoptosis immediately prior to fusion and there is development of a temporary glycoprotein coat, enabling adhesion between epithelial cells of the two opposing palatal processes [13].
The greatest changes in growth of the palate shape take place in very early childhood. They found that the hard palate grows very rapidly until the age of 18 months, where it has reached 80% of its adult mature size. After age 11 the shape of the palate stays about the same [4]. The arch lengths also slightly deferred on right and left sides though no significant differences were noted when sex was taken into consideration. This negates the role of tongue movement played during post natal development. The palatine index varied significantly in male and female skulls thereby highlighting the role of chromosomal, hormonal factors and bone growth factors.
The traditional shape categories for palate shape are parabolic, hyperbolic, and elliptical.3 Hooton was one of the earliest to notice the differences in palate shape. He described white palates as pinched, black palates as being long and narrow while Asian palates as wide and short [14]. As the palatal arch length increases the width also increases until the inter first molar. The width then remains constant. Hence the width for the palatine index was chosen at second molar in the present study [8]. This result gave rise to the accepted natural view that the shape of palatal arch is U shape palatal vault otherwise the shape of palate will be semicircular. Palatal dimensions are statically different between sex and race, so that, there is opportunity to establish criteria by which the dentist and forensic physician can predict the race and sex of unknown individual [15]. In the present study we found that there are significant differences between male and female palatal dimensions. These can be deployed to compare with other population [16]. The size of palate is larger in males group than females and the average difference in the palatal depth is significantly higher in males than females this simply reflect the greater overall breadth of male skull in any given ethnic group. These results are in agreement with the result of most other previous studies by Hassanali J, et al. [12]; Carter GA, et al. [17]; Hsu BS, et al. [18]; Gujar SM, et al. [19]. We have also taken additional measurements in the current study which can be of use as future reference, like lengths AR and AL.
Gujar SM, et al. [19] in their study they found leptostaphyline, mesostaphyline and brachystaphyline 68%, 20% and 12% in comparison to Pallavi, et al. [11]. Which were 95% leptostaphyline and 5.35% mesostaphyline. In the present study we found that the majority (59%) of skulls had narrow palate (Leptostaphyline) [11]. These results are in agreement with the result of other previous studies Krogman Wm, et al. [20] described 14 indicators with an accuracy of 90% for helping with sex determination, and one of these indicators is the shape of the palate. Moreover, palate is well protected within the oral cavity which makes them resistant to damage by massive trauma and thermal insults [20]. This makes sex estimation and individual identification using the morphometric features of the palate a convenient method of identification when there is massive tissue damage. Morphologic and morphometric knowledge of hard palate is advantageous in many fields of medical science. Since there are few studies available on the morphometric measurements of hard palate, the present study based on Indian population of known gender can be used to compare data with other population.
Conclusion
Morphologic and morphometric knowledge of hard palate is advantageous in many fields of medical science. Since there are few studies available on the hard palate, the present study based on Indian population of known gender may be helpful for surgeons, anatomists, dentists, anthropologists and forensic experts. It can be used to compare data with other population.
Acknowledgements
The authors would like to sincerely thank those who donated their bodies to science so that anatomical research and teaching can be performed. Results from such research potentially increase scientific knowledge. Therefore donors and their relatives deserve our high respect. We are also thankful to the statistician for his input and guidance for statistical analysis.
Conflict of Interest: Nil
Funding: Nil
References
-
Standring S (2005) Gray’s anatomy, The Anatomical Basis of Clinical Practice. 39th(Edn.), Edinburgh: Elsevier, Churchill Livingstone, pp: 459.
-
Moore KL, Persaud TVN (1998) The developing human: Clinically Oriented Embryology. 6th(Edn.), Philadelphia: W.B. Saunders Company, pp: 245-252.
-
Maier CA, Zhang K, Manhein MH, Li X (2013) Palate shape and depth: A shape matching and machine learning method for assessment of ancestry from skeletal remains. J Forensic Sci 60(5): 1129-1134.
-
Lammert A, Proctor M, Narayanan S (2013) Morphological variation in the adult hard palate and posterior pharyngeal wall. J Speech Lang Hear Res 56(2): 521-530.
-
Tangugsorn V, Skatvedt O, Krogstad O, Lyberg T (1995) Obstructive sleep apnoea: a cephalometric study. Part-I. Cervico-craniofacial skeletal morphology. Eur J Orthod 17(1): 45-46.
-
Janardhan Rao M, Shiny, Vinila BH, Yes M (2017) Morphological and morphometric analysis of the hard palate and the greater palatine foramen in the dry adult south Indian skulls. International Journal of Anatomy and Research 5(4.1): 4441-4444.
-
Patel M (2012) A study of the hard palate in the skulls of central Indian population. Int J Pharma Bio Sci 3(2): 527- 533.
-
Mack MR (1996) Perspective facial esthetic in dental treatment planning. J Prosthet Dent 75(2): 169-176.
-
Sumati, Patnaik VVG, Phatak A (2012) Determination of sex from hard palate by discriminant function analysis. Int J Basic Appl Med Sci 2(3): 243-251.
-
Sarilita E, Soames R (2015) Morphology of the hard palate: a study of dry skulls and review of the literature. Rev Arg de Anat Clin 7(1): 34-43.
-
Pallavi, Singh P, Kumar A, Ranjan Sinha R, Kumar B, et al. (2020) Morphometric Analysis of Hard Palate & its Clinical Significance. Int J Med Res Prof 6(3): 5-8.
-
Hassanali J, Mwaniki D (1984) Palatal analysis and osteology of the hard palate of the Kenyan African skulls. Anat Rec 209(2): 273-280.
-
Moss-Salentijn L HD 14: Facial and Palatal Development. Larsen 3rd (Edn.), Chapter 12, pp: 352-404.
-
Hooton EA (1946) Up from the Ape. New York: MacMillan Company, pp: 788.
-
Salman KA (2001) The relationship between the maxillary arch width, depth and circumference. Al- Rafidian dent J 1(3): 401-410.
-
Burris BG, Harris EF (1998) Identification of race and sex from the palatal dimension. J Forensic Sci 43(5): 959-963.
-
Carter GA, Macnamara JA (1998) Longitudinal dental arch change in adult. Am J Orthod dentofacial orthop 114(1): 88-99.
-
Hsu BS (1998) The nature of arch width difference of the anterior openbite. Am J orthod dentofac orthop 113(3): 344-350.
-
Gujar SM, Oza SG (2018) Morphometric analysis of hard palate and its clinical importance. National J clinical anatomy 7(1): 36-40.
-
Krogman WM, Iscan MY (1986) The Human Skeleton in Forensic Medicine, 2nd (Edn.). University of Mchigan, USA, pp: 359.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat