Bifurcation of the Radial Nerve in the Arm as a Cause of Traumatic Partial Nerve Palsy: A Case Report
Purpose: To describe the case of a traumatic partial nerve palsy following an open crushing arm injury. The partial palsy was due to the presence of radial nerve bifurcation in the proximal arm. Methods: A 23-year-old male was involved in a motor vehicle accident, where his motorbike crushed against a steel road divider sustaining multiple injuries in the spine, thorax, and right arm. On clinical examination, the patient presented a deep, blunt trauma on the posterior aspect of the proximal arm and partial radial nerve palsy was diagnosed with preservation of the brachioradialis and the extensor radialis longus muscle function. Surgical exploration was carried out. Results: An extensible posterior approach to the arm was performed and two main radial nerve branches were found. The lateral, more sizeable nerve, had an epineural hematoma without any distal response during intraoperative stimulation. The medial, thinner nerve trunk was preserved and, when stimulated, elicited response from the brachioradialis. Conclusion: We describe an uncommon variation of the radial nerve which was associated with partial palsy following blunt force trauma. This anatomical variation should be kept in mind in cases like the one described.
Introduction
The radial nerve originates from the ventral rami of the spinal nerves C5 to T1 and is the largest of the 5 terminal branches of the posterior cord entering the posterior arm compartment through the triangular space [1, 2]. It then runs along the posterior spriral groove of the humerus lying in close contact with the periosteum. It then descends between the lateral and the medial triceps muscle heads, reaching the distal third of the arm where it enters the anterior arm compartment penetrating the the lateral intermuscular septum. It then runs between the brachialis and the brachioradialis muscles splitting into the terminal superficial and deep branches [2, 3, 4]. The radial nerve with its muscular branches (rami musculares) supplies several muscles in the arm and forearm, including the Triceps brachii, Anconæus, Brachioradialis, Extensor carpi radialis longus, and Brachialis. The deep branch of the radial nerve (dorsal or posterior interosseous nerve) supplies all the other muscles on the radial side and dorsal surface of the forearm [1, 2, 3, 4].
The radial nerve in the arm is vulnerable to direct or indirect injury and is not uncommon in fractures of the humeral diaphysis due to its close proximity with the humeral shaft [1]. In a systematic review, the incidence of radial nerve palsy in diaphyseal humerus fractures was 11.8% (532 palsies in 4517 fractures) [5]. Radial nerve palsy was more common in middle and middle-distal parts of the shaft [5]. Herein, we report a rare case of radial nerve bifurcation leading to peculiar partial radial nerve palsy following blunt force trauma to the arm.
Case Report
A 23-year-old male was involved in a motor vehicle accident, where his motorbike crushed against a steel road divider sustaining multiple injuries in the spine, thorax, and right arm. On clinical examination, the patient presented a transverse deep, blunt wound on the posterior aspect of the proximal arm (Figure 1) and partial radial nerve palsy was diagnosed with preservation of the brachioradialis and the extensor radialis longus muscle function. There was no active thumb and finger extension or supination. Surgical exploration was carried out using an extensible posterior approach to the arm by extending the transverse wound proximally and distally. Using a combination of sharp and blunt dissection, the long and the lateral heads of triceps were separated, and the medial head of the triceps was exposed. The radial nerve was located and followed distally. Surprisingly, two neural branches were located, a thicker lateral nerve branch and a thinner medial nerve branch (Figure 2). Both neural branches had the same course distally, piercing the lateral intermuscular septum and entering the anterior compartment of the arm. No nerve trunk was clearly divided but the lateral branch had an epineural hematoma, which was evacuated using microsurgical dissection and neurolysis was performed. The VARI-STIM III nerve stimulator (Medtronic Inc, Jacksonville, Florida) was used for intraoperative nerve stimulation. When the probe tip is in direct contact with the nerve, the device can delivered 1 or 2 mA stimuli. The lateral trunk did not show any distal response during intraoperative stimulation although the medial, thinner nerve trunk, when stimulated, elicited motor response from the brachioradialis.

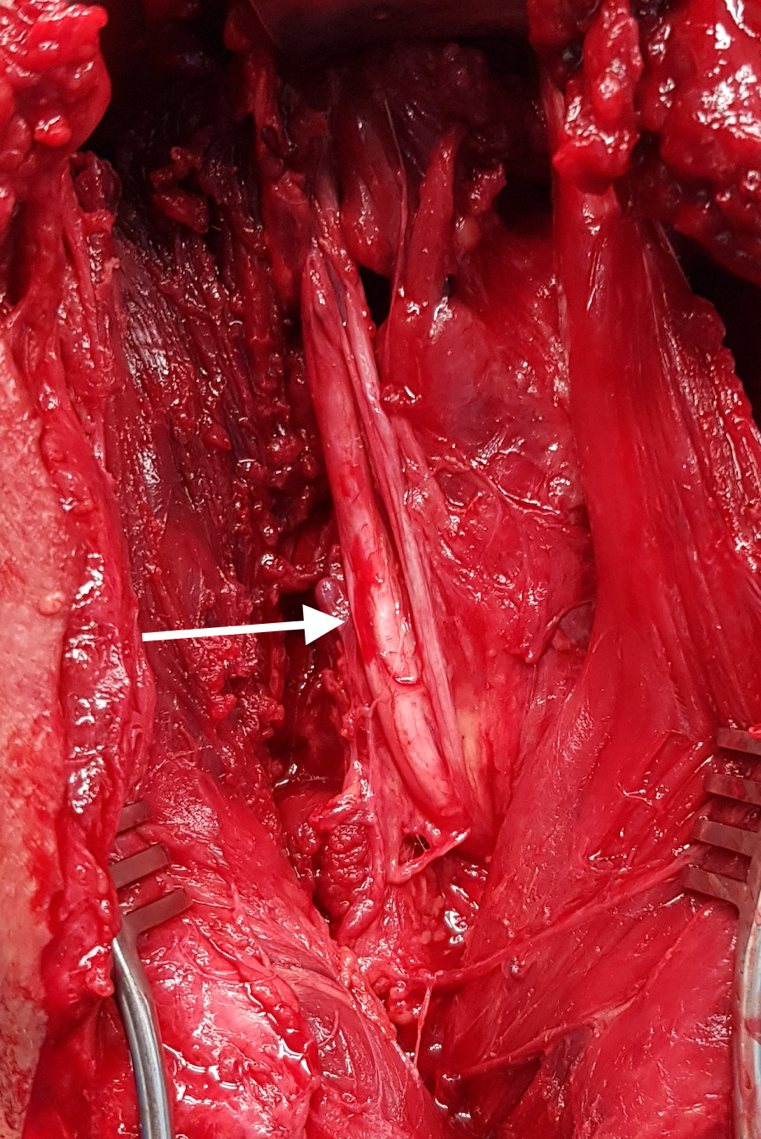
Figure 2: Extensile posterior approach to the proximal right arm of the patient. The elbow is on the upper border of the photograph. The radial nerve was explored using microsurgical technique. The radial nerve was found to be bifurcated. The thicker lateral nerve trunk (white arrow) had an epineural hematoma, and the smaller medial trunk was intact.
Postoperatively, the surgical wound was partially closed and finally healed following repeated surgical debridements and application of a vacuum assisted closure system. The function of the radial recovered fully within the next 4 months.
Discussion
The first case of radial nerve bifurcation in the arm has been described, to the best of our knowledge. The anatomical variation was accidentally encountered in a patient with blunt force trauma to the arm and accompanying partial radial nerve palsy. Knowledge of the anatomical variations of the peripheral nerves is essential in the clinical and surgical practice. Although anatomical variations of the median and the ulnar nerve are commonly reported, variations of the radial nerve are probably less common [1, 6, 7, 8, 9]. Typically, the radial nerve bifurcates at the level of the lateral humeral epicondyle [1, 3], although in our case the bifurcation occurred directly from the posterior cord of the brachial plexus. The radial nerve pierces the lateral intermuscular septum, on average, 38% (29%–56%) of humeral length, proximal to the lateral epicondyle and the posterior interosseous division occurs on average 1 cm (-11.4 to 3.5) distal to the lateral epicondyle [3]. In a case report, trifurcation of the radial nerve in the radial groove was encountered in a patient with a humerus fracture, without radial nerve palsy [8].
Radial nerve palsy is a debilitating injury and is encountered in patients with both open and closed injuries and fractures of the humerus [1, 5, 7]. Open exploration is indicated in cases where neurotmesis is suspected such as open fractures, high velocity gunshot wounds, penetrating injuries and injuries associated vascular trauma. The majority of radial nerve palsies are neurapraxic injuries and improve with observation alone.The overall rate of radial nerve recovery in fractures of the humeral shaft is 88.1% (921 of 1045), with spontaneous recovery reaching 70.7% (411 of 581) in patients treated conservatively [5]. Similarly, in another systematic review spontaneous radial nerve palsy recovery was reported in 85% of the cases [7]. Exploration and neurolysis during humerus fracture management led to much higher rates of recovery than expectant management [7].
The clinical significance of a radial nerve bifurcation is considerable because it may explain the disparity between clinical, imaging and electromyographic findings in cases like the one presented. Additionally, the surgeon should be prepared to encounter anatomic variations when he/she is performing peripheral nerve operations.
Conclusion
We described the first case, to the best of our knowledge, of radial nerve bifurcation in the arm. Rare anatomical variations, such as the one described, should be considered when the findings of the clinical examination do not coincide with the level or the extent of an injury.
Declarations
Conflict of Interest
The author has no competing interest to declare. No funding was received in support of this study.
Ethical Approval and Consent to Participate
All surgical procedures were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments.
Data Availability
All intraoperative and postoperative photographs and videos are available from the corresponding author upon request.
Consent for Publication
The patient signed informed consent regarding publishing his data and figures.
References
-
Bumbasirevic M, Palibrk T, Lesic A, Atkinson HDE (2017) Radial nerve palsy. EFORT Open Rev 1(8): 286-294.
-
Cho H, Lee HY, Gil YC, Choi YR, Yang HJ (2013) Topographical anatomy of the radial nerve and its muscular branches related to surface landmarks. Clin Anat 26(7): 862-869.
-
Cox CL, Riherd D, Tubbs RS, Bradley E, Lee DH (2010) Predicting radial nerve location using palpable landmarks. Clin Anat 23(4): 420-426.
-
Glover NM, Black AC, Murphy PB (2023) Anatomy, Shoulder and Upper Limb, Radial Nerve. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
-
Shao YC, Harwood P, Grotz MRW, Limb D, Giannoudis PV (2005) Radial nerve palsy associated with fractures of the shaft of the humerus: a systematic review. J Bone Joint Surg Br 87(12): 1647–1652.
-
Henry BM, Zwinczewska H, Roy J, Vikse J, Ramakrishnan PK, et al. (2015) The Prevalence of Anatomical Variations of the Median Nerve in the Carpal Tunnel: A Systematic Review and Meta-Analysis. PLoS One 10(8): e0136477.
-
Hegeman EM, Polmear M, Scanaliato JP, Nesti L, Dunn JC (2020) Incidence and Management of Radial Nerve Palsies in Humeral Shaft Fractures: A Systematic Review. Cureus 12(11): e11490.
-
Kim KC, Rhee KJ, Shin HD, Kim YM, Kim DK, et al. (2010) Trifurcated radial nerve in the spiral groove of the humerus. J Trauma 68(2): E55-E56.
-
Schwabl C, Hörmann R, Strolz CJ, Drakonaki E, Zimmermann R, et al. (2023) Anatomical Variants of the Upper Limb Nerves: Clinical and Preoperative Relevance. Semin Musculoskelet Radiol 27(2): 129-135.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat