Clinical Case Reports 1976 - 79
In this paper five case reports were presented and include growth of hypoplastic right ventricle following pulmonary valvotomy, intracavitary electrocardiography in the diagnosis of Ebstein’s anomaly of the left atrioventricular valve in congenital corrected transposition of the great arteries, growth phenomenon as a cause of kinking of the right pulmonary artery in Waterston anastomosis, the usefulness of pulmonary vein wedge angiography in the visualization of an obstructed pulmonary artery, false aneurysm of the right pulmonary artery as a new complication of the Waterston anastomosis. For each case report, clinical, chest x-ray, electrocardiogram, angiogram, and other pertinent findings were presented. This was followed by discussion of etiology, diagnosis, and treatment options, as appropriate.
Introduction
During the academic clinical practice for over five decades, the author had the unique opportunity to observe and document many interesting clinical case scenarios. The purpose of this review is to revisit these interesting cases. Because of the voluminous amount of this material, the material may be divided into several parts. In the first and second papers of this series, a total of ten cases seen/ documented in 1970 through 1974 were presented [1, 2]. In this paper, cases seen during 1976-1979 will be reviewed. Each of these case reports, while rare and important clinical observations, do demonstrate a clinical point that is useful to the pediatricians, pediatric cardiologists and/or other physicians.
Growth of Hypoplastic Right Ventricle Following Pulmonary Valvotomy
Introduction: Pulmonary stenosis with an intact ventricular septum is typically associated with a mildly dilated and hypertrophied right ventricle (RV). Hypoplasia of the RV is unusual, but reported. The prognosis of this condition and pulmonary atresia with intact ventricular septum is largely dependent upon the adequacy of the RV size. The management of these cases should include initial successful palliation and procedures to encourage the growth of the RV so that it attains a reasonable size to support the pulmonary circulation. The purpose of our report [3] was to document the growth of the hypoplastic RV in a patient with pulmonary stenosis with intact ventricular septum by pulmonary valvotomy and to discuss the therapeutic implications related to the management of hypoplastic RV with pulmonary stenosis and pulmonary atresia with intact ventricular septum.
Case Report: A one-year-old child had cardiac catheterization and selective cineangiography because of cyanosis and auscultatory features suggestive of pulmonary stenosis (ejection systolic murmur and ejection systolic click at the left upper sternal border). The catheterization findings revealed a RV systolic pressure at systemic level and a right-to-left atrial shunt. RV angiography revealed severe pulmonary stenosis with a markedly hypoplastic RV (Figures 1A & 1B).
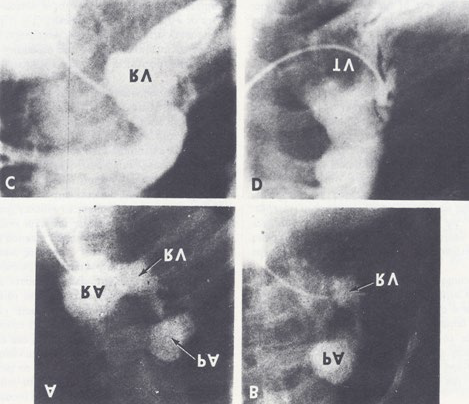
Figure 1A & 1B: Selected frames of right ventricular cine-angiogram in postero-anterior (A) and right anterior oblique (B) views performed at the age of one year, demonstrating an extremely hypoplastic right ventricle (RV). Note the tricuspid regurgitation resulting in the opacification of the right atrium (RA) and the post-stenotic dilatation of the pulmonary artery (PA). C and D. Selected frames of right ventricular cine-angiogram in right anterior oblique views of the same patient as shown in A and B, performed at the age of 4.5 (C) and 10 (D) years demonstrate a considerable increase in the size of the RV when compared to A and B. Also note the non-opacified blood flowing through the tricuspid valve (TV) in D, showing that there has also been growth of the TV. There is only minimal tricuspid regurgitation. Reproduced from Rao PS, et al. [3].
The patient underwent pulmonary valvotomy by Brock’s [4] technique (this was in the pre-balloon pulmonary valvuloplasty era). The patient improved, and had less cyanosis and better exercise tolerance. Reevaluation at 4.5 years revealed normal right ventricular systolic pressure, no evidence for tricuspid stenosis, a persistent right-to-left shunt at the atrial level and an improved RV size (Figure 1C). Because of increasing cyanosis, clubbing of the fingers and toes, and polycythemia, the patient had repeat cardiac catheterization at the age of 10 years, which showed normal RV and pulmonary artery (PA) systolic pressures without any gradient across the pulmonary valve, and the persistence of the right-to-left atrial shunt. RV angiography revealed a continued improvement in RV size (Figure 1D). The surgical closure of the atrial septal defect was performed (this was in the pre-trans-catheter atrial septal defect occlusion era). He improved regarding his cyanosis. Subsequent clinical follow- ups over the next 3.5 years revealed continued improvement.
Discussion: The case presented clearly demonstrated that the growth of a hypoplastic RV was induced by successful pulmonary valvotomy. The factors causing the RV growth were not clear, but the discussion presented favored the idea that free pulmonary regurgitation was likely to be responsible for the RV growth [3]. A detailed discussion of a comprehensive approach to the management of hypoplastic RV was presented; this included pulmonary valvotomy at the time of initial presentation, staged surgical correction utilizing the RV, and staged surgical correction by RV bypass. We have also commented upon the interesting finding of a right-to-left atrial shunt in the presence of normal RV systolic pressure, and attributed it to decreased RV compliance [3].
Diagnosis of Ebstein’s Anomaly of the Left Atrioventricular Valve with Congenital Corrected Transposition of the Great Arteries by Intracavitary Electrocardiography
Introduction: The diagnosis of Ebstein’s anomaly of the tricuspid valve by the simultaneous recording of intracavitary electrocardiograms and pressures across the tricuspid valve was a well-established technique as of the mid-1970s. However, such a method has not been used as of that time to diagnose Ebstein’s anomaly of the left atrioventricular valve in patients with congenital corrected transposition of the great arteries (CCTGA). The purpose of our paper [5] was to document simultaneous recordings of the intracavitary electrocardiogram and pressure in a patient with CCTGA and Ebstein’s anomaly of the left atrioventricular valve and to establish the utility of intracavitary electrocardiographic studies in the diagnosis of this entity.
Case Report: A female infant weighing of 3.3 kg was born after a normal pregnancy, labor, and delivery. The baby presented with tachypnea and poor feeding at the age of two weeks. Physical examination revealed a holosystolic murmur suggestive of a ventricular septal defect (VSD) and signs of congestive heart failure (CHF). The chest roentgenogram demonstrated cardiac enlargement and increased pulmonary blood flow. The electrocardiogram (ECG) revealed right ventricular (RV) hypertrophy. In addition, the initial QRS vector was directed to the left, indicating CCTGA. Following therapy with digoxin and diuretics, CHF improved. Cardiac catheterization with selective cine-angiography indicated CCTGA (Figure 2), large left to right shunt across the VSD, mild subvalvular pulmonary stenosis, and a patent foramen ovale (PFO). The left-sided, morphologic RV cine-angiogram Figure 2b showed significant left atrioventricular valve regurgitation, suggesting the possibility of Ebstein’s anomaly of the left atrioventricular valve.
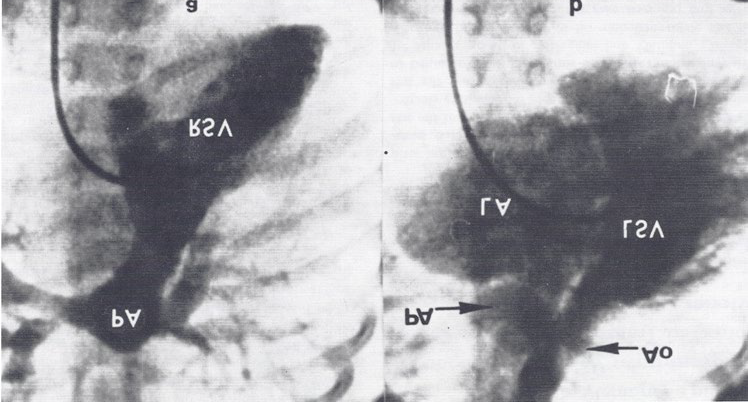
Figure 2a: Selected frame of right-sided ventricular (RSV) cine-angiogram demonstrating smooth-walled morphologic left ventricle on the right side with opacification of the pulmonary artery (PA). b. Selected frame of left-sided ventricular (LSV) cine-angiogram demonstrating coarsely trabeculated morphologic right ventricle on the left side with opacification of the aorta (Ao). Note the significant left-sided atrioventricular valve insufficiency, resulting in the opacification of the left atrium (LA). The PA is also opacified because of a left-to-right shunt via a ventricular septal defect (not marked). Reproduced from Rogers JH, et al. [5].
During the next one year, the baby did well with control of her CHF although the weight gain was slow. Re- evaluation including cardiac catheterization and selective cineangiography at 13 months of age revealed findings like those of previous evaluation with the exception that the VSD became smaller. Since Ebstein’s anomaly of the left atrioventricular valve was suspected, simultaneous intracavitary electrocardiogram and pressure recordings were performed. A #5 French unipolar platinum-tipped electrode catheter (USCI 56IO) was positioned in the ascending aorta. Where a small loop was formed. This loop was pushed forward across the aortic valve into the left- sided ventricle, and from there was manipulated across the left atrioventricular valve into the left atrium. Intracavitary ECG along with pressures was recorded concurrently as the electrode catheter was slowly withdrawn from the left atrium into the left-sided morphologic right ventricle (Figure
3). This recording displayed a ventricular ECG complex at a time when an atrial pressure tracing was present (Figure 3), confirming the existence of Ebstein’ s anomaly of the left atrioventricular valve.
![Figure 3: Simultaneous recording of intra-cardiac electrocardiogram (ECG) and pressures as the electrode/pressure recording catheter is slowly withdrawn from the left atrium (LA) to the left-sided, morphology-right ventricle (LSV). The left panel shows the atrial pressure curve with an atrial electrogram. The middle panel shows the atrial pressure curve with a ventricular electrogram when the tip of the catheter is in the atrialized ventricular chamber. The right panel shows the ventricular pressure curve with a ventricular electrogram when the tip of the catheter is in the ventricular chamber. Pressure is marked in mmHg. The pressure in LSV is damped because of the small diameter of the catheter. Reproduced from Rogers JH, et al. [5].](/fulltextimages/11599/fig_3.png)
Figure 3: Simultaneous recording of intra-cardiac electrocardiogram (ECG) and pressures as the electrode/pressure recording catheter is slowly withdrawn from the left atrium (LA) to the left-sided, morphology-right ventricle (LSV). The left panel shows the atrial pressure curve with an atrial electrogram. The middle panel shows the atrial pressure curve with a ventricular electrogram when the tip of the catheter is in the atrialized ventricular chamber. The right panel shows the ventricular pressure curve with a ventricular electrogram when the tip of the catheter is in the ventricular chamber. Pressure is marked in mmHg. The pressure in LSV is damped because of the small diameter of the catheter. Reproduced from Rogers JH, et al. [5].
Discussion: We made simultaneous intracavitary electrocardiographic and pressure recordings across the left atrioventricular valve simultaneously (Figure 3) in a 13-month-old infant with angiographically confirmed CCTGA and left atrioventricular valve insufficiency (Figure 2) [5]. These recordings were like those obtained in classic cases of Ebstein’s anomaly of the tricuspid valve.
In this paper [5], we reviewed the historical aspects of CCTGA, described the anatomy and typical angiographic findings of the condition, and pointed out the frequent association of Ebstein’s type of malformation of the left-sided, morphologic tricuspid valve with CCTGA and the usefulness of recognizing this abnormality in the management of CCTGA [5]. The characteristic features of Ebstein’s are
- atrial pressure with atrial electrogram,
- atrial pressure with ventricular electrogram, and
- ventricular pressure with ventricular electrogram, in that order, as the electrode catheter is slowly withdrawn from the left atrium to the left- sided, morphology-right ventricle (Figure
Growth Phenomenon as a Cause of Kinking of the Right Pulmonary Artery in Waterston Anastomosis
Introduction: Ascending aorta to right pulmonary artery anastomosis, described by Waterston [6], was widely used in the 1960s and 1970s for the palliation of patients with severe right ventricular outflow tract obstruction causing severe pulmonary oligemia. Despite the extensive use of this surgical technique, large shunts, producing heart failure and pulmonary vascular obstructive disease; and kinking of the right pulmonary artery proximal to the shunt location, causing left lung oligemia have been reported as of the mid- 1970s. We hypothesized that kinking of the right pulmonary artery is likely to be related to growth phenomenon, rather than to the surgical technique [7]. We presented our observations in an infant who had Waterston anastomosis in support of this hypothesis [7].
Case Report: A 12-hour-old infant with pulmonary atresia with intact ventricular septum underwent an emergency Waterston shunt (this was in the pre-prostaglandin era) following diagnostic catheterization and selective cineangiography; the infant’s hypoxemia and metabolic acidosis improved following the surgery. On the third post-operative day, the infant’s O2 saturations decreased remarkably, prompting us to evaluate the patency of the shunt. A #5 polyethylene catheter was introduced into the umbilical artery and its tip advanced into the aorta. A hand injection of 2 ml of contrast material was made into the arch of the aorta via the catheter, and there was no evidence of the patent ductus arteriosus; presumably the ductus has closed spontaneously since the first study. The catheter was advanced into the ascending aorta and the angiography with 2 ml of contrast material was repeated (Figure 4a). There was prompt opacification of both branch pulmonary arteries via the Waterston shunt (Figure 4a). The fall in O2 saturation was attributed to the closure of the ductus, and minor respiratory adjustments were made. The infant improved with no further intervention.
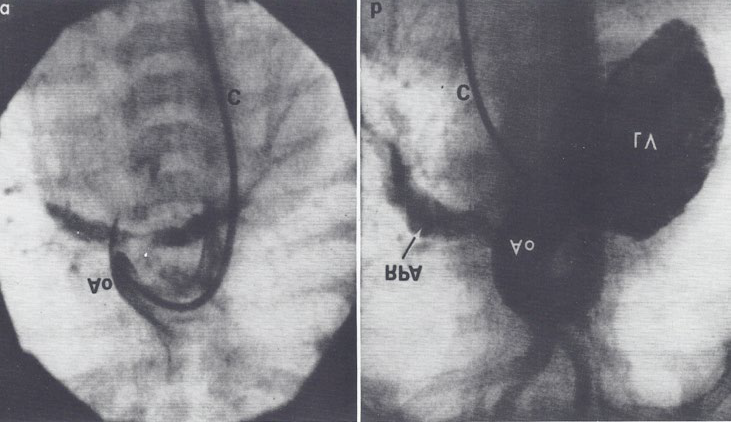
Figure 4a: Selected frame of an aortic (Ao) root cine-angiogram in postero-anterior view, three days after Waterston shunt surgery, demonstrating the prompt opacification of both branch pulmonary arteries via the Waterston shunt. The catheter (C) was positioned in the Ao via the umbilical artery. b. Selected frame of a left ventricular (LV) cine-angiogram in postero-anterior view at the age of 12 months, demonstrating opacification of the aorta (Ao) with visualization of the right pulmonary artery (RPA) but without opacification of the left pulmonary artery (LPA). The catheter (c) is positioned in the LV via the patent foramen ovale and left atrium (not marked). Reproduced from Rao PS, et al. [7].
Following discharge from the hospital, the infant was examined periodically. Progressive polycythemia with a hemoglobin level of 20 gm% was observed by the age of 12 months. A repeat cardiac catheterization was performed prior to considering additional surgery. The findings during this study confirmed the prior diagnoses, but upon left ventricular (LV) angiography, only the right pulmonary artery was visualized via the Waterston shunt (Figure 4b). There was no visualization of the left pulmonary artery in this or any of the other angiograms. This was thought to be due to kinking of the right pulmonary artery proximal to the Waterston shunt.
Discussion: In the case presented, there was good opacification of both the pulmonary arteries via the Waterston shunt shortly after the surgery (Figure 4a). However, on a repeat study at 12 months of age, only the right pulmonary artery was visualized, without opacification of the left pulmonary artery (Figure 4b). This data clearly indicates the obstruction of the left pulmonary artery, presumably secondary to the kinking of the right pulmonary artery (RPA), developed sometime after the initial procedure. Since both pulmonary arteries were seen soon after surgery, it is unlikely that it was caused by the surgical technique. The cardiologists/surgeons at New York reported kinking of the right pulmonary artery in 11 of 15 patients operated on prior to one year of age, while only one in seven patients operated on when older than one year of age had such RPA kinking. They suggested that the kinking may be related to the growth and re-alignment of the great arteries [8]. The case that we presented gives credence to these authors’ observations and supports our hypothesis that the kinking of the RPA following a Waterston shunt is related to growth phenomenon, with a realignment of the great arteries. Based on these observations and other complications associated with the Waterston shunt, we recommended that the Waterston shunt should be avoided and instead, either a corrective surgery (if a given defect is amenable to such surgery) or other types of palliative shunts –such as the aorta-pulmonary Gore-Tex graft shunt or Blalock-Taussig anastomosis – be performed [7].
The Usefulness of Pulmonary Vein Wedge Angiography in the Visualization of an Obstructed Pulmonary Artery
Introduction: The measurement of the size of the pulmonary artery is as important as that of the PA pressure in the overall evaluation and management of congenital heart defects (CHDs). If the pulmonary artery cannot be visualized because of a proximal obstruction, we thought it might be possible to opacify it by pulmonary vein (PV) wedge angiography [9].
Case Report: A four day-old baby with severe cyanosis underwent cardiac catheterization and selective cine- angiography and a diagnosis of pulmonary atresia with a large VSD was made. Shortly after the catheterization, the infant had Waterston shunt with resultant improvement of cyanosis. The baby was followed periodically, and because of increasing cyanosis and polycythemia (Hemoglobin of 20 gm %), a repeat cardiac catheterization was performed at the age of 2 years. The previously made diagnosis of pulmonary atresia and large VSD was confirmed. Left ventricular cine-angiogram revealed good opacification of right pulmonary artery without opacification of the left pulmonary artery (LPA) (Figure 5A). It was presumed that lack of LPA opacification is due to obstruction or kinking of the pulmonary artery as has been described previously [6, 7]. In an attempt to demonstrate the LPA, a left pulmonary vein wedge angiogram was performed [8]. A #5F end-hole catheter was advanced from the RA to LA across the PFO and then into the left mid pulmonary vein. A 4 ml of contrast material was pressure injected while cine filming. The pulmonary vein opacified first with subsequent opacification of the LPA (Figure 5B). The LPA measured 3 mm. The baby had a left Blalock-Taussig shunt two months later. At that time the LPA measured 4 mm. The minor discrepancy between angiographic and surgical measurements is related to the measurement of internal dimension by angiography and external dimension by surgery.
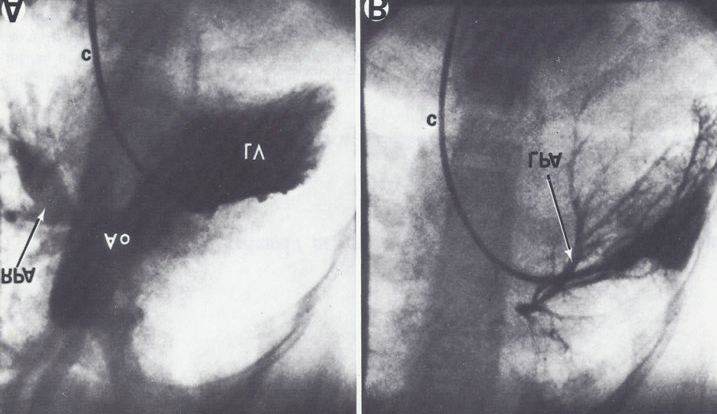
Figure 5A: Selected frame of a left ventricular (LV) cine-angiogram in postero-anterior view, demonstrating the opacification of the aorta (Ao) with a visualization of the right pulmonary artery (RPA) without the opacification of the left pulmonary artery (LPA). The catheter (c) is positioned in the LV via the patent foramen ovale and left atrium (not marked). B. Selected frame of a pulmonary venous wedge cine-angiogram, clearly demonstrating the size of the LPA. The catheter is positioned in the pulmonary venous wedge position via the patent foramen ovale and left atrium (not marked). Reproduced from Rao PS [9].
Discussion: A 2 year-old child with a large VSD and pulmonary atresia who had a Waterston anastomosis in the neonatal period was presented to illustrate the concept and utility of pulmonary vein wedge angiography [9]. Left ventricular angiography clearly visualized the right pulmonary artery (RPA) but the LPA could not be seen (Figure 4A). Non opacification of the LPA was postulated to be due to kinking in the proximal right pulmonary artery, probably related to the relative growth of the vascular structures in that region [7, 8]. A left PV wedge angiogram was performed via a #5 French end-hole catheter with 4.0 ml of contrast material was injected with low pressure. This resulted in the visualization of the LPA retrogradely (Figure 4B). The diameter of the LPA was like that measured at the time of the left Blalock-Taussig
anastomosis shortly thereafter. We suggested that PV wedge angiography is a good technique to demonstrate pulmonary arteries when they are not visualized by conventional anterograde methods. We recommended a PV wedge injection with 0.3 cc/kg of body weight of contrast material, and that it be injected over a two second period under low pressure (less than 100 PSI) [9].
In a subsequent editorial communication, we reported the successful use of this technique in demonstrating the pulmonary artery anatomy by PV wedge angiography in an additional six patients, while commenting on the reported complication of contrast extravagation into the bronchus, with resultant broncho-constriction. We also cautioned against using large quantities of contrast material under high pressure, as suggested by other workers [10]. We reiterated injecting 0.3 cc/kg of body weight of contrast material over a two second period under low pressure (less than 100 PSI) via an end-hole catheter in the PV wedge position, and the immediate removal of the catheter; using such a technique may avoid the complications associated with PV wedge angiography [10].
False Aneurysm of the Right Pulmonary Artery: A New Complication of the Waterston Anastomosis
Introduction: While continuing our observations on the complications of Waterston anastomosis [6], we detected a false aneurysm of the right pulmonary artery following a Waterston shunt [11].
Case Report: A one-year-old child with severe tetralogy of Fallot underwent an ascending aorta to right-pulmonary- artery shunt (Waterston). The child improved. On reevaluation at the age of 5 years, a ring-like calcification at about the level of the Waterston shunt was seen on a chest roentgenogram. The data on repeat cardiac catheterization were consistent with those of tetralogy of Fallot, with a functioning shunt and an arterial O2 saturation of 84%. The main pulmonary artery cine-angiogram revealed only the LPA without opacification of the right PA, and a large aneurysm (Figure 6a). An ascending aortic cine-angiogram showed the opacification of both pulmonary arteries via the Waterston shunt as well as the aneurysm (Figures 6b & c).
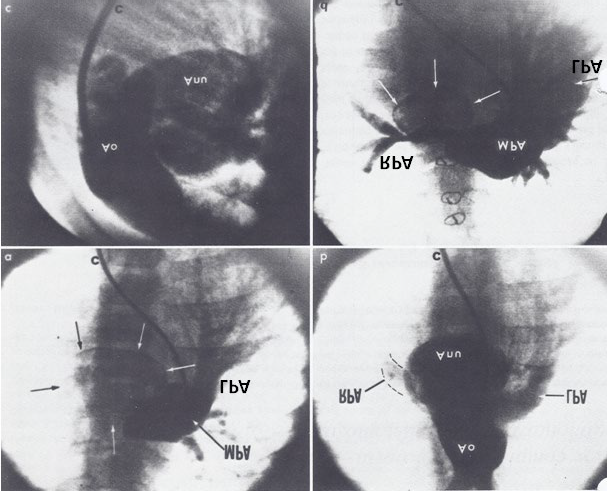
Figure 6a: Selected frame of a main pulmonary artery (MPA) cine-angiogram performed at 5 years of age in postero-anterior view, demonstrating the opacification of the left pulmonary artery without the opacification of the right pulmonary artery (RPA). The calcified aneurysm is marked with the arrows. b and c. Selected frames from an aortic root (Ao) cine-angiogram performed at 5 years of age in postero-anterior (b) and lateral (c) views, demonstrating the opacification of both the LPA and RPA. The calcified aneurysm (Anu) was also seen in b and c. d. Selected frame of an MPA cine-angiogram performed 2 years after surgery in posteroanterior view, demonstrating the opacification of the LPA and RPA. The residual calcified aneurysm is marked with arrows. Reproduced from Monarrez CN, et al. [11].
Surgical correction of the tetralogy of Fallot and the resection of the aneurysm were recommended. During surgery, the aneurysm was noted to be compressing the right PA. The anterior part of the false aneurysm was resected, and the proximal and distal portions of the right PA were identified and reconstructed with an 8 mm Gore-Tex graft, along with the repair of the tetralogy of Fallot. The false aneurysm was not completely removed because it was firmly attached to the adjacent structures. The child improved clinically, and restudy two years later revealed normal systemic arterial O2 saturation (96%) and mild-to-moderate right and left pulmonary artery stenosis. Remnants of the aneurysm were seen (Figure 6d).
Discussion: The case presented demonstrates a false aneurysm of the right PA; this type of complication following Waterston anastomosis had not been previously reported as of that date, and was added to the list of other complications of Waterston documented as of that time. A brief review of the classification of false aneurysms was included in the discussion section of our paper [11].
Summary and Conclusion
In this paper, multiple cases were presented. The first case illustrates that the growth of a hypoplastic RV can be accomplished by surgical relief of pulmonary valve obstruction. In the second case, Ebstein’s-like malformation of the left atrioventricular valve in a patient with congenital corrected transposition of the great arteries was presented which was diagnosed by intracavitary electrocardiography by the simultaneous recording of intracavitary electrocardiograms and pressures across the morphologic tricuspid valve. While this was a well-established technique as of the mid-1970s to diagnose Ebstein’s in non-inverted ventricles, this was the first case to demonstrate the utility of intracavitary electrocardiography in patients with inverted ventricles. In the third case, kinking of the right pulmonary artery in a baby who had Waterston anastomosis was shown to be due to a growth phenomenon rather than to the surgical technique. The fourth case describes the usefulness of pulmonary vein wedge angiography in the visualization of an obstructed pulmonary artery; a useful technique to evaluate pulmonary artery anatomy. In the final case, false aneurysm of the right pulmonary artery following Waterston anastomosis was described; this was a new complication of the Waterston anastomosis. The author hopes that these case illustrations are useful to the physicians providing clinical care to children.
References
-
Rao PS (2023) Clinical Case Reports- 1970. Jour of Clin Cas Rep Med Imag and Heal Sci 5(5).
-
Rao PS (2023) Clinical Case Reports 1971-1974. Jour of Med Case Stud 1(1): 000105.
-
Rao PS, Liebman J, Borkat G (1976) Right ventricular growth in a case of pulmonic stenosis with intact ventricular septum and hypoplastic right ventricle. Circulation 53: 389-394.
-
Brock RC (1948) Pulmonary valvulotomy for congenital pulmonary stenosis. Br Med J (4562): 1121-1126.
-
Rogers JH, Rao PS (1977) Ebstein’s anomaly of the left atrioventricular valve with congenital corrected transposition of the great arteries - diagnosis by intracavitary electrocardiography. Chest 72(2) : 253- 256.
-
Waterston DJ (1962) [Treatment of Fallot’s tetralogy in children under 1 year of age]. Rozhl Chir 41: 181-183.
-
Rao PS, Ellison RG (1978) The cause of kinking of the right pulmonary artery in Waterston anastomosis: a growth phenomenon. J Thorac Cardiovasc Surg 76: 126- 129.
-
Tay DJ, Engle MA, Ehlers KH, Levin AR (1974) Early results and late developments of the Waterston anastomosis. Circulation 50: 220-229.
-
Rao PS (1978) Value of pulmonary vein wedge angiography in visualization of obstructed ipsilateral pulmonary artery. Cardiovasc Radiology 1(3): 151-152.
-
Rao PS (1980) Complications of pulmonary vein angiography (Letter). Brit Heart J 43:124.
-
Monarrez CN, Rao PS, Moore HV, Strong WB (1979) False aneurysm of the right pulmonary artery: A new complication of the aorta-right pulmonary artery anastomosis. J Thorac Cardiovasc Surg 77(5): 738-741.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report