Clinical Case Reports 1980 – 84 (Contrast Echocardiography)
In this paper all case reports reviewed demonstrate usefulness of contrast echocardiography in the diagnosis of cardiac abnormalities. The first case illustrates the utility of this technique in diagnosing anomalous connection of the right superior vena cava to the left atrium. This diagnosis was later confirmed on angiographic studies. In the second paper, contrast echocardiography confirmed the successful results of surgery of the anomalous connection seen in the first case. In the third case, contrast echocardiography was helpful in identifying the cause of hypoxemia in a post-open heart patient, leading to successful closure of the residual cardiac defect.
Introduction
While the author practiced in academic medical centers for a better part of five decades, he had the distinctive opportunity to witness and report several remarkable medical case reports. The objective of this report is to reopen these noteworthy cases. Because of the huge volume of these cases, they were split into multiple parts. In the first report of this series, five case reports published in 1970 were presented [1]. In the second paper, clinical case reports documented in 1971-1974 were discussed [2]. The cases seen between 1976 through 1979 are in the process of publication [3]. In this report, cases seen during 1980 to 84 will be reviewed. While uncommon and notable clinical studies, each of these cases illustrate a clinical theme that is helpful to the practicing physicians.
Use of Contrast Echocardiography in the Diagnosis of Anomalous Venous Connection to the Left Atrium
Introduction: A baby with cyanosis but without any other abnormal clinical findings was investigated by contrast echocardiography and a diagnosis of anomalous systemic venous connection to the left atrium was suspected.
the right heart structures suggesting anomalous drainage of the superior vena cava into the left atrium. An injection into the vein in the right foot resulted in the opacification of the right heart without visualization of the left heart (2 A and B), suggesting normal drainage of the inferior vena cava into the right atrium.
![Figure 1: Selected M-mode recordings from the parasternal short axis view of the left atrium (LA), aorta (Ao), and right ventricular outflow tract (RVOT), made while injecting agitated saline into veins of the right (R) hand, which demonstrate the appearance of contrast echoes in the LA (arrow) first and then the Ao (arrow). B: Similar tracings of the left ventricle (LV) and right ventricle (RV) demonstrate the appearance of contrast echoes in the LV (arrow) without contrast in the RV. Similar findings were seen while injecting agitated saline into the veins of the left hand. These recordings indicate the drainage of the superior vena cava into the left atrium. The start of the agitated saline injection is marked with arrows at the bottom of each tracing. ECG, electrocardiogram. Modified from Truman TA, et al. [4].](/fulltextimages/11818/fig_1.png)
Figure 1: Selected M-mode recordings from the parasternal short axis view of the left atrium (LA), aorta (Ao), and right ventricular outflow tract (RVOT), made while injecting agitated saline into veins of the right (R) hand, which demonstrate the appearance of contrast echoes in the LA (arrow) first and then the Ao (arrow). B: Similar tracings of the left ventricle (LV) and right ventricle (RV) demonstrate the appearance of contrast echoes in the LV (arrow) without contrast in the RV. Similar findings were seen while injecting agitated saline into the veins of the left hand. These recordings indicate the drainage of the superior vena cava into the left atrium. The start of the agitated saline injection is marked with arrows at the bottom of each tracing. ECG, electrocardiogram. Modified from Truman TA, et al. [4].
![Figure 2: Recordings similar to those shown in Figure 1 were made while injecting agitated saline into the veins of the feet, and these reveal contrast in the right ventricular outflow tract (RVOT) (A) and right ventricle (RV) (B) (arrows in A and B) suggesting that the inferior vena cava drains normally into the right atrium (not shown) and RV. The start of the agitated saline injection is marked with arrows at the bottom of each tracing. ECG, electrocardiogram. Modified from Truman TA, et al. [4].](/fulltextimages/11818/fig_2.png)
Figure 2: Recordings similar to those shown in Figure 1 were made while injecting agitated saline into the veins of the feet, and these reveal contrast in the right ventricular outflow tract (RVOT) (A) and right ventricle (RV) (B) (arrows in A and B) suggesting that the inferior vena cava drains normally into the right atrium (not shown) and RV. The start of the agitated saline injection is marked with arrows at the bottom of each tracing. ECG, electrocardiogram. Modified from Truman TA, et al. [4].
At the age of eight months, cardiac catheterization with selective cineangiography was performed. The LA was catheterized via a tight patent foramen ovale (PFO) and the catheter was advanced from the LA into the superior vena cava (SVC) and into both the right and left innominate veins. The right heart saturations were low (60% to 62%) without any evidence for a step up. The pulmonary venous saturations were normal (98%) with a step down in the LA and LV (79%). The pressures in all cardiac chambers were normal (See Table 1 of Reference 4). Selective cineangiography into the right (Figures 3A & 3B) and left (Figure 3C) innominate veins confirmed the diagnosis of an anomalous connection of the right SVC to the LA. No persistent left SVC was identified. Because of the lack of other symptoms and only mild polycythemia (hemoglobin of 15 gm%), surgical correction was deferred at that time, with a plan for surgery at a later date.
![Figure 3: Angiographic frames from injections into the right innominate (A and B) and left innominate (LInV) (C) veins demonstrating direct opacification of the right superior vena cava (SVC), left atrium (LA), left ventricle (LV) and aorta (Ao) without opacification of the right heart structures. C, Catheter. Reproduced from Truman TA, et al. [4].](/fulltextimages/11818/fig_3.png)
Figure 3: Angiographic frames from injections into the right innominate (A and B) and left innominate (LInV) (C) veins demonstrating direct opacification of the right superior vena cava (SVC), left atrium (LA), left ventricle (LV) and aorta (Ao) without opacification of the right heart structures. C, Catheter. Reproduced from Truman TA, et al. [4].
Discussion: An extensive review of the literature revealed only four published cases of anomalous connection of the right SVC to the LA as of the time of our review [4]. The ages at diagnosis were two to 34 years, our case being eight months old. All of them presented with cyanosis and the diagnoses were made by angiography, except for our case which was initially diagnosed by contrast echocardiography and later confirmed by angiography. The differential diagnosis of cyanosis (and arterial desaturation) without any other abnormal cardiac findings includes pulmonary arteriovenous fistula, connection of the pulmonary artery to the LA, and of course anomalous systemic venous connection to the LA. In pulmonary arteriovenous fistula and connection of the pulmonary artery to the LA, the contrast would first appear in the right ventricle before the LA, LV, and Ao. In addition, differential contrast patterns when the site of injection into the veins of upper and lower extremities should not be present with pulmonary arteriovenous fistula and connection of the pulmonary artery to the LA. The discussion also included a review of the possible embryological origin of anomalous systemic venous connection to the left atrium [4].
Contrast Echo Evaluation Following Surgical Correction of Anomalous Right Superior Vena Cava to the Left Atrium
Introduction: The baby reported in the preceding section [4] underwent surgical repair and this report [5] documents the results by contrast echo echocardiography.
Case Report: At the age of twenty-six months, surgical repair was performed under cardiopulmonary bypass, as described in Figure 4. A repeat contrast study following the surgical correction showed opacification of the right heart structures without contrast detected in the left heart after the injection of agitated saline into the arm veins (Figure 5), indicating that the surgery had had good results [5].
![Figure 4: A repeat contrast study following the surgical correction showed opacification of the right heart structures without contrast detected in the left heart after the injection of agitated saline into the arm veins (Figure 5), indicating that the surgery had had good results [5].](/fulltextimages/11818/fig_4.png)
Figure 4: Artist’s portrayal of the surgical correction of anomalous drainage of the superior vena cava (SVC) into the left atrium. A. After incising the SVC the blood is seen going behind the atrial septum (AS) into the left atrium (solid arrow in A). The shadowed area was resected. B. A pericardial patch was sewed in such a way as to divert the SVC flow into the right atrium (solid arrow in B). C. A pericardial patch is placed to enlarge the SVC-right atrial junction. Ao, aorta; IVC, inferior vena cava; PV, pulmonary veins. Reproduced from Alpert BS, et al. [5].
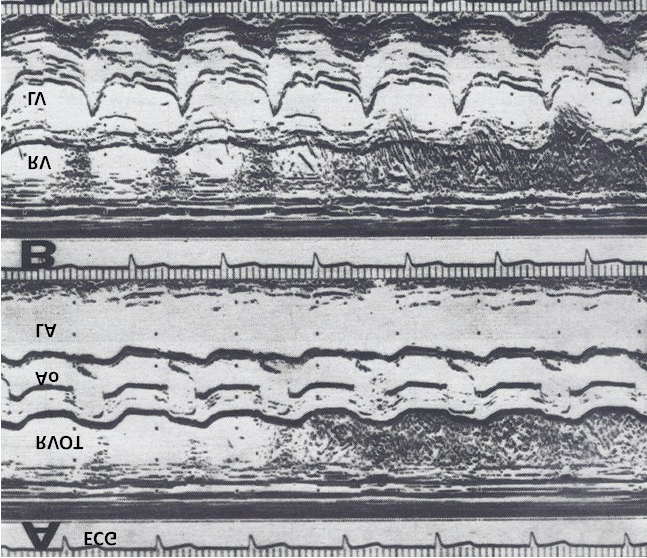
Figure 6: Following surgical correction, recordings similar to those shown in Figures 1 & 2 were made while injecting agitated saline into the veins of the hand, and these reveal contrast in the right ventricular outflow tract (RVOT) (A) and right ventricle (RV) (B), suggesting that the superior vena cava now drains normally into the right atrium (not shown) and RV. AO, aorta; ECG, electrocardiogram; LA, left atrium; LV, left ventricle. Modified from Alpert BS, et al. [5].
Discussion: The discussion focused on the methods of surgical repair performed in the other three cases reported prior to our report, and the usefulness of contrast echocardiography in diagnosing several types of congenital heart defects [5]. Of the four definite cases and one possible case of anomalous connection of the right SVC to the LA, three have been managed surgically in a successful manner. Contrast echocardiography has been used to identify cardiovascular structures; to detect shunts, either right to left or left to right; to demonstrate valvular regurgitation; and to help diagnose a variety of congenital heart defects as references in our publication [5]. The contrast materials which can be used for either central or peripheral injection are blood, indocyanine green dye, or agitated saline. We concluded that the contrast echocardiogram is easily performed from a peripheral vein through a scalp vein needle, and the procedure is feasible in patients of all sizes and ages [5].
In an editorial communication published later [6], in addition to a discussion of the lack of sex-based predilection for the prevalence of this rare anomaly, the differential diagnosis of cyanosis without any other abnormal cardiac findings with the use of noninvasive contrast echo studies, surgery to treat this anomaly and postoperative evaluation, we presented another non-invasive method to diagnose this condition, namely first-pass radionuclide angiographic study (Figure 7).
![Figure 6: Following surgical correction, recordings similar to those shown in Figures 1 & 2 were made while injecting agitated saline into the veins of the hand, and these reveal contrast in the right ventricular outflow tract (RVOT) (A) and right ventricle (RV) (B), suggesting that the superior vena cava now drains normally into the right atrium (not shown) and RV. AO, aorta; ECG, electrocardiogram; LA, left atrium; LV, left ventricle. Modified from Alpert BS, et al. [5].](/fulltextimages/11818/fig_6.png)
Figure 7: First-pass radionuclide angiographic study of the patient with an anomalous connection of the right superior vena cava to the left atrium. A. When radionuclide material (tecnetium-99m macro-aggregated albumin) was injected into a vein in the foot, the inferior vena cava (IVC), right ventricle (RV) and lungs were seen, indicating normal drainage of the IVC into the right atrium. B. When the injection was made into a vein of the left hand, the left (L) arm vein, the superior vena cava (not marked), left atrium (not marked), left ventricle (LV) and aorta (AO) were seen, indicating the anomalous entry of the superior vena cava into the LA. Reproduced from Rao PS [6].
Role of Contrast Echocardiography in the Differential Diagnosis of Hypoxemia Following Open Heart Surgery
Introduction: The utility of contrast echocardiography in a post-operative patient is explored by Rao PS, et al. [7].
Case Report: A three-year-old child had surgical correction for tetralogy of Fallot by patch closure of the ventricular septal defect (VSD), resection of infundibular muscle, and relief of valvar obstruction by a trans-annular pericardial patch. Following surgery, the child maintained good perfusion with normal vital signs, but had marked hypoxemia. The arterial PO2 was around 30 torr with O2 saturations in the mid-50s without any change after administration of 100% O2. No cardiac murmurs were heard and no pulmonary pathology was identified on chest X-ray. Since the patent foramen ovale (PFO) was not closed during the surgery, it was thought that the patent foramen ovale (PFO) might be the reason for the hypoxemia. Contrast echocardiography was performed with the notion of confirming the patent foramen ovale (PFO) as the site of a right-to-left shunt. M-mode recordings from the parasternal short axis view of the LA, Ao, and right ventricular outflow tract (RVOT) were made while injecting agitated saline into the right atrial line, which revealed the almost simultaneous appearance of contrast echoes in the Ao and RVOT, without opacification of the LA (Figure 8), suggesting that there was no inter- atrial shunt and that the shunt was distal to the atria. A similar contrast study made while recording the LV and right ventricle (RV) demonstrated the almost simultaneous appearance of contrast echoes in both the LV and the RV (Figure 9), indicating that that the right-to-left shunt was at the ventricular level.
![Figure 7: First-pass radionuclide angiographic study of the patient with an anomalous connection of the right superior vena cava to the left atrium. A. When radionuclide material (tecnetium-99m macro-aggregated albumin) was injected into a vein in the foot, the inferior vena cava (IVC), right ventricle (RV) and lungs were seen, indicating normal drainage of the IVC into the right atrium. B. When the injection was made into a vein of the left hand, the left (L) arm vein, the superior vena cava (not marked), left atrium (not marked), left ventricle (LV) and aorta (AO) were seen, indicating the anomalous entry of the superior vena cava into the LA. Reproduced from Rao PS [6].](/fulltextimages/11818/fig_7.png)
Figure 8: A selected M-mode recording from the parasternal short axis view of the left atrium (LA), aorta (Ao), and right ventricular outflow tract (RVO) was made while injecting agitated saline into the right atrial line, which demonstrates the appearance of contrast echoes almost simultaneously in the Ao and RVO without opacification of the LA, suggesting that there is no inter-atrial shunt and that the shunt is distal to the atria. The time of injection is marked by an arrow at the left top of the Figure 8. ECG, electrocardiogram. Reproduced from Rao PS, et al. [7].
![Figure 8: A selected M-mode recording from the parasternal short axis view of the left atrium (LA), aorta (Ao), and right ventricular outflow tract (RVO) was made while injecting agitated saline into the right atrial line, which demonstrates the appearance of contrast echoes almost simultaneously in the Ao and RVO without opacification of the LA, suggesting that there is no inter-atrial shunt and that the shunt is distal to the atria. The time of injection is marked by an arrow at the left top of the Figure 8. ECG, electrocardiogram. Reproduced from Rao PS, et al. [7].](/fulltextimages/11818/fig_8.png)
Figure 9: A selected M-mode recording from the parasternal short axis view of the left ventricle (LV) and right ventricle (RV), which demonstrates the almost simultaneous appearance of contrast echoes in the LV and the RV, indicating that that the right-to-left shunt is at the ventricular level. The time of injection is marked by an arrow at the left top of the Figure 9. ECG, electrocardiogram. Reproduced from Rao PS, et al. [7].
The patient was returned to the operating room and upon inspection of the ventricular septum via right atriotomy, a second VSD was noted adjacent to the previously closed VSD, separated by a muscle bundle. The defect was closed with another Dacron patch. The PFO was also closed with sutures. The PO2 and O2 saturation improved. A repeat contrast echo study did not reveal any evidence of a right-to-left shunt.
Discussion
Other investigators have used contrast echocardiography to demonstrate residual post-operative shunts as reviewed in our paper [7], and our report further demonstrates the usefulness of this technique in evaluating postoperative residual shunts. We concluded that this technique is useful in identifying and localizing shunts in postoperative patients [7].
Postscript
It should be noted that the above studies were undertaken prior to the wider availability and use of two- dimensional echocardiography.
Summary and Conclusion
In this paper, several cases, all involving contrast echocardiography were presented. In the first case, anomalous connection of the right superior vena cava to the left atrium, a rare anomaly, was diagnosed by contrast echocardiography using M-mode echo. The diagnosis was later confirmed by angiography and surgical inspection. Following surgical correction, successful surgical result was also confirmed by repeat contrast echocardiography. The third case illustrates usefulness of contrast echocardiography in identifying residual cardiac defect in post-operative tetralogy of Fallot patient, leading to surgical closure of a second ventricular septal defect and resolving the hypoxemia. These case illustrate usefulness of contrast echocardiography in the diagnosis of different types of cardiac abnormalities.
References
-
Rao PS (2023) Clinical Case Reports – 1970. Jour of Clin Cas Rep, Med Imag and Heal Sci 5(5) 1-6.
-
Rao PS (2023) Clinical Case Reports 1971-1974. Jour of Med Case Stud 1(1): 1-11.
-
Rao PS (2023) Clinical Case Reports 1976-1979. Jour of Med Case Stud 1(1): 1-8. DOI: 10.23880/jmcs-16000109.
-
Truman TA, Rao PS, Kulungara RJ (1980) Use of contrast echocardiography in the diagnosis of anomalous connection of the right superior vena cava to the left atrium. Brit Heart J 44(6): 718-723.
-
Alpert BS, Rao PS, Moore HV Covitz W (1981) Surgical Correction of Anomalous Right Superior Vena Cava to the Left Atrium: Post-operative Contrast Echo Evaluation. J Thorac Cardiovasc Surg 82(2): 301-305.
-
Rao PS (1984) Anomalous connection of the right superior vena cava to the left atrium. J Amer Coll Cardiol 4(3): 650-651.
-
Rao PS, Andaya WG, Whisennand HW (1983) Contrast Echocardiography in the Differential Diagnosis of Hypoxemia Following Open Heart Surgery. King Faisal Specialist Hospital Medical Journal 3(2): 121-124.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report