Stomach Foreign Body: A Retrospective Study with a Review
Foreign bodies in the stomach may be accidental or voluntary swallowing. Most foreign bodies are due to unintentional ingestion except in insane people or drug peddlers who may be voluntary. Most of the time, coins are accidentally ingested by children. A rare phenomenon is accidental ingestion of a size 16 to 20 cm in length (toothbrush) foreign body in a sane person. Oesophageal foreign bodies are not as risky as airway foreign bodies. These foreign bodies can obstruct and are located at the oesophagus cricopharynx constriction, the crossover of the aortic arch at the mid-oesophagus, and the lower end. After reaching the stomach, most ingested foreign bodies less than 6 cm will pass uneventfully through the gastrointestinal tract, as in 10 patients who consumed one/two rupee coins. Nevertheless, long and rigid foreign bodies like toothbrushes can result in gastrointestinal impaction, perforation and bleeding. Moreover, there have been a few case reports of spontaneous passage of a toothbrush, and promptly removing such ingested foreign objects is recommended before complications develop. Treatment option remains controversial considering the waiting policy or intervention, either endoscopic or surgical. This study describes 11 patients, 10 cases of coin ingestion and one case of the swallowed toothbrush. Ten cases of coin ingestion were managed conservatively. Upper midline laparotomy was done to remove the toothbrush as removal via flexible endoscopy failed. A swallowed toothbrush is a special clinical challenge. Early retrieval of the toothbrush is critical for reducing morbidity.
Introduction
Accidental/voluntary consumption of foreign bodies is common among patients, especially in the young age group. Most patients can be sent home after reassurance if the foreign bodies are round and less than 6 cm in size without sharp traumatic edges. Depending on foreign bodies’ size, shape, and nature, many patients are admitted for observation and further management. It is common in children between six months and six years of age, and the most common objects ingested are coins and toys, but it is rare in adolescents and adults [1]. In adults, the most common foreign objects of the stomach, after accidental swallowing, are impacted meat bones and other food bolus or dentures [2]. The prisoners voluntarily swallow razor blades, toothbrushes, and several kinds and shapes of metallic items to escape jail [2, 3]. The involuntary ingestion of a foreign object can be dangerous or even lethal and is reported to be responsible for approximately 1,500 deaths per year in the United States [2]. However, The persons who ingest foreign bodies for self-harm usually suffer from psychiatric conditions, alcohol abuse, present developmental or learning disabilities or are prisoners and seek secondary gains [3]. The latest may include a short release from jail and transport to medical facilities to access narcotic analgesic substances, especially for those with a history of drug addiction [4].
Most swallowed indigestible foreign bodies pass through the gastrointestinal tract without complications. However, three physiological narrowings involve the pylorus, duodenal C-loop, and ileocecal valve. Due to its fixed retroperitoneal position, foreign bodies longer than 10 cm, such as a toothbrush, cannot negotiate the duodenal C-loop. These objects should be endoscopically removed soon to avoid pressure necrosis and gastrointestinal perforation. If endoscopic removal fails or there is evidence of obstruction or perforation, open gastrotomy should be performed as in our case [5].
After foreign body ingestion, clinical signs of the acute abdomen may be absent as there is no gastrointestinal perforation or obstruction. These patients usually present with complaints of diffuse pain in the epigastrium or lower chest with the sensations of a foreign body in the stomach and narrate a history of swallowing a foreign body.
Accurate management is often difficult to establish by history alone and mostly depends on the nature of the ingested bodies [6]. Treatment options remain controversial without specific guidelines, considering the waiting policy or immediate intervention, either endoscopic or surgical [7]. Thus, there is always the dilemma of waiting and observing until the treatment of choice is set or intervening promptly [8].
Material & Method
11 cases were reported in an emergency with a history of foreign-bodied stomach in the last three years ( Jan 2019- April 2022). Ten patients were of accidental coin ingestion children’s ages varied from 3 to 5 yrs [Fig-1]. All these children were managed conservatively with success.
| Age in years | Number of cases | Nature of F.B. |
|---|---|---|
| 3 | 2 | Coin |
| 4 | 7 | Coin |
| 5 | 1 | Coin |
Table 1: Ten Caes of Coin Ingestion.
One case was of toothbrush ingestion by a 67-year- old male patient who reported a history of swallowing a toothbrush while brushing his teeth. He gave the history of ingestion of his toothbrush accidentally while cleaning the posterior third of the tongue without abdomen pain or breathing difficulty. The patient’s vitals were stable.
The patient described having transient retrosternal pain, for which he took a small amount of water. No history of dysphagia, shortness of breath, vomiting and upper G.I. bleeding immediately after ingestion. He had no neurological or mental illnesses. A complete physical examination was carried out. All vitals and physical examination findings were normal at the presentation. CECT upper abdomen was done. Based on preliminary examination, a UGI endoscopy was planned for the patient. Endoscopic failed in removing long toothbrush. All pre-operative preparations were done to remove the toothbrush surgically. The patient was operated on within six hours from the time of presentation. The operation was done using general anaesthesia.
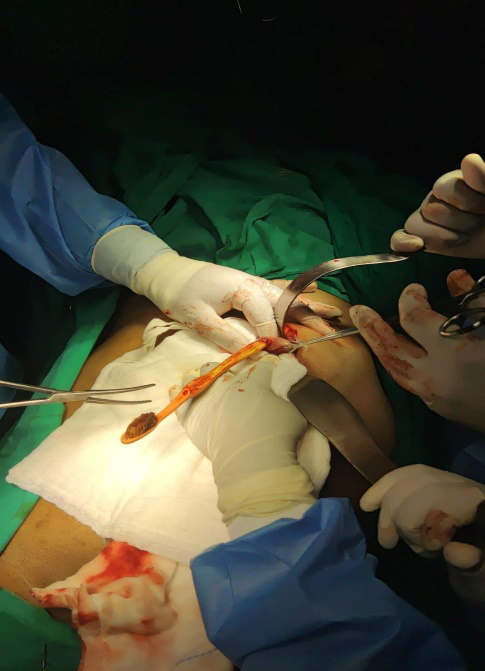
Standard surgical technique was used to enter the peritoneum through supraumbilical midline incision dissecting across the anterior abdominal wall, after which the pyloric antrum was identified. A three cm straight incision was given along the anterior border of the pylorus. The toothbrush was lodged within the lumen at the pyloric antrum. Using forceps, the toothbrush was removed, which measured 19 cm in length [Fig-2]. After removal, the gastric lumen was examined for any injury, and no active hemostasis was noted. An incised segment of the bowel wall was sutured using a 3-0 Vicryl suture. The abdomen wall was closed in layers after ensuring adequate hemostasis. The process described above is shown in Figures 1 and 2.

Discussion
The involuntary ingestion of a foreign object can be dangerous or even lethal and is reported to be responsible for approximately 1,500 deaths per year in the United States [2]. It is a frequent occurrence in children, with a peak incidence between six months and six years of age, and the most common objects ingested are coins and toys, but a rare one in adolescents and adults [1]. In adults, the most common foreign objects of the stomach, after accidental swallowing, are impacted meat bones and other food bolus or dentures [2]. As for prisoners, the most commonly ingested bodies after voluntary swallowing are razor blades, toothbrushes and several kinds and shapes of metallic items [2, 3]. The persons who consume foreign bodies for self-harm usually suffer from psychiatric conditions, alcohol abuse, present developmental or learning disabilities or are prisoners and seek secondary gains [3]. The latest may include a short release from jail and transport to medical facilities to access narcotic analgesic substances, especially for those with a history of drug addiction [4].
Classification of Foreign Bodies [9]
- Size Length </> 6 cm
- Surface Consistency
Rounded versus sharp edges Sharp/pointed versus blunt
- Material/Contents, for Example Battery Food Drugs Magnet
- Characteristics Metallic Radio-dense Chemically inert Plastic materials like toothbrushes After foreign body ingestion, clinical signs of the acute abdomen may be absent as there is no gut perforation or obstruction. The patients usually present with a complaint of diffuse pain in the lower chest or the abdomen, the presence of a foreign body in the stomach, and a history of its ingestion.
The primary diagnosis of the ingested foreign body depends mainly on the history given by the patient; based on the record, the physician can evaluate the type of ingested material and decide the need for urgent intervention. Radiological investigations-X-Ray provides information regarding the material consumed’s number, size, site, and configuration [10].
Stomach fluids and tissue masses may hide small foreign bodies in the radiograph. Plastic material like a toothbrush (as in this case) is not visible on a plain X-ray due to translucency. Identification of such Foreign bodies can be made with the help of computed tomography (C.T.). C.T. with sensitivity (100%) and specificity (91%) has an important role in the diagnosis of ingested foreign bodies [11].
The guidelines about the options to treat gastric foreign bodies are not specific [8]. If ingested foreign bodies cannot be removed, a tailored approach must be thought about the size, shape, and type of the foreign body and the age of the patients.
Moreover, there aren’t precise ways to estimate which objects can pass through the abdominal viscera based on the patient’s size [12]. Nevertheless, the ingested foreign body doesn’t need endoscopic or surgical removal in most cases, as the object will pass through the gastrointestinal tract without causing any injuries. Thus, conservative treatment is possible in almost 80% of the accidentally ingested cases in the general population.
However, in cases of intentional ingestion, endoscopic treatment can range from 63% to 73%, whereas surgical treatment ranges from 12% to 16% [13]. Spontaneous passage through the viscera is expected to occur within
4-6 days, but it can take up to 4 weeks [14]. Therefore, if the object is blunt, round and relatively small (less than 2 cm in diameter and less than 6 cm in length), conservative treatment with close observation is considered the treatment of choice [15]. However, foreign objects over 10 cm, such as a toothbrush, cannot negotiate the duodenal C-loop due to its fixed retroperitoneal position [5].
Special attention must be paid to its alignment with the oesophagus during the toothbrush’s endoscopic extraction. This is important when pulling the toothbrush through the gastroesophageal junction, which may easily result in mucosal damage or toothbrush impaction. The second important stage of the extraction procedure is when the toothbrush reaches the oropharynx. The patient must extend his head backwards to remove the toothbrush with hand and pull it out. Considering all this, usually, endoscopy fails in toothbrush removal, and open surgery is the treatment of choice, which was done in this case [5].
An outpatient management protocol with weekly radiographs should be adopted. Alternatively, these objects may be followed with daily radiographs to identify their location changes. Suppose such blunt and small things remain in the stomach. In that case, it is recommended to delay any attempt of endoscopic retrieval from 3 weeks to up to 2 months after the ingestion to facilitate any possibility of spontaneous passage [16]. However, endoscopy of the upper gastrointestinal tract, an oesophagus-gastro-duodenoscopy, a common and easily accessible procedure, is necessary for 20% of such cases and preferably performed in children. A sharp foreign body that has passed into the stomach or proximal duodenum, larger than 2.5 cm, should be retrieved promptly through endoscopy if this procedure is safely performed. However, endoscopic extraction is considered unsuccessful in 10% of cases [17].
Surgical intervention is essential for objects that fail to progress after 3 days. The chief risk of complications (up to 35%) is with sharp edges or pointed tips [18]. Long delays from ingestion to admission and intervention may account for relatively high perforation rates and the need for surgery [17]. Therefore, patients should be instructed to report symptoms or complications immediately, such as abdominal pain, vomiting, persistent temperature elevations, hematemesis, or melena. Firstly, objects more than 6 to 8 cm in the stomach should be managed by endoscopy, as it was tried in our cases unsuccessfully [19]. Surgical removal of the foreign body is required in less than 1% of the cases. It is performed when endoscopic removal fails or in patients with early complications, such as perforation, obstruction, bleeding after penetration in a vascular structure, and peritonitis or late, such as abscess formation and fistula mucosal ulcerations [20]. Laparotomy is the conventional surgical procedure to remove complicated cases [21].
Recently, laparoscopic removal has become an attractive & useful alternative for treating gastric objects. It can be less invasive, causes less pain, and is followed by faster recovery [21]. Furthermore, combining laparoscopic and endoscopic approaches has many advantages over traditional open procedures. Managing foreign body ingestion is an interesting field in which such a combination approach can be used [21]. Treating foreign body ingestion in prisoners can be tricky, as these patients repeat their actions and present multiple ingestions [22]. It is generally recommended to avoid initial surgical treatment in those patients because there is the risk of the necessity of future operations and self-mutilation of any new surgical wound. Finally, for patients acting as body packers (carriers of illegal drugs that have swallowed them to avoid detection), as the failure rate of the conservative approach is only 2% to 5%, it is advisable to wait for strategy. In such cases, we should closely observe the parcels passing through the viscera and carefully monitor for changes in vital signs or any indication of intoxication [23].
Conclusion
Since endoscopic procedures have progressed, the surgery takes more of a background seat for managing foreign gastric bodies. Thus, endoscopy is considered a safe and efficient method for removing most gastric foreign objects. However, surgical removal, either laparoscopic or laparotomy, remains a crucial procedure for treating certain cases, as our experience shows, where laparotomy has been proven necessary for such sizeable cases as ours.
References
-
Denney W, Ahmad N, Dillard B, Nowicki MJ (2012) Children will eat the strangest things: A 10-year retrospective analysis of the foreign body and caustic ingestions from a single academic centre. Pediatr Emerg Care 28(8): 731-734.
-
Erbil B, Karaca M, Aslaner M, Ibrahimov Z, Kunt MM, et al. (2013) Emergency admissions due to swallowed foreign bodies in adults. WJG 19(38): 6447-6452.
-
Grimes IC, Spier BJ, Swize LR, Lindstrom MJ, Pfau PR (2013) Predictors of recurrent ingestion of gastrointestinal foreign bodies. Can J Gastroenterol 27(1): e1-e4.
-
Telford JJ (2005) Management of ingested foreign bodies. Can J Gastroenterol 19(10): 599-601.
-
Paramythiotis D, Kofina K, Bangeas P, Salonikidis S, Tsakiris G, et al. (2015) Surgical management of sizeable intragastric foreign bodies: two cases of self-harm in psychiatric patients. Surg Chron 20(3): 106-109.
-
Tonkica A, Bogdanovic Z, Grandić L (2011) Successful Endoscopic Removal of a Swallowed Toothbrush: Case Report. Case Rep Gastroenterol 5(1): 122-124.
-
Williams HE, Khokhar AA, Rizvi M, Gould S (2014) Gastric perforation by a foreign body presenting as a pancreatic pseudotumour. Int J Surg Case Rep 5(7): 437-439.
-
Syrakos T, Zacharakis E, Antonitsis P, Zacharakis E, Spanos C, et al. (2008) Surgical intervention for gastrointestinal foreign bodies in adults: A case series. Med Princ Pract 17(4): 276-279.
-
Pavlidis T, Markakis G, Triantafyllou A, Psarras K, Kontoulis TM, et al. (2008) Management of ingested foreign bodies. How justifiable is awaiting policy?. Surg Laparosc Endosc Percutan Tech 18(3): 286-287.
-
Teli B, Taneja J (2020) Rare Case of Accidental Ingestion of Tooth Brush: Endoscopic Retrieval. Asian Journal of Case Reports in Surgery 3(2): 312-315.
-
Mosca S, Manes G, Martino R, Amitrano L, Bottino V, et al. (2001) Endoscopic management of foreign bodies in the upper gastrointestinal tract: Report on a series of 414 adult patients. Endoscopy 33(8): 692-696.
-
Marco De Lucas E, Sadaba P, Lastra Garcia-Baron P, Ruiz- Delgado ML, Sánchez FG, et al. (2004) Value of helical computed tomography in the management of upper oesophagal foreign bodies. Acta Radiol 45(4): 369-374.
-
Sahn B, Mamula P, Ford CA (2014) Review of foreign body ingestion and esophageal food impaction management in adolescents. J Adolesc Health 55(2): 260-266.
-
Ikenberry SO, Jue TL, Anderson MA, Appalaneni V, Banerjee S, et al. (2011) Management of ingested foreign bodies and food impactions. GastrointestEndosc 73(6): 1085-1091.
-
Ambe P, Weber SA, Schauer M, Knoefel WT (2012) Swallowed foreign bodies in adults. Dtsch Arztebl Int 109(50): 869-875.
-
Bisharat M, O’Donnell M, Gibson N, Mitchell M, Refsumet SR, et al. (2008) Foreign body ingestion in prisoners – The Belfast experience. Ulster Med J 77(2): 110-114.
-
Palta R, Sahota A, Bemarki A, Salama P, Simpson N, et al. (2009) Foreign-body ingestion: characteristics and outcomes in a lower socioeconomic population with predominantly intentional ingestion. Gastrointest Endosc 69: 426-433.
-
Smith MT, Wong RK (2007) Foreign bodies. GastrointestEndosc Clin N Am 17(2): 361-382.
-
Ribas Y, Ruiz-Luna D, Garrido M, Bargalló J, Campilloet F (2014) Ingested foreign bodies: do we need a specific approach when treating inmates?. Am Surg 80(2): 131- 137.
-
Dalal PP, Otey AJ, McGonagle EA, Whitmill ML, Levine EJ, et al. (2013) Intentional foreign object ingestions: the need for endoscopy and surgery. J Surg Res 184(1): 145- 149.
-
Furihata M, Tagaya N, Furihata T, Kubota K (2004) Laparoscopic removal of an intragastric foreign body with endoscopic assistance. Surg Laparosc Endosc Percutan Tech 14(4): 234-237.
-
Lee TH, Kang YW, Kim HJ, Kim SM, Heog Im E, et al. (2007) Foreign objects in Korean prisoners. Korean J Intern Med 22(4): 275-278.
-
Silverberg D, Menes T, Kim U (2006) Surgery for “body packers” – a 15-year experience. World J Surg 30(4): 541-546.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report