Primary Anorectal Malignant Melanoma (PARM) with Liver Metastasis: Case Report
Primary Anorectal Malignant Melanoma (PARM) is a rare and aggressive tumor with incidence of 3% of all anorectal cancers. The tumor may seem like adenocarcinomas, small cell carcinomas, or sarcomas histologically, yet it looks like hemorrhoids grossly. It is frequently discovered at an advanced stage due to vague symptoms and its aggressive nature, resulting in a bad prognosis. The prognosis is poor, with a median survival of only 24 months and a 5-year survival rate of < 10%. The majority of patients die as a result of complications related to metastasis. We are reporting a case of 57year old woman with PARM with liver metastasis. The diagnosis of primary anorectal malignant melanoma can be challenging due to its rarity and the overlap of symptoms with other more frequent anorectal diseases. This case study emphasizes the significance of including malignant melanoma in the differential diagnosis of anorectal malignancies. The occurrence of liver metastases highlights the disease's aggressive nature and the importance of a comprehensive diagnostic approach. The treatment options for anorectal melanoma with liver metastases are limited and generally palliative, with the goal of enhancing quality of life and prolonging life expectancy.
Abbreviations
PARM: Primary Anorectal Malignant Melanoma; APR: Abdominoperineal Resection; WLE: Wide Local Excision.
Introduction
Anorectal malignancies are commonly adenocarcinoma or squamous cell carcinoma, with melanoma having a relative incidence of 0.5–4% of all malignancies in this region [1, 2]. This site is the third most common primary location for melanoma after skin and retina and yet only 0.4–1.6% of all primary melanomas arise here [2, 3]. Patients present themselves with local symptoms like rectal bleeding and a changed defecation pattern.
Prognosis is very poor with a median survival of 24 months and a 5-year survival of 10%. Almost all patients die because of metastases [4].
Due to rarity of this entity there is no consensus on which surgical approach is favorable [5, 6]. The surgical procedure of choice ranges from an abdominoperineal resection (APR) to wide local excision (WLE) with or without adjuvant radiotherapy [6].
Case Report
We report a case of PARM in a 57-year-old female presenting with bleeding per rectum since 2 months and vague upper abdominal pain. The patient was in good condition with no weight loss and past medical and family history unremarkable.
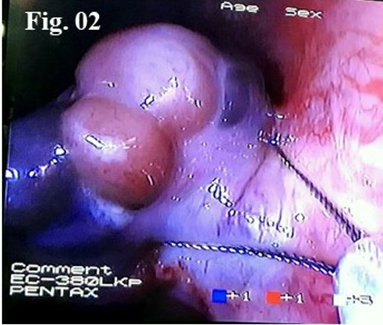
Proctoscopy confirmed the physical examination and showed a 3cm bleeding polypoidal growth that originated 2cm above the dentate line. Colonoscopy was performed which revealed polypoidal growth in the anorectal region with infiltration (Figure 1). Polypectomy was performed (Figure 2) and specimen sent for HPE. CECT abdomen & pelvis revealed an ill-defined heterogenous hypodense lesion in the left lobe (Seg. IV) Showing peripheral enhancement in arterial and washout in portovenous phase (Figure 3) with multiple enlarged portahepatis, celiac and para aortic group of lymph nodes.

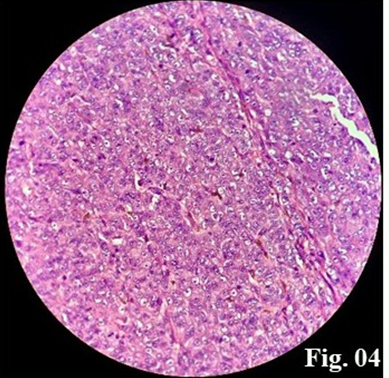
The histopathology of the polyp biopsy concluded to a primitive malignant melanoma (Figure 4) due to the tumour profile in immunohistochemistry: Human Melanoma Black (HMB-45) 3+, S100 protein 2+. Wide spectrum cytokeratins negative. Ki 67: 80-85%. The oncologic multidisciplinary council validates a palliative chemotherapy with Tablet temozolomide 200mg for 14 days every 28 days. Patient refused for chemotherapy and opted to avail alternative medicine likely Ayurvedic. Patient was lost in follow-up and exact details of the palliative treatment patient opted is unknown.

Discussion
Anorectal melanoma is a rare disease that accounts for approximately 1% of all malignant melanomas and 0.5% of tumors of anorectal area. Symptoms are rather nondescript, with bleeding manifesting as the most common complaint. The gross appearance varies from a small, pigmented lesion to an ulcerated mass. PARM is implanted on both sides of the dentate line, hence the term ‘anorectal’, developed from melanocytes of the dentate area.
Macroscopically, the tumours are polypoidal and pigmented while microscopically, the cells are arranged in nests with characteristic immunostaining specific for melanosome protein. However, 30–70% of the lesions can be amelanotic. The histologic markers of S-100, HMB-45 and vimentin are frequently identified and help clarify the diagnosis [7]. If biopsy shows a specimen suspicious for sarcoma (e.g. leiomyosarcoma), S-100 staining should be performed and if positive the tumour is most likely to be a melanoma. In the absence of metastasis surgical therapy is the treatment of choice. There is no consensus on which surgical approach is preferred between WLE and APR [8].
A worse prognosis was also associated with tumour thickness, tumour necrosis (important histologic feature, representing a biologically more aggressive tumour) and perineural invasion [5, 8]. An amelanotic lesion has a worse prognosis [9]. Patients without lymph node metastasis have a survival advantage with a 5-year survival rate of 20 versus 0% in patients with metastasis. Survival of patients with reccurent or metastatic disease is <10 months [10]. There is an important deterioration of the prognosis for tumours superior to 20 mm Five-year actuarial OS, DFS, distant metastases-free survival, local nodal control, and regional nodal control rates were 31%, 37%, 35%, 74%, and 84%, respectively, comparing favorably to varying reports using local excision alone [9, 10].
Conclusion
Metastatic anorectal melanoma is a rare and highly aggressive type of cancer and has a poor prognosis along with a high mortality rate. The aggressiveness and unfavorable prognosis of metastatic anorectal melanoma are well-known. Because of the rapid course of the disease and the sometimes delayed diagnosis, the five-year survival rate is often low—less than 20%. A multidisciplinary team comprising oncologists, surgeons, radiologists, and pathologists is frequently needed for effective management in order to customize specific treatment approaches. Given the high likelihood of recurrence and metastasis, palliative care is crucial to improving quality of life and managing symptomatology. In short, early detection, a multidisciplinary approach, and advancements in targeted therapies and immunotherapy offer hope for better management and improved survival rates. Early detection of the lesion is the cornerstone of management, and in advanced disease, treatment remains palliative care at present.
Author Contributions
Collection and/or Assembly of Data: Anand Bhandary Panambur, Reba Thoppil Philipose Manuscript Writing: Anand Bhandary Panambur Final Approval of Manuscript: Anand Ignatius Peter
Disclosures
Conflict of Interest Statement: The authors have no conflicts of interest to declare.
Funding Sources
The authors did not receive any funding.
References
-
Van Shaik PM, Ernst MF, Meijer HA, Bosscha K (2008) Melanoma of the rectum: a rare entity. World J Gastroenterology 14(10): 1633-1635.
-
Reid A, Dettrick A, Oakenful C, Lambrianides AL (2011) Primary rectal melanoma. JSCR 2011(11): 2.
-
Dube P, Elias D, Bonvalot S, Spatz A, Lasser P (1997) Primary rectal melanoma. About 19 cases. J Chir (Paris) 134(1): 3-8.
-
Yeh J, Shia J, Hwu W, Busam K, Paty P, et al. (2006) The role of abdominoperineal resection as surgical therapy for anorectal melanoma. Annals of Surgery 244(6): 1012-1017.
-
Stefanou A, Nalamati S (2011) Anorectal melanoma. Clin Colon Rectal Surg 24(3): 171-176.
-
Dias AR, Pinto RA, Mory E, Silva IC, Siqueira SAC, et al. (2010) Synchronous collision malignant melanoma and adenocarcinoma of the rectum. Tech Coloproctol 14(2): 181-184.
-
Delikaris P, Koutmeridis D, Tsonis G, Asimaki A, Mouratidou D (1997) Synchronous anorectal malignant melanoma and rectal adenocarcinoma: report of a case. Diseases of the Colon & Rectum 40: 105-108.
-
Wang M, Zhang Z, Zhu J, Sheng W, Lian P, et al. (2013) Tumour diameter is a predictor of mesorectal and mesenteric lymph node metastases in anorctal melanoma. Colorectal Dis 15(9): 1086-1092.
-
Carcoforo P, Raiji MT, Palini GM, Pedriali M, Maestroni U, et al. (2012) Primary Anorectal Melanoma: An Update. Journal of Cancer 3: 449-453.
-
Singer M, Mutch MG (2006) Anal melanoma. Clin Colon Rectal Surg 19(2): 78-87.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report