Parkinson Disease and Ayurveda
Parkinson’s disease, a degenerative brain disease of dopamine secreting brain cells Substantia nigra is increasing progressively and presents therapeutics-levodopa, carbidopa, MAOB inhibitor, COMT inhibitors, surgery and deep brain stimulations, though improve presenting feature but not quality of life. Present study using herbal composite containing Mucuna pruriens, Herpestis monnieri, Acors calamus, Nardostachys jatamansi and Withania somnifera taken in equal part shows better quality of life in all most all with marked improvement in movement disorder in 92% cases as compared to 39% cases on conventional therapy. In addition Herbal composite also improve the haematological, hepatic and Renal function by bioregulating body biomechanics and neural cell function, revitalizing neural cell damage in substantia nigra check destruction of dopamine and facilitate optimal level of Dopamine for normal brain function.
Avinash Shankar1*, Amresh Shankar2 and Anuradha Shankar3
India
dravinashshankar@gmail.com check destruction of dopamine and facilitate optimal level of Dopamine for normal brain function.
Deep Brain Stimulation
Introduction
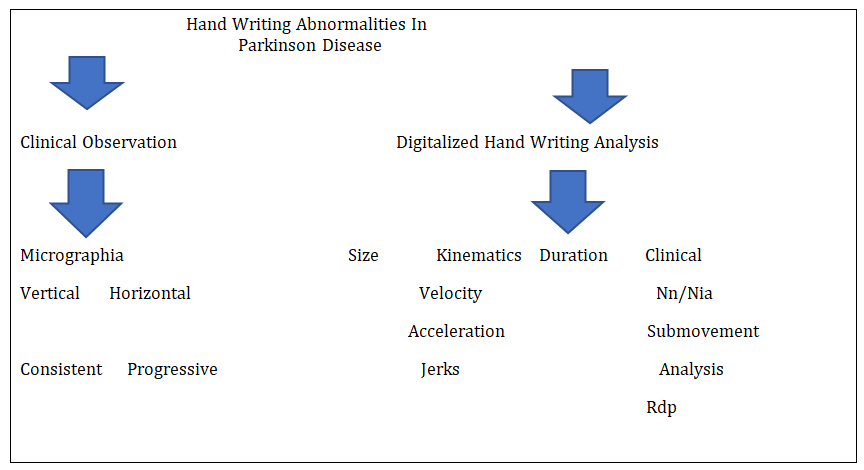
Parkinson disease is a chronic progressive and degenerative disease of Central Nervous System and presents with movement disorders which prompt handicap in long time [1, 2, 3]. This is considered as a combination of genetic susceptibility, exposure to one or more disease triggering environmental factor [4, 5]. Clinical manifestations are solely due to degenerative change in substantia nigra, a seat of an important neuro transmitter synthesis i.e. Dopamine and 60-80% loss of dopamine secreting cells presents with dreaded presentation of movement disorder i.e.- tremor, rigidity, bradykinesia, postural instability. In addition changing dietary habits and lifestyle causes free radical accumulation also triggers the clinical presentation [6, 7, 8, 9, 10, 11, 12, 13, 14] (Figure 1).

Inspite of all the available therapeutic modalities incidence of Parkinson’s disease increasing and affects 1% of the people above the age of 65 years and presently it is 247per lakh. There is no homogenous and large epidemiological data on PD from India. Razdan, et al. reported a crude prevalence rate of 14.1 per 100,000 amongst a population of 63,645 from rural Kashmir in the northern part of India. The prevalence rate over the age of 60 years was 247/100,000.
Thus today’s need is safe affordable and curative therapeutics.
- Objective of the study: Evaluate the comparative therapeutic efficacy of herbal composite in management of parkinsons disease.
- Design of the study: comparative
- Interest of conflicts: None
- Ethical committee: Ethical committee approves the evaluation of status of safe herbal composite in management of Parkinson disease.
Material & Methods
Material
Patients attending neuro clinic of RA Hospital & Research Centre Warisaliganj (Nawada) and Aarogyam Punrjeevan, Patna 14 having complaints of movement disorders were considered for the proposed study.
Patients with severe debility, bed ridden and associated other disease like diabetes mellitus and hypertension were excluded from the study.
Methods
Selected patients and their attendants were thoroughly interrogated for their presenting features, their duration, age of onset, disease progression, treatment taken, their effects and adversity. Patients were clinically examined and investigated for their basic bioparameters to adjudge the effect of drug or drug related adversity (Table 1).
| Stage | Characteristics | ||||
|---|---|---|---|---|---|
| I | symptoms of one side of the body | ||||
| II | symptoms on both side of the body, no balance impairment | ||||
| III | balance impaired, physically independent | ||||
| IV | severe debility and still able to walk or stand | ||||
| V | wheel chair or bed ridden |
Table 1: Selected patients were graded as per clinical presentation (as per Hochu and Yahr sstaging).
Group A: conventional treatment with Levodopa /carvidopa Group B: herbal composite

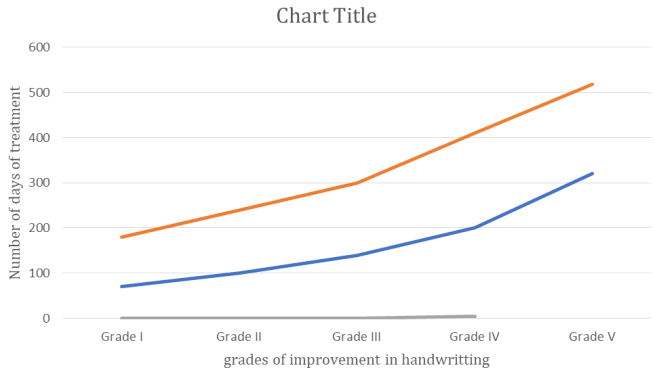
Each patient were given a follow up card to enter the changes in movement, stability and handwriting with an instruction to attend the centre on every alternate Friday for first 6 months and every 3 months afterward. Patients were followed by the Medical social worker of the organization to ascertain the changes in clinical presentation. To adjudge the improvement in CNS function handwriting was analysed digitally on tab (Table 2).
Dose schedule: 1 cap every 8 hours
| Clinical grade | Characteristics | ||||
|---|---|---|---|---|---|
| Excellent | complete absence of movement abnormality without any adjuvant, drug adversity and withdrawal or relapse | ||||
| Good | marked improvement in clinical presentation with occasional dystonia No drug adversity | ||||
| Poor | only transient relief with frequent recurrence and adversity |
Table 2: Clinical response was adjudged.
Observation
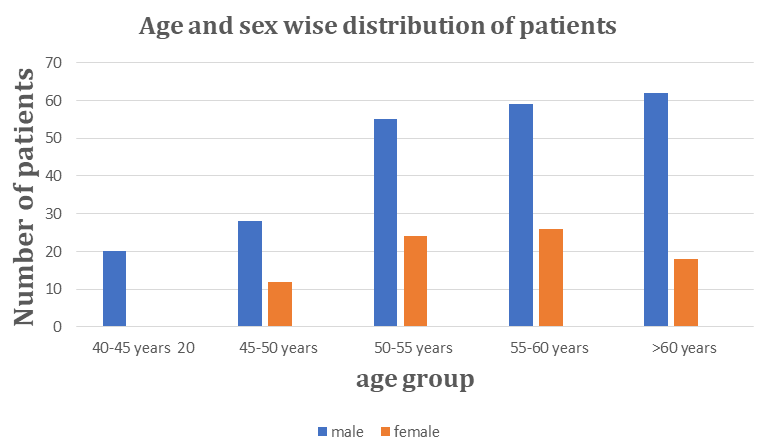
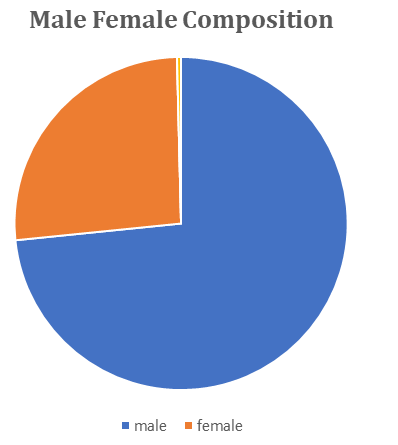
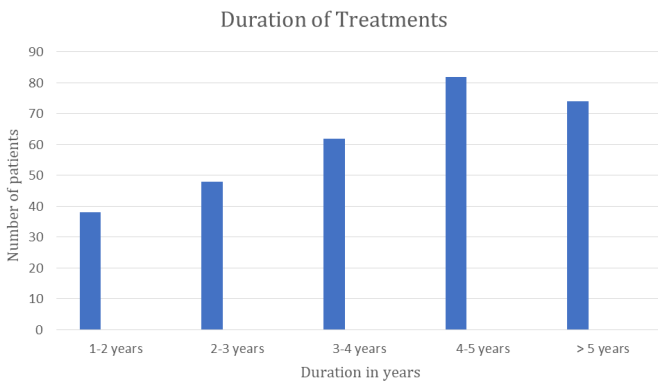
Selected patients were of age group 40->60 years with male predominance over the female and majority patients were of age >60 years, 73.7% male and 26.3% female were of age group 55-60 years, 6.6% of 40-45 years, 26.3% were of >60 years (Figures 3 & 4). Out of all 12.5% were taking treatment since last 1-2 years, 27% sine 4-5 years while 24.3% since >5 years (Figure 5). Figure 3: Bar diagram showing age and sex wise distribution of patients.
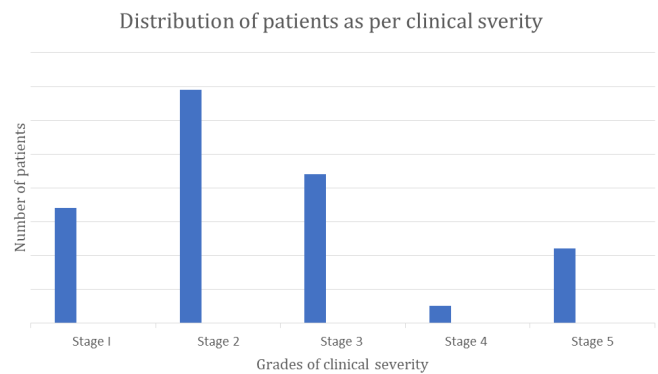
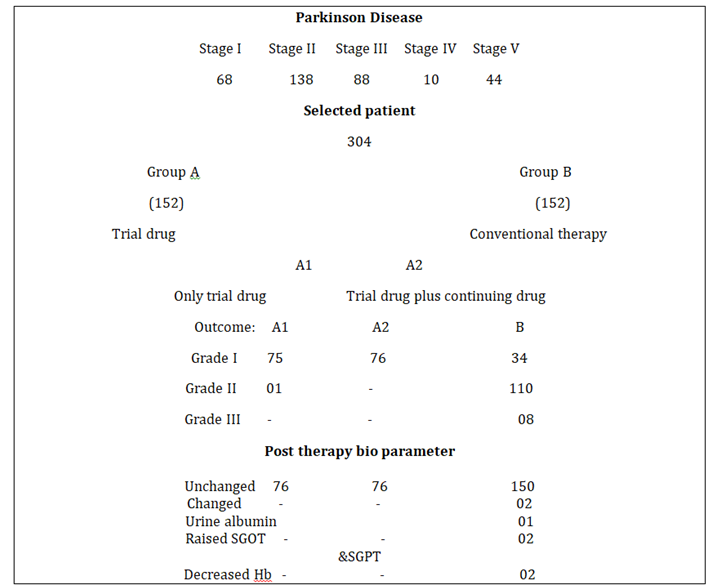
22.4% were presenting with movement disorder, 45.4% with movement disorders on both side and 29% with balance disorder (Tables 3 & 4). As per clinical severity 22.4 %, 45.4%, 29% and 3.2% are of stage I,II,III and IV respectively (Figure 6). Out of all basic bio parameters of the selected patients 77.6% patients had haemoglobin <10 gram %, Serum bilirubin >1mg%, SGOT and SGPT >30 IU, Alkaline phosphatase>130 in 5.3%, blood sugar (Fasting) >100mg% in 3.3% cases .
| Clinical Presentation | N | umber o | f |
|---|---|---|---|
| patients | |||
| Movement disorder on one side of the body | 68 | ||
| Movement disorder on both side of the body | 138 | ||
| Balance impairment | 88 | ||
| Severe debility | 10 | ||
| Wheel chair Or bed ridden | 14 |
Table 4: Showing distribution of patients as per their presentation.
| Basic bio parameters | Number of patients | ||||
|---|---|---|---|---|---|
| Hematological | |||||
| Hemoglobin | |||||
| <10gm % | 236 | ||||
| >10gm% | 68 | ||||
| Hepatic profile | |||||
| Serum bilirubin | |||||
| <1mg % | 236 | ||||
| >1mg% | 68 | ||||
| SGOT | |||||
| <30 IU/L | 236 | ||||
| >30 IU/L | 68 | ||||
| SGPT | |||||
| <30 IU/L | 236 | ||||
| >30IU/L | 68 | ||||
| Alkaline phosphatase | |||||
| < 100 | 288 | ||||
| >100 | 16 | ||||
| Diabetic profile | |||||
| Blood sugar | |||||
| Fasting | |||||
| <100mg% | 294 | ||||
| >100mg% | 10 | ||||
| Renal profile | |||||
| Blood urea | |||||
| <30mg% | 304 | ||||
| >30mg % | - | ||||
| Serum Creatinine | |||||
| <1.5mg% | 304 | ||||
| >1.5mg% | - |
Table 3: Showing basic bio –parameters.
Result
Patients on herbal composite shows early and better movement improvement as adjudged by handwriting or hand movement (ascertained digitally) than other group i.e.-92% patients on herbal composite had normal hand writing while on conventional therapy only 39% cases (Figures 7 & 8). Therapeutic outcome is better in both cases i.e. herbal composite alone or herbal composite with conventional drug than mere conventional therapy, almost 100 % than 22.4% on conventional therapy. Post therapy bioparameters get improved in all the cases on Herbal composite than 02 patients on conventional therapy had worsening of parameters.
Conclusion
Herbal composite constituting equal parts of Mucuna pruriens, Herpestis monnieri, Acorus calamus, Nardostachys jatamansi and Withania somnifera proves worth in patients of Parkinson’s disease in alleviating clinical presentation and improving quality of life without any untoward effects or withdrawal manifestation.
Discussions
Parkinson disease affecting elderly and more male than female result in handicap and bed ridden in spite of advanced therapeutics like surgery and deep brain stimulation, current therapeutics though control movement disorder but fails to improve quality of life. Present study of comparative evaluation of herbal composite versus conventional therapeutics shows superiority of herbal composite than conventional i.e.- 92% patients on Herbal composite had grade I clinical recovery and better quality of life without any adversity or disease related sequel or required any adjuvant as compared to 39% on conventional therapeutics and is attributed to
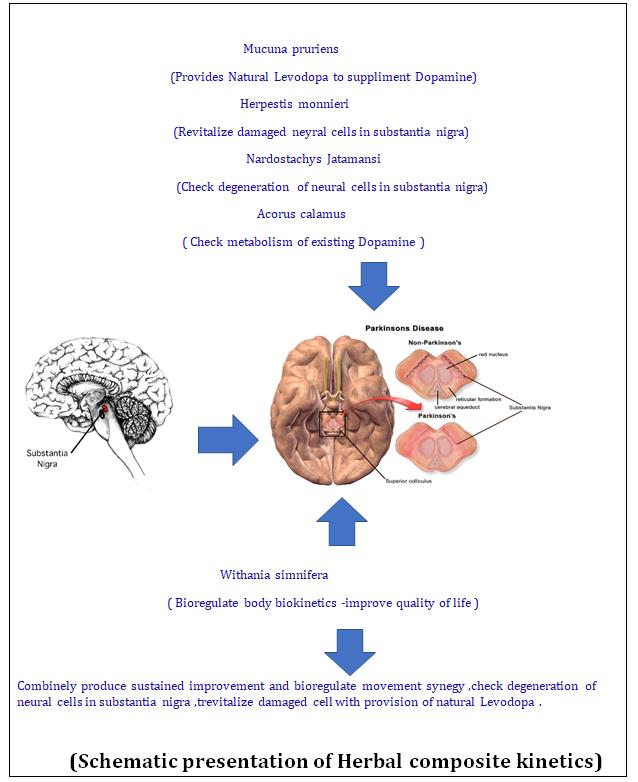
- Mucuna pruriens: Provides Natural Levodopa to suppliment Dopamine
- Herpestis monnieri: Revitalize damaged neyral cells in substantia nigra
- Nardostachys jatamansi: Check degeneration of neural cells in substantia nigra
- Acorus calamus: Check metabolism of existing Dopamine
- Withania simnifera: Bioregulate body biokinetics - improve quality of life Hence combinely produce sustained improvement and bioregulate movement synegy ,check degeneration of neural cells in substantia nigra ,trevitalize damaged cell with provision of natural Levodopa (Figures 9 & 10) [18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33].
References
-
Pearce JM (1989) Aspects of the history of Parkinson's disease. J Neurol Neurosurg Suppl: 6-10.
-
Singhal B, Lalkaka J, Sankhla C (2003) Epidemiology and treatment of Parkinson's disease in India. Parkinsonism Relat Disord 9(2): S105-109.
-
De Lau LM, Breteler MM (2006) Epidemiology of Parkinson's disease. Lancet Neurol 5: 525-535.
-
Das SK, Biswas A, Roy T, Banerjee TK, Mukherjee CS, et al. (2006) A random sample survey for prevalence of major neurological disorders in Kolkata. Indian J Med Res 124(2): 163-172.
-
Ragothaman M, Murgod UA, Gururaj G, Louis ED, Subbakrishna DK, et al. (2008) High occurrence and low recognition of Parkinsonism (and possible PD) in old age homes in Bangalore, South India. J Assoc Physicians India 56: 233-236.
-
CM T, DW G, CG G (1990) A brief screening questionnaire for Parkinsonism. Ann Neurol, pp: 267- 88.
-
Behari M, Srivastava AK, Das RR, Pandey RM (2001) Risk factors of Parkinson's disease in Indian patients. J Neurol Sci 190(1-2): 49-55.
-
Streifler M, Hofman S (1984) Disorders of verbal expression in Parkinsonism. Adv Neurol 40: 385-393.
-
Singh S, Behari M (2006) Verbal and visual memory in patients with early Parkinson's disease: Effect of levodopa. Neurol India 54(1): 33-37.
-
Arun MP, Bharath S, Pal PK, Singh G (2011) Relationship of depression, disability, and quality of life in Parkinson's disease: A hospital-based case- control study. Neurol India 59(2): 185-189.
-
Kumar S, Bhatia M, Behari M (2002) Sleep disorders in Parkinson's disease. Mov Disord 17: 775-781.
-
Giovannoni G, van Schalkwyk J, Fritz VU, Lees AJ (1999) Bradykinesia akinesia inco-ordination test (BRAIN TEST): an objective computerised assessment of upper limb motor function. J Neurol Neurosurg Psychiatry 67(5): 624-629.
-
Durif F, Vidailhet M, Debilly B, Agid Y (1999) Worsening of levodopa-induced dyskinesias by motor and mental tasks. Mov Disord 14(2): 242-245.
-
Markham CH, Diamond SG (1981) Evidence to support early levodopa therapy in Parkinson disease. Neurology 31(2): 125-131.
-
Gupta D, Saini J, Kesavadas C, Sarma PS, Kishore A (2010) Utility of susceptibility-weighted MRI in differentiating Parkinson's disease and atypical parkinsonism. Neuroradiology 52(2): 1087-1094.
-
Yadav R, Shukla G, Goyal V, Singh S, Behari M (2012) Knowledge of Parkinson's disease among patients and caregivers attending movement disorder clinic at a tertiary care centre in north India. Ann Indian Acad Neurol 15(4): 294-296.
-
Katzenschalger R, Evans A, Manson A, Patsalos PN, Watt H, et al. (2004) Mucuna Pruriens in Parkinson’s Disease: a Double-blind Clinical and Pharmacological Study. Journal of Neurology, Neurosurgery and Psychiatry 75(12): 2672-2677.
-
Manyam B (1990) Paralysis agitans and levodopa in “Ayurveda”: ancient Indian medical treatise. Mov Disord 5(1): 47-48.
-
Manyam B, Sanchez-Ramos JR (1995) Traditional and complementary therapies in Parkinsońs disease. Adv Neurol 80: 565-574.
-
Damodaran M (1937) Ramaswamy R. Isolation of L- dopa from the seeds of Mucuna pruriens. Biochem J 31(12): 2149-2451.
-
(1995) HP-200 in Parkinson’s Disease Study Group. An alternative medicine treatment for Parkinson’s disease: results of a multicenter clinical trial. J Altern Complement Med 1(3): 249-255.
-
Vayda AB, Rajgopalan TS, Mankodi NA, Antarkar DS, Tathed PS, et al. (1978) Treatment of Parkinsońs disease with the cowhage plant - Mucuna pruriens (Bak). Neurol India 26(4): 171-176.
-
Nagashayana N, Sankarankutty P, Nampoothirir MR, Mohan PK, Mohanakumar KP (2007) Association of L- dopa with recovery following ayurveda medication in Parkinson’s disease. J Neurol Sci 176(2): 124-127.
-
Rinne UK, Sonninen V, Sirtola T (1973) Plasma concentration of levodopa in patients with Parkinson’s disease. Eur Neurol 10(5): 301-310.
-
Mars H (1973) Modification of levodopa effect by systemic decarboxylase inhibition. Arch Neurol 28(2): 91-95.
-
Jaffe M (1973) Clinical studies of carbidopa and L- dopa in the treatment of Parkinson’s disease. Adv Neurol 2: 161-72.
-
Reid JL, Calne DB, Vakil SD, Allen JG, Davies CA (1972) Plasma concentration of levodopa in parkinsonism before and after inhibition of peripheral decarboxylase. J Neurol Sci 17(1): 45-51.
-
Pinder RM, Brogden RN, Sawyer PR, Speight TM, Avery GS 1976) Levodopa and decarboxylase inhibitors: a review of their clinical pharmacology and use in the treatment of parkinsonism. Drugs 11(5): 329-377.
-
Kurth MC, Tetrud JW, Irwin I, Lyness WH, Langston JW (1993) Oral levodopa/carbidopa solution versus tablets in Parkinson’s patients with severe fluctuations: a pilot study. Neurology 43(5): 1036- 1039.
-
Tripathi YB, Upadhyay AK (2002) Effect of the alcohol extract of the seeds of Mucuna pruriens on free radicals and oxidative stress in albino rats. Phytother Res 16(6): 534-538.
-
Kuopio AM, Marttila RJ, Helenius H, Toivonen M, Rinne UK (2000) The quality of life in Parkinson's disease. Mov Disord 15(2): 216-223.
-
Ray J, Das SK, Gangopadhya PK, Roy T (2006) Quality of life in Parkinson's disease-Indian scenario. J Assoc Physicians India 54: 17-21.
-
Shankar A, (2019) Pharmacokinetics of constituent herbs, Pharmacological basis of indigenous therapeutics, 1st (Edn.), Bhalani Publishing House Mumbai.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya