Mechanism and Nutritional Management of Alzheimer’s Disease
Alzheimer’s disease (AD) is one of the most common neurodegenerative disorders in the human population. The symptoms initiated with the forgetfulness and dementia, as a result of neuronal cell death. AD patients have many phases in the progress of the disease such as mild, moderate, and severe stage. Molecular mechanism of the pathogenesis states that there are many factors, which are responsible for the AD such as mutation in the AD associated genes, genetic and environmental factors. Nutrition is also the key factor, which is notified as one of the reason to maintain to avoid the disease progression in patients. Nutrition is the most essential method, which provides a balanced diet for the AD patients. There are numerous agencies, which target the AD patient population for their nutritional management and study for a better understanding. This review article provides short information about the AD patient symptoms, causes, molecular mechanism and nutritional management.
Abbreviations
AD: Alzheimer’s Disesse; Aβ: Β-Amyloid; ESPEN: European Society for Clinical Nutrition and Metabolism; ONS: Oral Nutritional Supplements.
Introduction
Alzheimer’s Disesse (AD) is one of the most common and progressive neurodegenerative disorder mostly in old age which is responsible for dementia worldwide [1, 2]. Statistical data analysis states that 44 million people live with dementia in 2013 globally, with numbers getting twice every 20 years, to reach 135 million by 2050. Dementia increasing risk will be common in low- and middle-income countries. Currently, such locations have 62% of the population with dementia this ratio is increasing to 66% by 2030 and 71% by 2050. The number of the patients will be 106.8 million worldwide by the end of 2050. The AD is an upcoming risk for the public health with socioeconomic concern [3]. The AD corresponds 50–70% among all dementia problems, categorized as a diffuse cortical atrophy with three essential sections of evolution: mild, moderate, and severe. Memory decline, attention, and language impairments can be the symptoms during the disease course, followed by behavioral changes that end up spoiling the performance in basic activities of daily living and problem-solving abilities. Cognition rearrangement and regular physical exercises may lead to reduced risk of the AD, while many factors such as; epsilon 4 alleles of the apolipoprotein, diabetes E gene (APOE 𝜀4), smoking, stress, and depression are associated with increased risk of the AD [4]. From past few years, there are plenty of evidences, which witnessed an essential role of nutrition in the AD [5, 6, 7]. The AD is similar with other chronic diseases, where an innumerable number of interconnected components associated with daily lifestyle, which involves in disease progression [8, 9]. Foods, beverages, and unusual eating habits have been engaged in several epidemiological risk factors [10, 11].
Foods containing saturated fatty acids, high-calorie, and excess alcohol consumption are the most common factors to induce the risk of the AD [12]. Oxidative stress and lipid peroxidation are among risk factors, which is associated with high-fat diets and the AD pathogenesis [13]. Foods, containing factors such as antioxidants, vitamins, polyphenols, and fish, are reported as reduced risk for the AD development. To update the AD progression and required nutrition, this review article contains the study of diet in the AD development.
Molecular Mechanism of AD
The neuropath logical disorder hallmarks are essentially β-amyloid (Aβ) plaques and neurofibrillary tangles/Tau made up of paired helical filaments of hyper-phosphorylated tau proteins. Decrepit plaques are mainly configured with Aβ peptide with 40–42 amino acid fragment of the Aβ precursor (APP) [14] and of Aβ25–35 oligomers [15, 16]. Accumulation of Aβ leads to oxidative stress, neurotoxicity, and inflammation, which can initiate the pathogenic cascade, finally, result to apoptosis and deterioration of the neurotransmission systems [17]. Proteins related with the neurodegenerative disorders such as Aβ, tau and α-synuclein exist in various assembly, and many proves implicate that smaller assembly like soluble oligomers are more pathogenic than larger, insoluble, highly ordered, fibrillary aggregates [18, 19]. Both tau and α-synuclein, both are intrinsically disorganized proteins; it is easily conceivable that even monomers could assume pathogenic conformations under circumstances that promote protein misfolding. The interaction of co-pathogen that have been investigated among tau, apoE4, Aβ and α-synuclein implicate that probably downstream mechanisms on which the effects of these proteins converge. Unusual distribution of neurotransmitter receptors and downstream signaling cascades, excite-toxicity and dysregulation of intracellular calcium homeostasis, alterations in the intracellular transport of critical cargoes, epigenetic dysregulation, mitochondrial impairments, and engagement of pathogenic glial loops are among the possible convergence keys. Illustrated mechanisms are not mutually exclusive. In fact, some of them may be correlated, like intracellular transport deficits and mitochondrial dysfunction. Witnesses supports that an autophagy is the main mechanism, which assist cells to remove abnormal protein aggregates [20]. In autosomal dominant form of AD, mutant presenilin1 (PS1) may damage autophagy directly by hampering proteolysis in a lysosome, whereas in second AD form autophagy impairments may engage various genetic or environmental factors [21].
An interesting feature of Aβ, tau, and α-synuclein together with neurodegenerative diseases is its ability to sustain pathogenesis through cell-to-cell spread and aggregation of abnormal protein in experimental animal models. Well-known fact is neurodegenerative diseases have strong relation with aging. Mutation that accelerates the aggregation of proteins, which is pathogenic in the brain can override the aging and cause AD or another neurodegenerative conditions in adults. Research evidence that neurodegenerative conditions may be activated by aging-related factors, such as dysfunction of neuroprotective protein or its clearance mechanisms. Further, Aβ and apoE4 can provide to network and cognitive dysfunction by impairing certain populations of agonist interneurons that generally control the excitatory principal cell activity. ApoE4 and its fragments influence age and tau- dependent somatostatin-positive GAB Aergic interneurons impairments in the hilus region of the dentate gyrus, leads to deficits of learning and memory. The hypothesis states that neurofibrillary tangles formation cause by mutation in a tau, which leads to malfunctioning microtubule and neurofibrillary tangles (Figure 1).
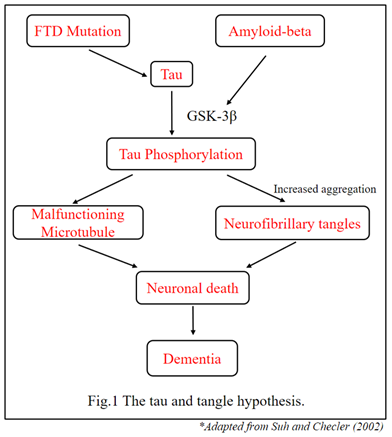
Many other molecular mechanisms responsible for the AD associated with the tau, Amyloid-beta, APOE, PS1, and PS2. They all are essential key factors engaged with the AD pathogenes in old age.
Nutritional Strategy for the AD Patients
In 2015, The European Society for Clinical Nutrition and Metabolism (ESPEN) designed a guideline of nutritional strategies for the patients with dementias and established that the application of oral nutritional supplements (ONS) has high level of significant contribution for the improvement of the nutritional status [22]. Nutritional intervention in such type of cases should be investigated responsibly and depending on the nutritional status of multiple commodities accordingly (Figure 2).
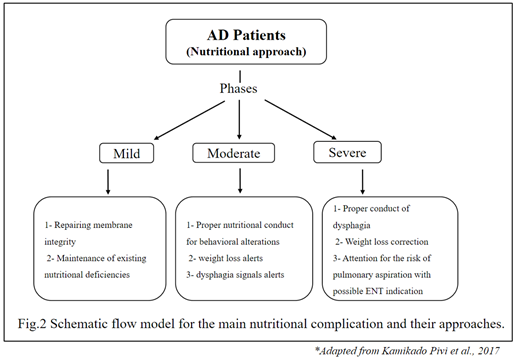
Biological and psychological alterations established with aging, functional capacity, and nutritional requirements of the individual to supply all the essential nutrients and enough amounts to manage a good nutritional condition [23, 24, 25, 26, 27, 28, 29, 30].
Conclusion
Many studies have claimed that the percentage of the AD patients will be huge in 2050. Nutritional strategy is an essential factor, which can affect this condition. Study for the molecular mechanism of the AD requires for the better comprehension about the pathogenesis and treatment of the AD. ONS had provided the guidelines for the nutritional management for the AD patients. A population of the AD patients needed for the study about nutritional management with the help of that way we can minimize the occurrence of the AD in the human population.
References
-
Blennow K, De Leon MJ, Zetterberg H (2006) Alzheimer’s Disease. The Lancet 368(9533): 387-403.
-
Gregory AJ, Sarah AC (2010) Conceptual Evolution in Alzheimer’s Disease: Implications for Understanding the Clinical Phenotype of Progressive Neurodegenerative Disease. Journal of Alzheimer’s disease 19(1): 253-272.
-
Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi MH (2007) Forecasting the global burden of Alzheimer’s disease. Alzheimer’s and Dementia 3(3): 186-191.
-
Williams JW, Plassman BL, Burke J, Benjamin S (2010) Preventing Alzheimer’s disease and cognitive decline. Evidence Report Technology Assessment 193: 1-727.
-
Dosunmu R, Wu J, Basha MR, Zawia NH (2007) Environmental and dietary risk factors in Alzheimer’s disease. Expert Review of Neurotherapeutics 7(7): 887- 900.
-
Lau FC, Shukitt-Hale B, Joseph JA (2007) Nutritional intervention in brain aging: reducing the effects of inflammation and oxidative stress. Sub-cellular Biochemistry 42: 299-318.
-
Shah R (2013) The role of nutrition and diet in Alzheimer disease: a systematic review. Journal of the American Medical Directors Association 14(6): 398-402.
-
Solfrizzi V, Capurso C, D’Introno A, Colacicco AM, Santamato A, et al. (2008) Lifestyle-related factors in predementia and dementia syndromes. Expert Review of Neurotherapeutics 8(1): 133-158.
-
Solfrizzi V, Panza F, Capurso A (2003) The role of diet in cognitive decline. J Neural Transm 110(1): 95-110.
-
Kivipelto M, Solomon A (2008) Alzheimer’s disease - the ways of prevention. Journal of Nutrition, Health and Aging 12(1): 89-94.
-
Heyman A, Wilkinson WE, Stafford JA, Helms MJ, Sigmon AH, et al. (1984) Alzheimer’s disease: a study of epidemiological aspects. Ann Neurol 15(4): 335-341.
-
Ramassamy C, Belkacemi A (2011) Nutrition and Alzheimer’s disease: is there any connection? Current Alzheimer Research 8(5): 443-444.
-
Shie FS, Jin LW, Cook DG, Leverenz JB, LeBoeuf RC (2008) Diet-induced hypercholesterolemia enhances brain A-beta accumulation in transgenic mice. Neuroreport 13(4): 455-459.
-
Glenner GG, Wong WC (1984) Alzheimer’s disease: Initial Report of the Purification and Characterization of a Novel Cerebrovascular Amyloid Protein. Biochemical and Biophysical Research Communications 120(3): 885- 890.
-
Kubo T, Nishimura S, Kumagae Y, Kaneko I (2002) In vivo conversion of racemized beta-amyloid ((D-Ser 26)A beta 1–40) to truncated and toxic fragments ((D-Ser 26)A beta 25–35/40) and fragment presence in the brains of Alzheimer’s patients. J Neurosci Res 70(3): 474-483.
-
Gruden MA, Davidova TB, Malisauskas M, Sewell RDE, Voskresenskaya NI, et al. (2007) Differential neuroimmune markers to the onset of Alzheimer’s disease neurodegeneration and dementia: Autoantibodies to Aβ (25–35) oligomers, S100b and neurotransmitters. J Neuroimmunol 186(1-2): 181-192.
-
Yankner BA (1996) Mechanisms of neuronal degeneration in Alzheimer’s disease. Neuron 16(5): 921-932.
-
Morris M, Maeda S, Vossel K, Mucke L (2011) The many faces of tau. Neuron 70(3): 410-426.
-
Winner B, Jappelli R, Maji, et al. (2011) In vivo demonstration that -synuclein oligomers are toxic. Proceedings of the National Academy of Sciences 108: 4194-4199.
-
Harris H, Rubinsztein DC (2011) Control of autophagy as a therapy for neurodegenerative disease. Nat Rev Neurol 8(2): 108-117.
-
Nixon RA, Yang DS (2011) Autophagy failure in Alzheimer’s disease-locating the primary defect. Neurobiology of Disease 43(1): 38-45.
-
Volkert D, Chourdakis M, Faxen-Irving G, Fruhwald T, Landi F, et al. (2015) ESPEN guidelines on nutrition in dementia. Clin Nutr. 34(6): 1052-1073.
-
Sousa VMC, Guariento ME (2009) Avaliação do idoso desnutrido. Rev Bras Clin Med 7(1): 46-49.
-
Selkoe DJ (2001) Alzheimer’s Disease: Genes, Proteins, and Therapy. Physiological Reviews 81(2): 741-746.
-
Song MS, Rauw G, Baker GB, Kar S (2008) Memantine Protects Rat Cortical Cultured Neurons against Beta-Amyloid-Induced Toxicity by Attenuating Tau Phosphorylation. European Journal of Neuroscience 28(10): 1989-2002.
-
Lopez OL, DeKosky ST (2003) Neuropathology of Alzheimer’s disease and Mild Cognitive Impairment. Review Neurology 37(2): 155-163.
-
Wollen KA (2010) Alzheimer’s Disease: The Pros and Cons of Pharmaceutical, Nutritional, Botanical, and Stimulatory Therapies, with a Discussion of Treatment Strategies from the Perspective of Patients and Practitioners. Alternative Medicine Review 15(3): 223- 244.
-
Borchelt DR, Ratovitski T, Van Lare J, Lee MK, Gonzales V, et al. (1997) Accelerated Amyloid Deposition in the Brains of Transgenic mice Coexpressing Mutant Presenilin 1 and Amyloid Precursor Proteins. Neuron 19(4): 939-945.
-
Huang Y, Mucke L (2012) Alzheimer Mechanisms and Therapeutic strategies. Cell 148(6): 1204-1222.
-
Vasantharaja R, Kumar A, Kumar A, Subramaniam JR (2016) Reserpine Improves Working Memory. Journal of Behavioral and Brain Science 6: 107-112.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya