Effects of “Fall Risk Assessment Training” on Knowledge and Skills of Nurses
The context of escalating need for government funded health care services encourages policymakers to develop new enterprises which can relieve demand for statutory services. This concept based article reports a scoping review designed to identify priorities for a research agenda of organisational studies which can examine these enterprises, and their emerging relational networks, within an expanding health and wellbeing sector. The review includes a thematic analysis in which transferable learning from recent ethnographic studies in Australia and the United Kingdom is presented. This is supported by lessons drawn from expert subject advice in follow up research projects and applications. The two countries were originally selected because of their rapid new development of wellbeing services. Overall findings point to distinct types of relational network, and informal leaderships emerging to facilitate wider access to social enterprises and informal health and wellbeing services. As ‘actor networks’ these are classified by their material features. Spiritual leaders and resources are shown to contribute significantly to these networks, which also incorporate sports, arts and therapeutic practices. With public health and social care strategically aligned in many market based systems globally, the review concludes that research on alternative network development processes is required for local authorities with community development responsibilities. Overlapping relationships between alternative networks may offer the prospect of more holistic approaches to public health and health care quality that reduce pressures on government funded interventions.
Introduction
Providing safety to the patients is vital in the healthcare industry. Patient safety means prevention of direct or indirect harm or injury to the patient. All healthcare personnel are equally responsible in providing safety to their patients. Nurses being vital and larger workforce of the hospital, play a major role in providing safety to their patients by preventing hospital acquired infections, negligence and errors, falls, injuries, and other incidences.
“Patient falls” in the hospital lead to injuries, disabilities and increased hospital stay. It not only affects their quality of life, but also increases the economic burden on the patients and their families as well as the hospital. Pacific Institute for Research and Evaluation (PIRE publication) [1] reported an increase in the mortality of such patients by 71% between 2000 to 2009. Houry, et al. [2] predicted rise in number of “patient falls” and cost of the treatment involved therein. Number of falls with fatal outcome among older adults with age 65 years and above, are predicted to reach almost 100,000
per year by 2030 and medical cost of treating these patients is projected to increase from $35 billion to over $101 billion2. This vividly reflects upon need to prevent such incidences. All healthcare professionals must know how to assess “fall risk” so that appropriate preventive measures can be taken [2].
In-patient (patients admitted in the hospital) falls is a major concern in the hospitals worldwide. Most of the times, in-patient fall rate is underreported by the nurses and other healthcare personnel, equally from developed and developing countries, due to the risk of losing job, stigma of negligence and its consequences.
Nurses from developed countries are trained to assess patients risk for fall and may have standards and/or policies and protocols for fall risk assessment, reporting system and further management of such incidences. On the contrary, developing countries like India, lack such standards, policies and protocols, and research activities. Additionally, routine practices of assessing patient for fall are also missing in public and private hospitals. Hence, it is important to investigate nurses’ knowledge and skills to perform fall risk assessment on their patients.
The aim of this study was to evaluate effectiveness of fall risk assessment training on knowledge and skills of nurses working in in-patient units of selected multispecialty teaching hospital.
Methodology
Most patient falls were reported from male and female medicine wards of the selected hospital. Hence, 22 nurses working in these medicine wards in morning and evening shifts were purposefully selected as study samples. Convenient purposeful sampling technique was used for the same.
Ethical approval was obtained from the selected hospital before the study. Informed written consent was obtained from the hospital authority, selected nurses as well as selected patients. Privacy, confidentiality, anonymity, protection of data, etc was maintained throughout the study.
Study Hypotheses
- H1: Fall risk assessment training improves knowledge of nurses.
- H2: Fall risk assessment training improves skills of nurses.
Data Collection
Content and construct validity of training module and power point presentation as well as case study was assessed and approved by experts from hospital administration, nursing and physiotherapy department. Fall risk assessment tool was developed based on the literature reviewed [3, 4]. Pearson’s correlation coefficient for this tool was 0.89, thus had strong reliability. Patient fall risk assessment tool consisted to test knowledge and skill on items like age, fall history, transfer ability, mobility level, medication, patient care equipment, balance and gait, mental status, environmental hazards, personal history, elimination- bowel and urine. Each item needs to be tick (• ) marked as applicable for individual patient.
Pre and post test was conducted to test knowledge of nurses, before and after the fall risk assessment training. This was case study based test. An additional post test was conducted on the next day of training to evaluate whether nurses can apply given knowledge on an actual patient means to test their skills. For this, 22 nurses were randomly (by picking up chit paper which mentioned group number) divided in 5 groups in which 3 groups had four nurses each and 2 groups had five nurses each. Each group was allotted one patient to conduct fall risk assessment and each member of the group assessed their patient individually. One of the researchers also conducted fall risk assessment on these selected patients so that nurses’ assessment could be judged and compared with.
Results
All nurses participated in this study had completed their general nursing and midwifery diploma programme. Majority of nurses (68%) were between 26-40 years of age (Table 1). 32% of nurses were below 25 years of age. Table 1 shows that 73% of nurses had less than 7 years and 27% nurses had more than 8 years of work experience.
| Age group of nurses | Experience | Percentage | ||||||
|---|---|---|---|---|---|---|---|---|
| 21-25years | 0-2 years | 32% | ||||||
| 26-30 years | 2-7 years | 41% | ||||||
| 31-35 years | 8-13years | 23% | ||||||
| 36-40 years | >13 years | 4% |
Table 1: Percentage of nurses according to their age and experience.
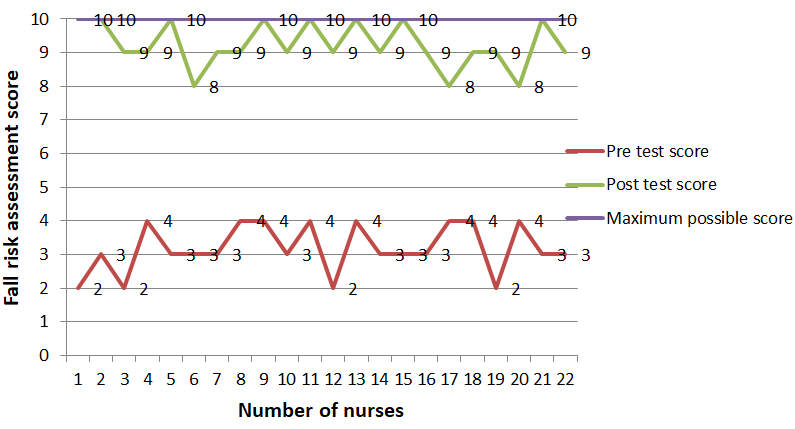
Figure 1 show expected maximum score for the pre and posttest was 10. The average test score of nurses was 3.18 out of 10 before the training, which improved to 9.23 after the training. It means nurses’ pretest score was much lesser but showed improvement in posttest which confirms that fall risk assessment training was effective in increasing knowledge of nurses.
Researchers applied paired t test to compare difference between deviation of scores before and after fall risk assessment training. Table 2 shows since p value was less than 0.05 (i.e. 0.00) difference in deviation scores is statistically significant. Researchers concluded at 5% level of significance and 21 degrees of freedom that the mentioned data in Table 2 gives sufficient evidence to conclude that the deviations in fall risk assessment scores by nurses showed significantly less deviation from expected maximum score(10) as compared to their deviation before fall risk assessment training. Hence, researchers accept research hypothesis one and two. It can be concluded that, the fall risk assessment training for nurses from medicine wards was proved to be effective in improving knowledge related to fall risk assessment.
- Test
- Mean (Deviation from
- SD (Deviation from
- Paired ‘T’ test expected score) expected score) value
- Pretest (Before fall risk assessment training)
- 6.8
- 0.7
- 27.1
- 21
- 0
- Posttest (After fall risk assessment training)
- 0.8
- 0.7
Table 2: Comparison of fall risk assessment score deviation from expected score.
As mentioned earlier the skills of fall risk assessment of nurses were also assessed by allocating one patient each to every group of nurses on next day of training. Researcher also assessed all these patients. Table 3 gives details of number of nurses per group and their scores along with the researchers score. Researcher’s score indicates that four patients had moderate risk for fall and one patient had low risk for fall. There was minor difference of scores of nurses as compared with the researchers fall risk assessment score of the assigned patient. This table also confirms that selected nurses could perform fall risk assessment on an actual patient as good as researcher herself. Additionally, it shows training session was effective and inter rater assessment did not show significant difference in the score.
| Group | Number of nurses | Researchers score of fall | Number of nurses and their score of fall | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| number | in a group | risk assessment of patient | risk assessment of patient | ||||||||
| 1 | 4 | 17 | 2 scored 17 2 scored 16 | ||||||||
| 2 | 4 | 16 | 3 scored 16 1 scored 15 | ||||||||
| 3 | 4 | 11 | All 4 scored 11 | ||||||||
| 4 | 5 | 14 | 3 scored 14 2 scored 13 | ||||||||
| 5 | 5 | 14 | 2 scored 14 3 scored 13 |
Table 3: Comparison of fall risk assessment scores of nurses with the researcher’s score.
“Patient Falls” result in increased morbidity, mortality and cost. Morello, et al. [5] reported 1330 falls and 418 injuries thereof, in the year 2011-2013 in Australia, which increased length of hospital stay and cost of treatment. Spetz, et al. [6] estimated more than 1million indoor patient falls to occur in hospitals per year increasing the financial burden for their treatment. Scuffham, et al. [7] detailed the cost per 10000 population as £300000 in the 60–64 age group, increasing to £1500000 in the >75 age group. These falls cost the UK government £981 million (2003. pg741). Verma, et al. [8] study mentioned that, cost of this treatment was 111 billion U.S. dollars in the year 2010. Center for disease control and prevention, USA, reported total medical cost for such falls as $50 billion in 2015. Fields, et al. [9] reported that within three years, 530 indoor patients faced such incidences in Bostan, USA and overall cost of imaging (including X-Ray, CT scan, MRI) services was $160,897.
Falls among hospital in-patients are common but complex phenomena. Because many factors contribute towards it [10, 11]. For example, factors from patients’ perspective, environmental perspective, organizational perspective etc. It means patient’s health, age, gender, his/her response to the disease condition, available resources, hospital infrastructure etc. contribute towards patient’s fall. Although fall is common in elderly patients, other patients who have sensory deprivation, endocrine disorders, nutritional deprivation and deficiencies and patients with fluid-electrolyte imbalance are equally vulnerable. It means all age groups of patients are likely to be affected due to falls [12]. Hence, to be on the safer side, every in-patient needs to be screened for fall risk assessment and nurses need to be trained for the same.
Although in-patient fall can be anticipated number of times; but still it is considered as an accidental/ inadvertent event, where patient descends downwards without any intimation or warning and may or may not result in direct or indirect injury or harm. Hence, to prevent in- patient fall multidisciplinary, Nursing training programme on this subject is a simple, easy to implement, effective and economic method to mitigate and prevent patient falls in the hospital. With this method, the nursing staff becomes aware of high risk patients and can pay more attention and take necessary precautions to reduce such incidences, thus paying a vital role. They need to have appropriate knowledge and skill to assess the risk for falls. Yuan Gu, et al. [14] confirms the same. Such training programmers enhance the quality care for the patients and lower the cost of treatment at the same. Nurses being central force in the hospital, play a major role in assessing patients for fall. Fall risk assessment training helps them to conduct such assessment effectively.
This study evaluated effectiveness of planned training on knowledge and skills of nurses related to fall risk assessment. The results of this study confirm that there was improvement in knowledge and skills of nurses after a single, short duration fall risk assessment training session. At the end of training, selected nurses’ knowledge and skills test scores were nearer to the expected maximum score. These results also provide evidence that nurses were able to conduct effective fall risk assessment on actual patient after the training session. Likewise, et al. [15] revealed that nurses’ knowledge and skills related to fall risk assessment was improved after the training.
Fall risk assessment training of nurses is important because it not only helps to prevent and reduce patients’ falls but also increases annual savings of hospital [16]. For example Singh, et al. [15] reported during subsequent consecutive three years, the rate of patient fall was consistently reduced; and later it helped for annual saving of £642,055. Training programme in this study was economic method to educate nurses on patient fall risk assessment. Although actual cost of training programme was not the focus of this study.
Main concern is many hospitals neither have standard policies and procedures nor training programmers for assessing and preventing falls especially in India [16]. Hence, it is of vital importance to develop in-service training programmers for nurses including designing patient fall assessment form. Importantly, each and every patient need to be assessed on admission and later on as and when needed i.e. post-operative, after sensory deprivation, after medication administration etc [16].
Few limitations were observed in the current study; for example, time limitation was a major constrain and retention, recalling of knowledge and skills of nurses were observed immediately on the same day and on the next day rather than after weeks or months.
Conclusion
Majority of patients’ fall are preventable and fall risk assessment is one step to achieve it. The purpose of this study was to determine whether or not a training session would make a difference in nurses’ knowledge and skills regarding fall risk assessment. The study findings confirmed that nurses who received single, short duration fall risk assessment training had significant increase in their knowledge and skills related to the same. Fall risk assessment training had integrated theoretical and practical components hence showed its impact on increasing knowledge and skills score of the participants. This is cost effective method to reduce patient falls in the hospital settings.
Both the authors agreed with the study findings and no conflict of interest in this study.
References
-
Ian R, Michael D, Nestor D, Jeffrey H, Ted R, et al. (2009) Leading causes of unintentional and intentional injury mortality: United States, 2000- 2009.
-
Houry D, Florence C, Baldwin G, Stevens J, McClure R (2016) The CDC injury center's response to the growing public health problem of falls among older adults. Am J Lifestyle Med 10(1): 74-77.
-
Hendrich AL, Bender PS, Nyhuis A (2003) Validation of the Hendrich II fall risk model: A large concurrent case/control study of hospitalized patients. Appl Nurs Res 16(1): 9-21.
-
Oliver D, Daly F, Martin FC, McMurdo ET (2004) Risk factors and risk assessment tools for falls in hospital in -patients: a systematic review. Age and aging 33(2): 122-130.
-
Morello, Barker AL, Watts JJ, Haines T, Zavarsek SS, et al. (2015) The extra resource burden of in- hospital falls: a cost of falls study. Med J Aust 203(9): 367.
-
Spetz J, Brown D, Aydin C (2015) The economics of preventing hospital falls. J Nurs Adm 45(1): 50-57.
-
Scuffham P, Chaplin S, Legood R (2003) Incidence and costs of unintentional falls in older people in the United Kingdom. J Epidemiol Community Health 57(9): 740-744.
-
Verma SK, Willetts JL, Corns HL, Marucci Wellman HR, Lombardi DA, et al. (2016) Falls and Fall-Related Injuries among Community-Dwelling Adults in the United States. PLoS ONE 11(3): e0150939.
-
Fields J, Alturkistani T, Kumar N, Kanuri A, Salem DN, et al. (2015) Prevalence and cost of imaging in inpatient falls: the rising cost of falling. Clinicoecon Outcomes Res 7: 281-286.
-
Nakai, Akihito, Akeda, Masami, Kawabata I (2006) Incidence and Risk Factors for Inpatient Falls in an Academic Acute-care Hospital. J Nippon Med Sch 73(5): 265-270.
-
Hendrich A (2007) How to try this: Predicting Patient Falls-Using the Hendrich II Fall Risk Model in Clinical Practice. Am J Nurs 107(11): 51-58.
-
Hitcho, Krauss MJ, Birge S, Claiborne Dunagan W, Fischer I, et al. (2004) Characteristics and circumstances of falls in a hospital setting a prospective analysis. J Gen Intern Med 19(7): 732- 739.
-
Spoelstra, Sandra, Given, Barbara, Given C (2012) Fall Prevention in Hospitals : An Integrative Review. Clin Nurs Res 2: 1-28.
-
Gu YY, Balcaen K, Ni Y, Ampe J, Goffin J (2016) Review on prevention of falls in hospital settings. Chinese nursing research 3(1): 7-10.
-
Inderpal S, Okeke J (2016) Reducing inpatient falls in a 100% single room elderly care environment: evaluation of the impact of a systematic nurse training programme on falls risk assessment. BMJ Quality Improvement Reports 5(1): u210921.
-
Atay S, Vurur S, Erdugan N (2016) Opinions of nurses about the evaluation of risk of falling among inpatients. Rehabil nurs 42(6): E19-E24.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda