Non‑Melanoma Skin Cancer (NMSC): Extramammary Paget ’s Disease
Non-melanoma skin cancer (NMSC) comprises squamous cell carcinoma (SCC), basal cell carcinoma (BCC), and several rare skin tumors (i.e., Extramammary Paget’s disease), being the most common malignancy affecting people worldwide. It represents the majority of skin cancers and a significant percentage of all malignancies. Despite increasing public awareness and scientific interest, the incidence of NMSC is constantly increasing. Even though most NMSC`s are associated with less aggressive behavior, they can still be invasive locally and cause extensive damage to neighboring structures, inducing significant morbidity. Also, different types and subtypes of NMSC tend to have frequent recurrences and may have significant metastatic potential. As a direct consequence, NMSC has become an important issue for healthcare systems with a significant socio-economic impact.
Extramammary Paget’s Disease (EMPD)
EMPD localized to the vulva is a rare disease that can mimic different types of dermatosis and only four cases have been reported in our practice in the last 5 years.
Definition
EMPD, according to World Health Organization, is a rare intraepithelial neoplasm characterized histopathologically by a prominent growth of large cells, with apocrine or eccrine glandular-like pattern, originating in the skin (primary EMPD) or representing intraepithelial spread of a hidden visceral carcinoma (secondary EMPD). This type of disease is represented by the International Classification of Diseases for Oncology with the following code: 8542/3 [1, 2].
EMPD is a marginated plaque that clinically and histologically resembles Paget’s disease, but occurs in sites rich in apocrine glands, such as vulva, anogenital region and axilla. Currently, there is controversy as to how often this condition appears against on the background of an underlying carcinoma and how often it occurs primarily in the epidermis or apocrine ductal tissue in the affected area. This gave rise to the concept of primary and secondary extra- mammary Paget’s disease [3, 4].
Epidemiology and Etiology
EMPD accounts for about 1 % of all ano-genital neoplasms. It develops more frequently in Caucasian women in the postmenopausal period [1] and usually begins in the fifth decade or later. Current opinion is that, in about 75% of cases, extracellular Paget’s disease appears as a primary intra-epidermal neoplasm, possibly from ductal cells of the apocrine gland or keratinocyte stem cells. Another possible origin may be the Toker’s cells [3, 5]. In the remaining 25% of cases, there is a hidden primary adenocarcinoma. These cases are referred as secondary Paget’s disease.
Only a few cases of association between mammary and vulvar Paget’s disease have been described. Under extraordinary circumstances, EMPD is a secondary event caused by extension of an adenocarcinoma either of the rectum to the perianal region, or of the cervix to the vulvar region. On the other hand, genital Paget’s disease with a long evolution can extend into the cervix and urinary tract [6].
Localization
The labia majora is the most widespread site, followed by the labia minora and clitoris. The perineum, perianal area, scrotum, penis, lower abdomen and inguinal folds can also be affected [1].
Based on origin, several classification schemes have been proposed: Type 1: Primary vulvar cutaneous origin Type 2: Secondary to primary anal or rectal adenocarcinoma Type 3: Secondary to urothelial carcinoma OR Type I: Paget disease of primary cutaneous origin Ia: As a primary intraepithelial neoplasm Ib: As an intraepithelial neoplasm with invasion Ic: As a manifestation of underlying adenocarcinoma of skin appendage or vulval glandular origin Type II: Paget disease of noncutaneous origin IIa: Secondary to anorectal carcinoma IIb: Secondary to urothelial neoplasia IIc: As a manifestation of another noncutaneous carcinoma: endocervical, endometrial or ovarian adenocarcinoma, etc.
Clinical Features
The most common presentation is a relatively well- demarcated flat or slightly elevated, scaly, erythematous patch or plaque, accompanied by itching or burning, often simulating eczema. Unusual forms include lesions with hyper- or hypopigmentation and multi-centric bruising [1].
EMPD lesion has many features in common with Paget’s disease of the nipple. The edges are sharp, rounded and slightly raised, and include an area that is pink or red. The affected area may be tiled, and small, gray-colored crusts may cover erosion. Itching is an essential feature and there may be excoriations or lichenification. Areas of fluctuating hyperpigmentation may be present, causing confusion between extra-mammary Paget’s disease and superficial spread melanoma. In some cases, leukoplakia may be present [3, 7, 8, 9].
The clinical presentation of the disease varies by site, the most frequent involved being vulva. The first symptom, especially in vulvar lesions, is itching and burning, which can be persistent and growing. It is often seen as dermatitis and may be disturbed by topical therapy. The surfaces of the lining of the labia are periodically redder than the skin when both areas are involved, and the change may proliferate towards the thighs, mons pubis and vaginal introitus. There will be a limited papillomatous area. Characteristic clinical features include fierce advancement, challenging all local applications, and the whetted margin. Eventually, one area may become thickened and ulcerated as evidence of downwards invasion. Lymph nodes involvement or distant metastases can appear. Although most cases of primary carcinoma result from a hidden adenocarcinoma of the sweat gland, it is essential to examine the patient for evidence of a later adenocarcinoma hidden in the cervix and rectum [3].
Pathogenesis
Histogenesis of primary EMPD is unknown [1]. Paget cells in the epidermis may appear as an in situ upward extension of an adenocarcinoma located in the deeper glands. Alternatively, EMPD may have a multifocal primary origin in the epidermis and skin appendages, and does not represent an epidermotropic spread or metastasis from an intrinsic carcinoma of the sweat gland. It can be shown that almost 25% of EMPD originates from primary adenocarcinoma of the secretory glands. Primary tumor and Paget cells are usually mucus secretory [10].
At one point, it was widely accepted that in primary EMPD, Paget cells in the epidermis are due to an in-situ upward extension of an in-situ adenocarcinoma of the sweat glands along the eccrine or apocrine ducts. This theory is comparable to the generally accepted view that secondary EMPD shows an extension of a cervical, rectal or urinary adenocarcinoma and that the progression of Paget breast disease is an extension of a lactiferous canalicular epidermotropic carcinoma. The fact that a hidden adenocarcinoma often could not be demonstrated, can be explained by the different anatomic characteristics between the breast, which has only 20 large, conspicuous lactiferous ducts, and the genital skin, which has thousands of small apocrine and eccrine glands, making the localization of this particular small gland invaded by carcinoma increasingly difficult [6].
Histopathology
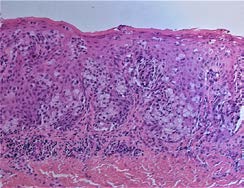
EMPD disease has in common with Paget’s disease the presence of varying numbers of Paget cells within the epidermis (Figure 1). In some cases, the Paget cells are found to be limited to the acanthotic epidermis, accompanied by hyperkeratosis, parakeratosis, erosion or ulceration. Frequently, Paget cells can be identified within the epithelium of hair follicles or eccrine sweat ducts. This types of in situ malignancy associated with EMPD has the same favorable prognosis as EMPD limited to the epidermis. However, the prognosis is much worse in cases in which the Paget cells have invaded the dermis from the epidermis or from an underlying sweat gland carcinoma. Glandular clusters with a central lumen, absent in mammary Paget’s disease may be identified in the lower epidermis in extra-mammary Paget’s disease [6].
Serial sectioning of excised lesions of vulvar EMPD demonstrated that the lesions within the epidermis and its appendages have a multifocal origin. In the cases that have extensive epidermal lesions, the involvement of eccrine glands and ducts is occasionally, and the involvement of apocrine glands and ducts is absent, even if some Paget cells form apocrine glandular structures in the epidermis. Despite the existence of cohesion between the epidermal and the ductal foci, no one can definitive say that the extension is in an up or down direction. The dermal invasion in EMPD has its beginning point in the epidermis and not ductal or glandular structures.
The origin of the Paget cell may be the poral portion of an apocrine duct, or the pluripotential germinative cells within the epidermis [6]. Paget cells have an abundant basophilic to amphophilic cytoplasm and vesicular nuclei with pronounced nucleoli. They are generally distributed in a solitary fashion or may form gland-like structures or well- demarcated solid nests. Involvement of adnexa (hair follicles and eccrine ducts) is seen in most cases. Rarely, single cells, glands and solid nests can be found in the dermis; this is considered to be microinvasion. Dermal invasion is rare in vulvar EMPD, more common in perianal region. However, this type of microinvasion cannot be applied in cases that are associated with an underlying adenocarcinoma with a ductal in-situ component [1].
Immunohistochemistry
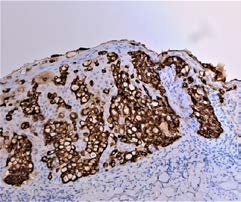
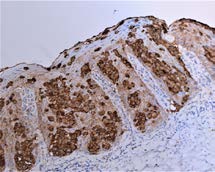
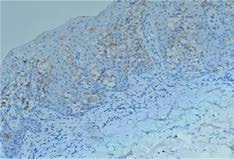
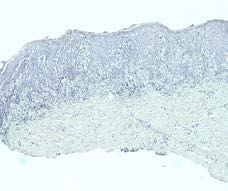
Immunohistochemical staining shows that Paget cells stain consistently positive for CK7 (cytokeratin 7) [1] (Figure 2) and EMA (Epithelial membrane antigen)-used by pathologists like a marker of Paget disease [11] (Figure 3).
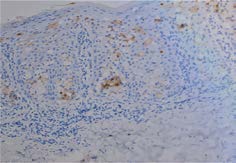
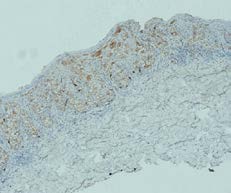
Paget cells often express GCDF-P15 (gross cystic disease fluid protein) (Figure 4), ERBB2 (HER2/neu) (Figure 5), CEA (carcynoembrionic antigen), CA125 (cancer antigen 125 / MUC16), and AR (androgen receptor) [1].
Differential Diagnosis
For correct diagnosis, immunohistochemistry and clinicopathological correlation are essential [1].
The most pressing matter is distinction between primary and secondary EMPD (Table 1). Potential imitators of EMPD are Toker vulvar cells, vulvar and penile analogues of cervical stratified mucin-producing intraepithelial lesion, high- grade squamous intraepithelial lesion, melanoma, pagetoid dyskeratosis, and clear cell papulosis [1].
| Immunohistochemical marker | Primary extra-mammary Paget’s disease | Secondary extra-mammary Paget’s disease | Bowen’s disease | Superficial spreading melanoma |
|---|---|---|---|---|
| CK7 | + | + | + or - | - |
| EMA | + | + | ||
| CEA | + | + | - | - |
| GCDFP-15 | + | - | - | - |
| Melan-A | - | - | - | + |
| P63 | - | - | + | |
| S100 protein | - | - | - | + |
| HMB45 | - | - | - | + |
Table 1: Differential diagnoses of Extra-mammary Paget’s disease (Immunohistochemical Markers) [12].
For differential diagnosis with superficial spreading melanoma we currently use as immunohistochemical markers S100 protein and HMB45 (Figure 6) and we do not use Melan-A because it has often given false positive results (Figure 7).
For proper localization of a large perineal lesion (vulvar or perianal) we usually use GCDFP-15 (positive for vulvar localization) and CK20 (positive for perianal localization) [13].
Prognosis and Treatment
Primary EMPD’s prognosis generally is better than that of mammary Paget’s disease [6]. Local recurrence is frequent, even in cases with a wide surgical extraction, the recurrence rate being 12-58%. This may be related to positive surgical margins, skip areas, and multicentricity.
Adverse prognosis is associated with increased serum levels of CEA and the depth of invasion. Proper tissue sampling and other investigations are vital to determine if there is an associated underlying malignancy that requires surgical excision. If such a malignancy exists, it should be excised along with all clinically abnormal epithelium. If no underlying malignancy is clinically and surgically detected on careful examination, the entire affected area of skin should be excised.
In the case of primary EMPD associated with an invasive component, the prognosis is significantly worse, and it can undergo lymph node metastasis. Cases with gene mutation of PIK3CA and AKT1 are often invasive [1].
An important method is “Mohs surgery” (microscopically controlled surgery) that minimizes the recurrence rate by carefully controlling excision margins of the tumor [14, 15, 16]. Photodynamic therapy is another important tool in the treatment of EMPD, but it requires larger series and longer periods of follow-up [17, 18]. Topical imiquimod has been used with good results in cases with limited disease [19]. Radiation therapy has been supported either as an adjuvant to surgical therapy [20] or as an alternative therapy for elderly patients in whom surgery may have a greater risk [21, 22].
Discussions
Because of the resemblance of the lesions in the EMPD with other dermatological conditions, it is important that the clinician always consider a possible diagnosis of EMPD, especially in the case of lesions in the genital and anal spheres.
Due to the false positive results that may appear at various markers used for the diagnosis of EMPD, the pathologist cannot always rely on immunohistochemical tests for differential diagnosis with other disorders. Therefore, a correlation between clinical, paraclinical and histopathological data is very important for a correct diagnosis.
Conclusion
EMPD is a very rare skin malignancy that needs to be diagnosed and treated accordingly. Because it can mimic a lot of benign or malignant diseases, a correct differential diagnosis is crucial for the treatment and prognosis of the patient. Also, it is imperative to differentiate primary EMPD from a secondary type, in the latest the identification of the primary site of the tumor being vital for the patient.
Author Contributions
All authors had equal contribution in this study elaboration.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Elder DE, Massi D, Scolyer RA, Willemze R (2018) WHO Classification of skin tumours. 4th (Edn.), International Agency for Research on Cancer, Lyon, pp: 217-218.
-
Kurman RJ. Carcangiu ML, Herrington CS, Young RH (2014) WHO Classification of Tumours of Female Reproductive Organs. 4th (Edn.), International Agency for Research on Cancer, Lyon 6: 236-237.
-
Burns T, Breathnach S, Cox N, Griffiths C (2010) Rook’s Textbook of Dermatology. 8th (Edn.), Chapter 53, John Wiley & Sons 4: 2700-2701.
-
Lloyd J, Flanagan AM (2000) Mammary and extramammary Paget’s disease. J Clin Pathol 53(10): 742-749.
-
Willman JH, Golitz LE, Fitzpatrick JE (2005) Vulva clear cells of Toker: precursors of extramammary Paget’s disease. Am J Dermatopathol 27(3): 185-188.
-
Elder DE, Elenitsas R (2009) Lever’s histopathology of the skin. 10th (Edn.), Lippincott Williams & Wilkins, pp: 839-840.
-
Curtin JP, Rubin SC, Jones WB, Hoskins WJ, Lewis JL (1990) Paget’s disease of the vulva. Gynaecol Oncol 39(3): 374-377.
-
Goldblum JR, Hart WR (1997) Vulvar Paget’s disease. Am J Surg Pathol 21(10): 1178-1187.
-
Fanning J, Lambert HC, Hale TM (1999) Paget’s disease of the vulva: prevalence of associated vulvar adenocarcinoma invasive Paget’s disease, and recurrence after surgical excision. Am J Obstet Gynaecol 54(5): 311- 312.
-
Fitzpatrick TB, Johnson RA, Wolff K, Polano MK, Suurmond D (1997) Color Atlas and Synopsis of Clinical Dermatology: common and serious diseases. mcgraw- hill health professions division pp: 1009-1010.
-
Kuan SF, Montag AG, Hart J, Krausz T, Recant W (2001) Differential expression of mucin genes in mammary and extramammary Paget’s disease, Am J Surg Pathol 25(12): 1469-1477.
-
Filho LLL, Lopes IM, Lopes LR, Enokihara MM, Michalany AO, et al. (2015) Mammary and extramammary Paget’s disease. An Bras Dermatol 90(2): 225-231.
-
Hale CS (2012) Skin nonmelanocytic tumor-Extrammary Paget disease. Pathology outline.
-
Lee SC, Roth LM, Ehrlich C (1977) Extramammary Paget’s disease of the vulva. Cancer 39: 2540.
-
Stacy D, Burrell MO, Franklin EW (1986) Extramammary Paget’s disease of the vulva and anus: use of intraoperative frozen sections, Am J Obstet Gynaecol 155(3): 519-522.
-
Thomas CJ, Wood GC, Marks VJ (2007) Mohs micrographic surgery in the treatment of rare aggressive cutaneous tumours: the Geisinger experience. Dermatol Surg 33(3): 333-339.
-
Shieh S, Dee AS, Cheney RT (2002) Photodynamic therapy for the treatment of extramammary Paget’s disease. Br J Dermatol 146(6): 1000-1005.
-
Raspagliesi F, Fontanelli R, Rossi G (2006) Photodynamic therapy using a methyl ester of 5 aminolevulinic acid in recurrent Paget’s disease of the vulva: a pilot study. Gynecol Oncol 103(2): 581-586.
-
Berman B, Spencer J, Villa A (2003) Successful treatment of extramammary Paget’s disease of the scrotum with Imiquimod 5% cream. Clin Exp Dermatol 28(S1): 36-38.
-
Guerrieri M, Back MF (2002) Extramammary Paget’s disease: role of radiation therapy. Australas Radiol 46(2): 204-208.
-
Yanagi T, Kato N, Yamane N (2007) Radiotherapy for extramammary Paget’s disease: histopathological findings after radiotherapy. Clin Exp Dermatol 32(5): 506-508.
-
Nagarajan P (2015) Vulva & female urethra - Glandular tumors. Paget disease.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda