Effect of Providing “Intra-operative Status Information” on Family Members’ Anxiety
Introduction: The family members in the waiting lounge of the operation theatre, when their loved one is undergoing surgery, face certain levels of anxiety and as the time passes, their anxiety increases. This study is aimed at evaluating the effects of providing patient’s intra-operative status information on the anxiety of the family members, during this waiting period. Methodology: A quasi-experimental pre and post-test study design was used in this study. Convenience samples of 50 family members i.e. 25 in control group and 25 in experimental group participated. Spielberger’s State and Trait anxiety inventory (STAI) Form Y-1 and Form Y-2 were used to assess anxiety scores of family members before and after the surgery. Results: Pre-test result showed no significant difference in the state and trait anxiety of family members from both the groups. However, at the end of the surgery i.e. post-test result showed significant difference (P<0.01) in state anxiety of family members from both the groups. Conclusion: Study findings confirmed that patients “intra-operative status information” minimized state anxiety of family members. Adequate assessment of family members’ anxiety and appropriate intervention to decrease the same has implications for intra-operative practices in the hospitals.
Introduction
The family members in the waiting lounge of the operation theatre, when their loved one is undergoing surgery, face certain levels of anxiety not only about the life and safety of their dear one, but they are also curious and eager to know about what is happening inside the operation theatre. They are obviously in desperate need of the information on these issues and as the time passes, their anxiety increases.
The family members of the patient are anxious during the intra-operative waiting period [1]. This anxiety is of temporary period, hence, called as “State anxiety.” Whereas Trait anxiety is how individual generally feels, his/her tendency/characteristics. Trimm, et al. [2] stated that stress and anxiety during waiting period in the hospital and surgery enhances physical and psychological reaction of the family members. Psychological support to these family members during this period when their loved one is undergoing surgery is fundamental and imperative [3, 4].
The family faces certain levels of anxiety while sitting in the waiting lounge outside the operation theatre. This experience is almost similar irrespective of their nationality, culture, education, socio-economic status, age and gender. When the family has control over the situation, they may be able to manage their anxiety. On the contrary, the family members experiences loss of control over the situation and their emotions due to lack of information from the hospital staffs or when they are unable to acquire information from any other source during this period of temporary separation from their patient. These situations create and aggravate their anxiety. As the time for surgery prolongs, the anxiety levels of family members usually rises. Sometimes they may misinterpret what they don’t see during this period. Hence, they desperately need some help during this period to manage their anxiety and cope up with the situation.
The phenomenon of anxiety is infectious and it can incubate and spread very quickly to others and later on to the patient. Hence, reducing family members’ anxiety is crucial in order to enhance recovery and improve health of their patient. Imparting information is considered as an important and integral part of healthcare. Information about the current situation of their patient may help to eliminate family members’ anxiety. Information should be honest, comprehensive, easy to understand, and should be provided to the relatives without waiting for them to ask for it. This kind of information about the current status of patient’s health should be provided from time to time or at regular intervals to minimize the anxiety levels of family. However, numbers of hospitals in India do not have these additional support services, especially during the intra- operative period. Trained operation theatre nurse, medical professional or authorized and trained person can provide brief information about the patient’s current status to the family members during waiting period.
Theoretical Framework and Need for the Current Study
This study is based on two theories: 1. General system theory 2. Hildegard Peplau’s (1952) Interpersonal nursing theory.
A system consists of a set of interacting components within a boundary that filters the type and rate of exchange with the environment. Systems are composed of both structured and functional components. Structure refers to the arrangements of parts at a given time; function is the process of continuous change in the system as matter, energy and information are exchanged with the environment, for survival, all systems must receive varying types and amounts of matter, energy, and information from the environment. The system uses the input to maintain its equilibrium or homeostasis.
Anxiety is an energy that emerges in response to a perceived threat. Peplau (1973). described the sequence of steps in the development of anxiety as, holding expectations, expectations not met, discomfort felt, relief behaviours used and relief behaviours justified. Anxiety has been described as existing along a continuum including mild, moderate, severe, and panicky. Although it is possible to experience a state of no anxiety, this seldom occurs. As human beings, we constantly face a barrage of information and other stimuli that pose at least some minor threat to our self-views towards a situation. Peplau (1973). insisted that healthcare professionals must consider the current anxiety levels of their clients.
During personal experience, investigators had come across the anxiety expressed by family members during the intra-operative period. Before conducting this study, investigators observed family members waiting in the waiting room of operation theatre, and interacted with them to know their psychological status and needs. Investigators observed that family members were very tense and worried and a few of them cried during this waiting period. They looked anxious and confused. Family members of patients were observed to follow the surgeons, nurses, technicians and other staff who were coming out from the operation theatre, in the hope of getting feedback regarding the health status of their patient. It was expressed by almost all family members that they needed information about their loved one’s condition when the operation was going on. Family members’ minds are turmoil of doubts and queries which usually remain unanswered as family members are afraid to voice them. Investigators found that the barriers to intra-operative communication include lack of time, lack of attention, lack of support from management, lack of trained healthcare professionals, who can pass on the information to the anxious family members. This experience motivated investigators to study in details about anxiety states of family members and the measures to minimize them.
So, while applying above mentioned theories to the present study, investigators had planned interventions to reduce the anxiety mainly by providing information related to intra-operative period. Therefore, realistic perception of events by the family members and the psychological support given by the healthcare professionals bring positive adaptation, and reduce anxiety and help the family members to cope with the situation effectively.
Methodology
Quasi experimental Pre and post-test design was used for this study. The objective of the study was to compare anxiety of relatives from experimental and control group: in the beginning i.e. after the last eye to eye contact with the patient, and later when the patient was shifted to the recovery room at the end of the surgical procedure.
In this study, what we meant by “intra-operative information” was “the facts told about the patient’s health status during the intra-operative period.” This status report of the patient undergoing cardiac surgery with the permission and approval of the operating surgeon and the anesthetist usually lasted for 3-5 minutes. The intra- operative information included was:
i. Physiological status of the patient ii. Stage of the operation iii. The patient would be transferred to the recovery room after the surgery iv. They could visit the patient after the patient was shifted to the recovery room. The Investigator avoided mentioning specific time frames.
• Sample: Patients who were undergoing open heart surgery, either valve replacement or coronary bypass grafting, were focused and family members of these patients like father, mother, brother, sister, husband, wife, son, daughter were included in this study. Non probability convenience sampling of total 50 relatives (25 in each group - control and experimental respectively) who were above 18 years of age and who could understand and speak Hindi, Marathi or English and gave consent, were included. Investigator assigned first few weeks for relatives from control groups and later weeks for experimental group. This was done in order to avoid contamination of information among relatives during this study.
• Hypothesis:
H0 : There was no significant difference in the state anxiety of the relatives from both the groups.
H1 : At the end of the surgical procedure, there was a significant decrease in the state anxiety of the relatives from the experimental group.
• Tool:
a) Demographic data sheet: This sheet consisted demographic data of the patient’s family members who were in the waiting room during their patient’s surgery.
b) STAI inventory: Anxiety is subjective in nature, hence, self-reporting technique was used to obtain data related to state and trait anxiety of family members. State and trait anxiety inventory (STAI) form-Y1 and form-Y2 developed by Spilberger, were the most suitable one, hence chosen for obtaining data on anxiety of relatives in this study.
• Validity of tools: Demographic data sheet for relatives was subjected to “construct, content validity” along with its adequacy and relevance to the study. Validity was done by total 11 experts from surgery, nursing, psychiatry and psychology fields. STAI tool was translated into Hindi and Marathi languages. The validity of this tool was established by language experts followed by its retranslation into English language.
• Reliability of tools: Cronbach’s alpha for the STAI ranges from 0.92 to 0.94, hence, this tool was statistically reliable.
• Pilot study: A Pilot test was conducted on 5 family members from control and experimental group each after their consent. This Pilot study results were comparable with respect to the age, gender, educational status and operation done. The analysis showed that anxiety levels of relatives increased significantly towards the end of the operation, whereas it decreased in the experimental group. This Pilot study also confirmed that both the tools were reliable for this study.
• Ethical consideration: Informed verbal consent was obtained by relatives from the pilot study as well as the main study. Written permission was obtained by the hospital authorities and the ethical committee. Data was coded, and privacy and security of data was maintained throughout the study.
Data Collection for Main Study
All health personnel were informed from cardiothoracic operation theatre about the nature and the purpose of this study. Intra-operative information given by supporting staff was requested to be stopped during the study period to avoid dilution of information. Instead, one investigator was assigned to give information to the family members. Surgeons and other medical staff were informed about which time period was allotted for control and experimental weeks of the study.
After two hours of the last eye contact with the patient, family members were approached individually by the investigator and obtained demographic data from them. Later, form Y-1 followed by form Y-2 were duly filled by the family members. At the end i.e. immediately after the patient was shifted to the recovery room, the investigator requested them to fill the form Y-1 second time.
In the experimental group, the investigator gave intra- operative information for about 3-5 minutes three times i.e. at the beginning of the operation, in the middle of the operation and at the end of the operation i.e. immediately after the patient was shifted to the recovery room. Rest of the process remained the same for the experimental group i.e. filling up of forms Y-1 and Y-2. Above information is depicted in Table1 as conceptual framework for the study.
| Time | 2 hrs after the last eye contact with the patient | After Starting the surgery | Middle of the surgery | Immediately after the patient was shifted to the recovery room |
|---|---|---|---|---|
| Control group | ||||
| STAI Form Y-1 | Yes | NA | NA | Yes |
| STAI Form Y-2 | Yes | NA | NA | NA |
| Intra-operative information received | No | No | No | No |
| Holding expectations | Yes | Yes | Yes | Yes |
| Expectations met | No | No | No | No |
| Experimental group | ||||
| STAI Form Y-1 | Yes | NA | NA | Yes |
| STAI Form Y-2 | Yes | NA | NA | NA |
| Intra-operative information received | Yes | Yes | Yes | Yes |
| Holding expectations | Yes | Yes | Yes | Yes |
| Expectations met | Yes | Yes | Yes | Yes |
Table 1: Conceptual framework of the study.
NA= Not Applicable Table 1: Conceptual framework of the study.
Data Analysis
Demographic data of the patient and the family members was analyzed by using frequency and percentage. Comparison between control and experimental group was done with ‘t’ test and ‘chi square’ test. State and trait anxiety levels i.e. mild, moderate and severe anxiety levels were determined in Table 2 according the score. Minimum score for each form Y-1 and form Y-2 was 20 and maximum score was 80 hence mild anxiety level score ranged from 20-40, moderate anxiety levels 40-60 and severe anxiety level score ranged from 60-80.
| As a patient and as a caregiver | 20 | 20 | ||
|---|---|---|---|---|
| Mild | 20-40 | No experience | 28 | 36 |
| Moderate | 40-60 | |||
| Severe | 60-80 |
Table 3: Anxiety levels with score.
Results
Study sample consisted of 29 male and 21 female family members with a mean age of 39 years, ranging from 18 to more than 57 years of age; 9 were adult children of the patient, and the remaining family members were spouses (n = 16), siblings (n = 11), parents (n = 14). Of the participants; 6 were illiterate, 1 had completed primary education, 38 had completed secondary education and 5 were graduated. Table 3 shows that the majority of family members i.e. 72 percent from the control and 64 percent from the experimental group had previous experience of hospitalization either as a patient, as a care-giver or both.
| Previous experience of hospitalization of family members | Control group | Experimental group | |
|---|---|---|---|
| As a patient | 12 | 20 | |
| As a care-giver | 40 | 24 | |
| As a patient and as a care-giver | 20 | 20 | |
| No experience | 28 | 36 |
Table 2: Previous experience of hospitalization of family members.
(Scores are in percentages) Table 3: Previous experience of hospitalization of family members.
52 percent of family members from the control group had previous experience of surgery and 48 percent did not have any experience of surgery as reported in Table 4. In contrast, Table 4 also demonstrates that only 28 percent of family members from the experimental group had previous experience of surgery and 72 percent did not have any experience of surgery, so, it was their “first time waiting” for the loved one’s surgery.
| Previous experience of surgery of family members | Control group | Experimental group |
|---|---|---|
| As a relative of a surgical patient | 24 | 8 |
| Had undergone surgery himself/herself | 16 | 12 |
| Had both experiences - as a surgical patient and attendant relative as well | 12 | 8 |
| No experience | 48 | 72 |
Table 4: Previous experience of surgery of family members.
(Scores are in percentages) Table 4: Previous experience of surgery of family members.
Table 5 confirms no significant difference was found between the groups’ state and trait anxiety scores during pre-test. In contrast significant difference (t value = 8.76 and p value= <0.01) was found in the post-test state anxiety scores of the family members from both the groups. One relative refused to fill the form at the time of posttest hence n=24 for posttest.
| Control Group (N=25) | Experimental Group (N=25) | t value | df | P Value | Significance | |
|---|---|---|---|---|---|---|
| State anxiety- pre test | 51.4 (±11.56) | 53.92 (±12.03) | 0.74 | 48 | >0.05 | NS |
| Trait anxiety- pre test | 45.32 (±10.90) | 48.88 (±12.97) | 1.03 | 48 | >0.05 | NS |
| State anxiety-post test | 60.4 (±10.72) | 34.46 (±9.48) (N=24) | 8.76 | 47 | <0.01 | SD |
Table 5: Comparison of anxiety scores of family members from both the groups.
df= Degrees of Freedom NS= No Significant Difference SD= Significant Difference Table 5: Comparison of anxiety scores of family members from both the groups.
Table 6 and Table 7 illustrate that there was no significant difference between trait anxiety scores of relatives who had and who did not have previous experience of hospitalization. Post-test State anxiety scores of relatives from both the groups who did have (t value=6.43 and p value=<0.01) and who did not have previous experience of hospitalization (t value=5.55 and p value=<0.01) showed significant difference at the end of the surgery.
| Control Group (N=18) | Experimental Group (N=16) | t value | df | P Value | Significance | |
|---|---|---|---|---|---|---|
| State anxiety- pre test | 49.89 (±11.50) | 56 (±11.41) | 1.5 | 32 | >0.05 | NS |
| Trait anxiety - pre test | 45.39 (±10.90) | 49.5 (±10.48) | 1.08 | 32 | >0.05 | NS |
| State anxiety-post test | 59.5 (±10.72) | 36.4 (±8.97) | 6.43 | 31 | <0.01 | SD |
Table 6: Comparison of anxiety scores of family members who had previous experience of hospitalization.
df= Degrees of Freedom NS= No Significant Difference SD= Significant Difference Table 6: Comparison of anxiety scores of family members who had previous experience of hospitalization.
| Anxiety Assessment | Control Group (N=7) | Experimental Group (N=9) | t value | df | P Value | Significance |
|---|---|---|---|---|---|---|
| State anxiety- pre test | 55.14 (±11.68) | 50.22 (±12.90) | 0.74 | 14 | >0.05 | NS |
| Trait anxiety - pre test | 45.14 (±11.78) | 47.78 (±17.28) | 0.32 | 14 | >0.05 | NS |
| State anxiety-post test | 62.71 (±11.21) | 31.22 (±9.95) | 5.55 | 14 | <0.01 | SD |
| Anxiety Assessment | Control Group (N=13) | Experimental Group (N=7) | t value | df | P Value | Significance |
| State anxiety- pre test | 50.15 (±12.48) | 57.29 (± 8.32) | 1.29 | 18 | >0.05 | NS |
| Trait anxiety - pre test | 46.08 (±9.84) | 47.57 (±8.87) | 0.32 | 18 | >0.05 | NS |
| State anxiety-post test | 59.92 (±11.00) | 33.43 (±8.83) | 5.2 | 18 | <0.01 | SD |
Table 7: Comparison of anxiety scores of family members who did not have previous experience of hospitalization.
df= Degrees of Freedom NS= No Significant Difference SD= Significant Difference Table 7: Comparison of anxiety scores of family members who did not have previous experience of hospitalization.
Table 8 and Table 9 illustrate that there was no significant difference between trait anxiety scores of relatives who had and who did not have previous experience of surgery. Post- test State anxiety scores of relatives from both the groups who did have (t value=5.2 and p value=<0.01) and who did not have previous experience of surgery (t value = 6.43 and p value=<0.01) showed significant difference at the end of the surgery (Table 8 and Table 9).
df= Degrees of Freedom NS= No Significant Difference SD= Significant Difference Table 8: Comparison of anxiety scores of family members who had previous experience of surgery.
| Control Group (N=12) | Experimental Group (N=18) | t value | df | P Value | Significance | |
|---|---|---|---|---|---|---|
| State anxiety- pre test | 52.67 (±10.87) | 52.61 (±13.17) | 0.01 | 28 | >0.05 | NS |
| Trait anxiety- pre test | 44.5 (±12.35) | 49.39 (±14.46) | 0.93 | 28 | >0.05 | NS |
| State anxiety-post test | 60.92 (±10.87) | 34.88 (±9.97) | 6.43 | 27 | <0.01 | SD |
Table 8: Comparison of anxiety scores of relatives who did not have previous experience of surgery.
df= Degrees of Freedom NS= No Significant Difference SD= Significant Difference Table 9: Comparison of anxiety scores of relatives who did not have previous experience of surgery.
Figure 1 shows interesting findings regarding state anxiety levels of family members from both the groups at the beginning and at the end of the surgery. Figure 1 shows that family members from the control group experienced 16 percent mild and 64 percent moderate state anxiety score which decreased to 4 percent and 48 percent respectively during post-test period. In contrast, percentages of severe state anxiety score of relatives from the control group was doubled during post-test - i.e. from 20 percent, it rose to 48 percent. In figure 1, we also see an entirely different picture of the family members from the experimental group. There were 8 percent of relatives, who experienced mild state anxiety. This percentage increased to 60 percent during post-test. The number of relatives with moderate anxiety levels reduced from 56 percent in the pre-test to 36 percent in the post-test. Severe anxiety levels as experienced by the family members from the experimental group as noticed in the pre-test was observed to be alleviated during post-test period, that is to say, no relatives from experimental group experienced severe state anxiety levels during post-test.
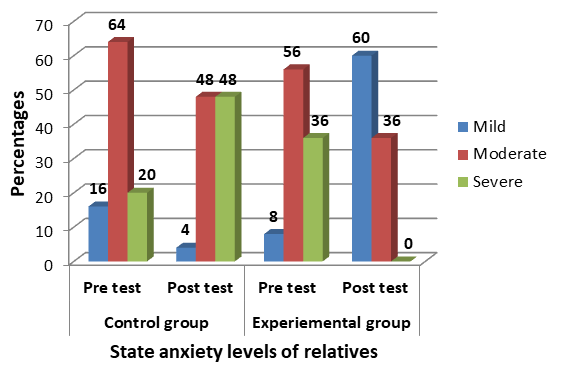
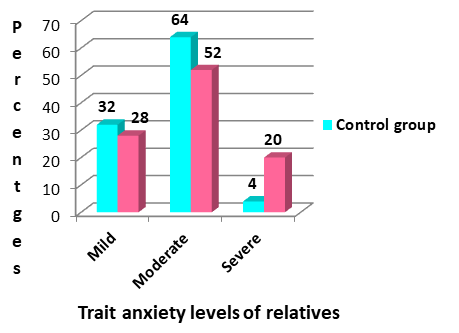
Figure 2 shows percentages of trait anxiety scores of family members from both the groups. Trait reveals overall nature of anxiety of that individual. It was important to compare trait anxiety with state anxiety, because trait affects how individual experiences situational anxiety i.e. state anxiety. Intra-operative period enhances situational anxiety among family members. Figure 2 reveals mild (32, 28), moderate (64,52) and severe (4,20) trait anxiety percentages of family members from the control group and the experimental groups respectively.
Discussion
The family members are anxious during intra-operative period in spite of variation in length and type of surgery [5] and this is irrespective of their nationality, cast and creed, age, gender, educational and socioeconomic status. Family is separated from the loved one for temporary period, but their need for the patient’s health-status information is greatly increased during this period. Number of studies confirmed this statement. For example, Carmody, et al. [6] revealed that family members expressed the need for this information as the highest priority during peri-operative period. Likewise Sayin, et al. [7] studied around 200 family members who expressed need for more intra-operative information.
Intra-operative waiting period is challenging for the family members. Trimm, et al. [2] reported balancing emotional equilibrium during waiting period was the main concern of the family members. Hence reducing anxiety is the need of the family members during intra-operative period. If these needs are not met with, their anxiety may be transferred to other family members during waiting period [8] as well as later to their patients. Family members are unable to provide required support to their patients after the surgery; because they are psychologically entangled in their own apprehension, anxiety, feeling of helplessness and desperation about patient’s health along with the outcome of surgery. They are struggling, fighting and seeking support from the hospital service providers to face such a situation.
This study confirms that providing intra-operative information helps the family members manage their anxiety during waiting period. Number of researchers support the findings of this study. For example, Eldridge, Ruth [4] reported that patients’ relatives were benefitted with intra- operative progress report during cardiac surgery. Likewise, Leske JS [1] conducted four group quasi-experimental post- test during intra-operative period. Results revealed that the group, who received “in-person progress report” about the patient’s health status, reported lower anxiety scores as compared to other three groups. Mi and Vasuki [9] stated that surgical progress reports via Short Message Service (SMS) reduced the anxiety of the family members during intra-operative period. Muldoon, et al. [8] issued “family care card” to 47 family members who were waiting during the surgical procedure on their loved ones. This card consisted information regarding the surgical procedure and estimated time, instructions for relatives during waiting period, instructions related to interactions with volunteers, and phone numbers for the contact. Muldoon, et al. [8] reported that majority (55percent) of the family members expressed that family care card helped them to reduce their anxiety during waiting period.
Trecartin, et al. [10] studied 151 family members waiting during invasive cardiac procedures on their loved ones. This was a study conducted on three groups, i.e. Group 1 (50 family members who received standard of care), Group 2 (50 family members who received standard of care and informational report), Group 3 (51 family members who received standard of care and informational report and were allowed post procedure visit). State anxiety was lowest in the Group 3. State anxiety was lesser in the Group 2 (who received informational report) as compared to the Group 1 (who received only standard of care).
Conclusion
The findings of our study are in line with other researchers who examined the anxiety levels of families during intra-operative period. Our study suggests that situational support given to the family members helps to reduce their anxiety levels during intra-operative period. Such practices of giving intra-operative information to family members should be inculcated as a routine practice in any hospital around the world.
Acknowledgment
Authors express gratitude to all patients’ family members and the hospital for permission to conduct this research study.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
References
-
Leske JS (1996) Intraoperative progress reports decrease family members’ anxiety. AORN Association of perioperative Registered Nurses Journal 64(3): 424-436.
-
Trimm DR, Sanford JT (2010) The process of family waiting during surgery. Journal of family nursing 16(4): 435-461.
-
Stefan KA (2010) The nurse liasion in perioperative services: A family- centered approach. AORN Journal 92(2): 150-157.
-
Eldridge R (1984) Surgery progress reports- support for cardiac surgery patients’ families. AORN Journal 40(2): 241-246.
-
Leske JS (1993) Anxiety of elective surgical patient’s family members- relationship between anxiety levels, family characteristics. AORN Journal 57(5): 1092-1103.
-
Carmody S, Hickey P, Bookbinder M (1991) Perioperative needs of families. AORN Journal 54(3): 561-567.
-
Sayin Y, Aksoy G (2012) The nurse’s role in providing information to surgical patients and family members in Turkey: A descriptive study. AORN Journal 95(6): 772- 787.
-
Muldoon M, Cheng D, Vish N, DeJong S, Adams J (2011) Implementation of an informational card to reduce family members’ anxiety. AORN Journal 94(3): 246-253.
-
Mi KJ, Vasuki R (2017) The effects of providing surgical progress information using SMS on satisfaction of nursing needs and state anxiety of patients’ family. IOSR Journal of Nursing and Health Science 6(2): 48-56_._
-
Trecartin K, Carroll D (2011) Nursing Interventions for family members waiting during cardiac procedures. Clinical Nursing Research 20(10): 1-13.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda