Indian Hospitals See Two More ‘Invasive White Fungal Infections’ Raising New Health Concerns in Covid 19- Second Phase in 2021
The years 2020 & 2021 will go in the history of World Public Health as the year of Covid 19 Pandemic. So will the Invasive fungal infections (IFI) complicating Covid 19 patients during and after recovery due to Black, White and Yellow Fungi are engraved in Indian Public Health history. IFI became a leading cause of vision or eye loss, facial disfigurement, and Pulmonary and other organ infections. Union Health Minister, GOI, reported to the Parliament on 3 December 2021 that a total of 51,775 cases of mucor mycosis have been reported in the country till 29/11/2021 but did not give the breakup of while fungus among them indicating lack of reporting and monitoring of sub-varieties of fungal infections. Invasive fungal disease (IFD) is an important complication in immunocompromised patients. The frequency of IFD has increased in correlation with growth in populations of cancer, immunocompromised hosts, and patients with HIV infection, organ transplantation and autoimmune diseases. In India, the rare fungal infection occurred among organ transplant cases. Even before Covid 19 Pandemic it disproportionately affected Indian patients, with the prevalence of the infection about 70 times higher in India than the rest of the world. Several cases of Mucor mycosis, aspergillosis, and candidiasis, linked to immunosuppressive treatment for COVID-19 were reported during the COVID-19 pandemic in India in 2020 and 2021. The number of cases has increased a lot that has led to prolonged morbidity and mortality in COVID-19 patients during illness and up to 3 months after recovery. The cases of White Fungus or Aspergillosis were detected in Bihar, Madhya Pradesh, Andhra Pradesh, and Uttar Pradesh starting mid-May 2021 in India. Fortunately, they are amenable to medical treatment and cause minimal damage and fatality. This article is an analysis of cases of Invasive white Fungus Infections reported in the country. Material & Methods: GOI reports on IFI to the Parliament, Local hospital press releases in metropolitan and major cities.
Introduction
The years 2020 & 2021 will go in the history of Global Public Health as the year of SARS Cov 2 virus (Covid 19) disease. So will the Invasive fungal infections (IFI) complicating Covid 19 patients during and after recovery due to Black, White and Yellow Fungi be engraved in Indian Public Health history. Union Health Minister, GOI reported to the Parliament on 3 December 2021 that a total of 51,775 cases of mucor mycosis have been reported in the country till 29/11/2021. However, an informal collation by states indicates this number can be over a million cases, out of which only 5% are due to white fungus. Five states of Maharashtra, Gujarat, Rajasthan, Karnataka, and Andhra Pradesh contribute nearly two thirds of the cases & deaths [1]. We also know that a unified portal was created by the ministry for states to enter surveillance data of Mucor mycosis cases, during second phase of Covid 19 Pandemic in April 2021. Invasive fungal disease (IFD) is an important complication in immunocompromised patients. The frequency of IFD has increased in correlation with growth in populations of cancer, immunocompromised hosts, and patients with HIV infection, organ transplantation and autoimmune diseases. Black, White and Yellow fungus infections are caused by fungi or moulds, called ‘mucoromycetes (MM). In India, the rare fungal infection is known to occur among organ transplant cases, Cancer patients for decades. For times immemorial IFD disproportionately affected Indian patients, with the prevalence of the infection about 70 times higher in India than the rest of the world [2].
White and Yellow fungi belong to the family of candida that can affect lungs, stomach and intestines, nails, brain, skin and even genitals. Fortunately, they are amenable to medical treatment, unlike the Black fungus that most commonly infects the nose, sinuses, eye, and brain (Sino-orbital) resulting in a runny nose, one-sided facial swelling and pain, headache, fever, blurred vision, bulging or displacement of the eye (proptosis), and tissue death. Disfigurement of the face is a major, lifelong consequence among survivors [3, 4, 5, 6]. The number and proportion of cases of Mucor mycosis, Aspergillosis, and Candidiasis, linked to immunosuppressive treatment for COVID-19 were increasingly reported since the beginning of COVID-19 pandemic in India in March 2020 till today. In the second wave of coronavirus disease in April-July 2021 after enormous increase in Covid 19 cases, IFD cases increased a lot and that has led to prolonged morbidity & mortality in COVID-19 patients.
The cases of White Fungus or Aspergillosis were detected in Bihar, Madhya Pradesh, Andhra Pradesh, and Uttar Pradesh starting mid-May 2021 in India. Invasive aspergillosis or white fungus or is a post-Covid complication in which the infection goes to the lungs and causes pneumonia. Invasive aspergillosis is a rapidly progressive, often fatal infection that occurs in patients who are severely immunosuppressed because of steroidal drugs they was administered to fight the coronavirus disease. Aspergillus is a common mould infection that lives indoors and outdoors. Most people inhale Aspergillus spores every day without getting sick. But people with a weakened immune system or lung disease are at a higher risk of developing health issues due to Aspergillus. The problems caused by Aspergillus include allergic reactions, infection in body organs including lungs. If detected at an early stage, the infection can be treated only by taking medication. In severe case, if the infection spreads to other parts of the body the person must undergo surgery. The treatment for aspergillosis is Amphotericin injections the same as black and white fungus [7].
Review of White Fungus Cases Reported in India in 2021
• Ghaziabad, Uttar Pradesh: Out of a total 26 IFD cases seven (27%) recovering COVID-19 patients were diagnosed with invasive aspergillosis, a severe form of white fungus infection in May 2021. At least three (11%) patients in the district had developed both black and white fungal infections. White fungus in the patients was confirmed based on histopathology reports. These infections had developed in the post-Covid stage after 15-30 days and after of testing negative for Covid 19. The white fungus has only one mode of treatment – through Amphotericin injections as parts of the lungs cannot be taken out like Black fungus infections that can be operated upon (debridement, enucleation of eye or mandibular reconstruction, and fungal mass taken out from the affected parts mainly Sino-orbital-cerebral mucor mycosis. While patients were administered Amphotericin injections, and Posaconazole (is effective in cases of white fungus only and is easily available) injections and tablets. All seven patients suffering white fungus had mild to moderate symptoms and recovered fully [8] (Figure 1).

- Jabalpur, Madhya Pradesh: A 55-year-old man was operated (Nose and sinus debridement) on 17 May 2021 after complaining of persistent headache and eye pain by the head of the ENT department at government-run Netaji Subhash Chandra Bose Medical College hospital in Jabalpur, Madhya Pradesh. A pathological test on 21 May 2021 revealed that he had white fungus in the nose and sinuses. He had recovered from COVID-19 two weeks ago. MP had reported 650 confirmed cases of black fungus so far and only about 10 cases of White Fungus as of 22 May 2021 [9].
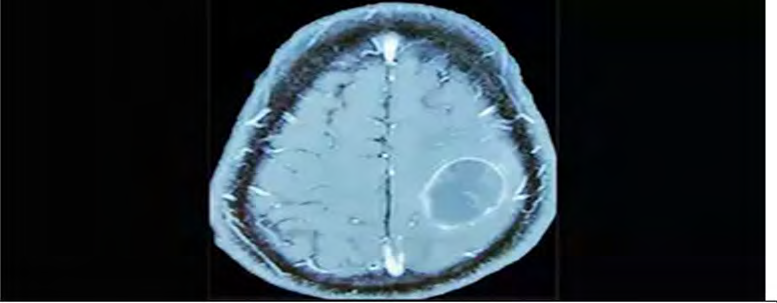
- Hyderabad, AP: A patient complained of weakness in limbs and difficulty in speech on the sixth day of his admission. The patient was hypertensive but not diabetic. An initial MRI of the brain revealed a large lesion in the left part along with two small lesions in different parts. He was treated for Haematoma that did not change and more symptoms were becoming clear, therefore a repeat MRI with contrast was done. That showed that the big lesion had increased in size with dense and well-defined margins & smaller lesion remained unchanged. Following a surgery, the doctors found a well-encapsulated abscess containing soft necrotic material, separate from normal brain. A pathological analysis of the abscess found it to be a case of white fungus infection, due to Aspergillosis. Aspergillosis of the central nervous system is a result of the invasion of the brain blood vessels by white fungus. The fungus can enter the brain either through inhalation of spores into the lungs from where they enter the blood stream, or directly through nose to the brain [10, 11] (Figure 2).
• Patna, Bihar: Four patients admitted to the hospital in Patna, Bihar Corona-like symptoms but the corona report of all those patients has been negative. Professor and head of department of microbiology at the PMCH, reported the four cases of white fungus. after identifying after a high-resolution computed tomography was performed on the infected patients. One of the patients was a doctor himself, who was treated in a private hospital after showing symptoms of COVID-19, but he tested negative for COVID-19 RTPCR test though his lung was infected. All patients were subjected to a fungus culture test of their phlegm or mucus that confirmed the diagnosis [12, 13].
- Bengaluru Karnataka: Bowring and Lady Curzon Medical College Hospital, Bengaluru which has treated more than 140 patients with mucor mycosis, after cell culture tests have confirmed that only 5% of cases were of Aspergillus Niger, and Candida albicans while in 95% of the cases the presence of Mucor mycosis. A Pulmonologist, Apollo Hospitals, Bengaluru reported that Apollo Hospitals saw 10-15 aspergillosis patients over the few weeks in May 2021 caused by inhaling aspergillus spores. In multiple cases, B&L Curzon hospital had seen the presence of all three fungi. However, Mucor mycosis was most invasive and fatal compared to Aspergillus Niger and Candida albicans, HCG hospital, Bengaluru had seen two cases of triple fungal infections and multiple cases with both Mucor mycosis and Aspergillus Niger. Trust well hospital, who has been treating mucor cases, has also seen super added infections of Aspergillus Niger and Candid Albicans [14, 15, 16].
- Vadodara, Gujarat: Doctors in Vadodara have reported 8 cases of a new fungal infection called aspergillosis on 29 May 2021. Pulmonary aspergillosis infection was observed in people who have compromised immunity. Sinus and pulmonary aspergillosis, observed right now in COVID patients, is rare. Aspergillosis is not as deadly as the black fungal infection, but it too can be fatal [12, 13].
Epidemiology
Aspergillus is the second commonest pathogens other than mucor mycosis causing deadly fungal infections. Infection is typically caused by Aspergillus fumigatus (90%), Aspergillus flavus, nidulans, s terreus, and Aspergillus versicolor. They cause a wide range of white fungus infections like Invasive Pulmonary Aspergillosis (IPA), Chronic Pulmonary Aspergillosis (CPA), Allergic Broncho- Pulmonary Aspergillosis (ABPA), chronic rhinosinusitis, fungal asthma, and Aspergillus bronchitis, Cold abscess in brain etc. It has been found in the second phase of Covid 19 during April-October2021 that up to 40 % of covid-19 hospitalized patients developed severe ARDS and become more susceptible to acquire co-infections caused by bacteria, viruses, or fungi Mode of contamination occurs through the inhalation of fungal spores. CAPA developed during the following weeks, and the risk increased for superinfections by anti-IL-6-receptor treatment for covid-19 or corticosteroid treatment for underlying conditions [17].
Pathogenesis
Association between covid-19 and aspergillosis: The highly elevated level of serum IL-6 and IL-10 are suspected to lead to disease progression as increased production of IL-10, mediates the influx of phagocytic cells, which can limit the extent of local tissue destruction of Aspergillus infection. Greater Th-2 (T helper type 2) cells responses that are the increase of IL-10 or lesser Th-1(T helper type 1) cells responses, down-regulate macrophage responses, and increase host susceptibility to deadly Aspergillus infection. IL-6 is a multi-functional cytokine, and it plays an important part in protective immunity against Aspergillus. After Aspergillus fumigatus infection, there is a significant increase in the amount of IL-6. Reduced responsiveness is exhibited of T cells to IL-6 in patients with IPA. Covid-19 patients with CRS show excessive IL-6 signalling which leads to numerous biological effects such as increasing vessel permeability, ARDS, cardiac arrhythmia, and reducing myocardial contractility [12, 13, 16, 17].
Discussion
Since the start of the COVID-19 pandemic, outbreaks of C. Auris have been reported in COVID-19 units of acute care hospitals in USA. Patients hospitalized for COVID-19 were at risk for healthcare-associated infections (HAIs), including candidemia, or bloodstream infections caused by Candida, infections resistant to antifungal. Early diagnosis and monitoring for Candida infections and antifungal resistant infections (e.g., C. Auris, azole-resistant Aspergillus) are key to reducing death from COVID-19 in patients with severe COVID-19 fungal co-infections [18]. Acute respiratory distress syndrome (ARDS) has emerged as an important disease that predisposes patients to secondary pulmonary aspergillosis, with 35 cases of COVID-19 associated pulmonary aspergillosis (CAPA) published until June 2020. Diagnosis of CAPA remains challenging, mainly because bronchoalveolar lavage fluid galactomannan testing and culture, which represent the most sensitive diagnostic tests for aspergillosis in the ICU, are hindered by the fact that bronchoscopies are rarely performed in COVID-19 patients due to the risk of disease transmission.
Aspergillosis has been increasingly reported in patients without weakened immune systems but who have had severe respiratory infections caused by viruses, including influenza. Several recent reports describe COVID-19-associated pulmonary aspergillosis (CAPA). Scientists are still learning about aspergillosis in people with severe COVID-19 and available evidence that CAPA, a) usually occurs in patients with severe COVID-19 (e.g., patients on ventilators in ICUs), b) is difficult to diagnose because patients often have non- specific symptoms and testing typically requires a specimen from deep in the lungs and c) can cause severe illness and death. Coronavirus disease 19 (COVID-19)-associated pulmonary aspergillosis (CAPA) emerged as important fungal complications in patients with COVID-19-associated severe acute respiratory failure (ARF). Whether mould active antifungal prophylaxis (MAFP) can prevent CAPA remains elusive so far. In an observational study, of all consecutive patients admitted to intensive care units with COVID-19- associated ARF between September 1, 2020, and May 1, 2021, 132 patients, of whom 75 (57%) received antifungal prophylaxis (98% Posaconazole). Ten CAPA cases were diagnosed, after a median of 6 days following ICU admission. Of those, 9 CAPA cases were recorded in the non-prophylaxis group and one in the prophylaxis group, respectively. However, no difference in 30-day ICU mortality could be observed. Thirty-day CAPA incidence estimates were 1.4% (95% CI 0.2–9.7) in the MAFP group and 17.5% (95% CI 9.6– 31.4) in the group without MAFP (p = 0.002). The respective sub distributional hazard ratio (sHR) for CAPA incidence comparing the MAFP versus no MAFP group was of 0.08 (95% CI 0.01–0.63; p = 0.017). The study concluded that in ICU patients with COVID-19 ARF, antifungal prophylaxis was associated with significantly reduced CAPA incidence, but this did not translate into improved survival [19, 20].
Bowring and Lady Curzon Medical College Hospital, Bengaluru which had treated more than has seen 500 mucor mycosis cases so by June 2021 of whom, 252 patients had undergone surgeries and 59 had died. Of the 140 patients with mucor mycosis, after cell culture tests have confirmed in 95% of the cases the presence of Mucor mycosis, and remaining 5% only, showed Aspergillus Niger, and Candida albicans. antifungal drug Liposomal Amphotericin B is the main drug of choice for the treatment. It costs about INR 7000 /dose vial and on an average patient requires 5-8 doses per day for 10-14 days, an overall cost of 1.5 Lakhs.
Conclusion
The number of cases of Mucor mycosis, Aspergillosis, and Candidiasis, linked to immunosuppressive treatment for COVID-19 were increasingly reported since the beginning of COVID-19 pandemic in India in March 2020 till today. There are no official data on white fungi cases in the country, however, collation from various cities press reports one estimate that about 5% of cases are of white fungi like Aspergillus Niger, Candida Albicans contribute about 5% of total Mucor Mycosis cases in India. Fortunately, they are amenable to medical treatment and cause minimal damage and fatality.
References
-
(2021) 51,775 cases of mucormycosis reported in India: Health Minister Mansukh Mandaviya. India Today.
-
Sharma A, Tanwar S, Asija R, Agarwal R (2021) Fungal infections associated with covid-19. International Journal of Pharmacy and Pharmaceutical Sciences 13(10): 12-19.
-
Baruah C, Devi P, Deka B, Sharma DK (2021) Mucor mycosis and Aspergillosis have been Linked to Covid-19- Related Fungal infections in India. Adv Case Stud 3(1): 1-4.
-
Skiada A, Pavleas I, Apiranthitou MD (2020) Epidemiology and Diagnosis of Mucor mycosis: An Update. Journal of Fungi 6(4): 265.
-
Singh AK, Singh R, Joshi SR, Misra A (2021) Mucor mycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab Syndr 15(4): 102146.
-
Sen M, Honavar SG, Sharma N, Sachdev MS (2021) COVID-19 and Eye: A Review of Ophthalmic Manifestations of COVID-19. Indian J Ophthalmol 69(3): 488-509.
-
Chander J (2018) Textbook of Medical Mycology. In: 4th (Edn.), Jaypee Brothers Medical Publishers Ltd, New Delhi, India, pp: 534-596.
-
(2021) Now, Ghaziabad hospital reports 7 cases of ‘white fungus’ infection. Hindustan Times.
-
(2021) MP: White fungus case reported in Jabalpur, doctor says it’s common & curable. India Today.
-
Akbar S (2021) White fungus abscess found in recovered Covid patient’s brain. Times of India.
-
(2021) Aspergillosis: After black, white, and yellow fungus, cases of aspergillosis, a new fungal infection reported. Times of India.
-
Khan MI (2021) After black fungus, white fungus cases reported in Bihar amid COVID-19. Down to Earth.
-
Yamin HS, Alastal AY, Bakri I (217) Pulmonary Mucor mycosis Over 130 Years: A Case Report and Literature Review. Turk Thorac J 18(1): 1-5.
-
Rao SR (2021) Not mucor alone, Bengaluru hospitals see two more fungal infections. The Times of India.
-
Ravindra K, Ahlawat A (2021) Five probable factors responsible for the COVID-associated Mucor mycosis outbreak in India. Int J Infect Dis 112: 278-280.
-
Rao SR (2021) 70% Mucor mycosis cases in Karnataka still under treatment. The Times of India.
-
Arastehfar A, Carvalho A, Veerdonk FL, Jenks JD, Koehler P, et al. (2020) COVID-19 Associated Pulmonary Aspergillosis (CAPA)-From Immunology to treatment. J Fungi (Basel) 6(2): 91.
-
Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, et al. (2005) Epidemiology and outcome of zygomycotic: a review of 929 reported cases. Clinical Infectious Diseases 41(5): 634-653.
-
Hurtado R (1965) Cerebral Mucor Mycosis 93(4): 179‐182.
-
Hatzl S, Reisinger AC, Posch F, Prattes J, Stradner M, et al. (2021) Antifungal prophylaxis for prevention of COVID- 19-associated pulmonary aspergillosis in critically ill patients: an observational study. Critical Care 25: 335.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda